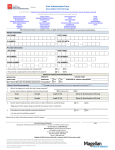
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
AAHAM Music City Chapter Conference September 26, 2013 Tennessee Plan for Payment Reform • State hired Mckinsey and Company • Modeling program after Arkansas Health Care Payment Improvement Initiative – Retrospective bundled payments – Primary care medical home • Will begin with TennCare and State employees • Goal to have majority of “healthcare spend” based on episodes and population-based payments within next three to five years Tennessee Plan for Payment Reform • Episode based payments – Reward one or more providers for total performance, specific event, procedure or treatment of condition – Episodes will cover a specific pre-defined period during which patients receive care from multiple providers – Each episode has a “quarterback” • Leads and coordinates all providers involved in care • Helps drive improvement • Pre-determined with episode definition and may be physician or hospital – Episodes are “triggered” by hospital inpatient or outpatient procedure or encounter Tennessee Plan for Payment Reform • Retrospective episode-based payments – Providers receive reimbursement from payers based on usual negotiated rates as they currently do – Quarterback receives rewards or penalties based on overall cost of episode • Commendable and acceptable levels of cost determined based on retrospective cost data • Calculate risk-adjusted average cost per episode for the total patient population served during the performance period for the episode • Share savings if average cost below commendable level • No change in payment if average cost between commendable and acceptable • Pay portion of excess costs if costs exceed acceptable Tennessee Plan for Payment Reform • Three initial episodes selected – Total Joint Replacement • Greatest impact for state employee population • Orthopedic surgeon will be quarterback – Asthma Exacerbation • Hospital will be quarterback – Perinatal • Obstetrician or Family Practice physician will be quarterback Tennessee Plan for Payment Reform • MCOs to start providing data to quarterbacks January 2014 • Additional episodes rolled out in batches every 3 to 6 months • Within 3 to 5 years episodes and population based payment models account for majority of healthcare spend Year 2 TennCare Rate Variation • Aon on track to complete the analysis by October – New data could result in minor changes to bands for Year 2 in order to maintain budget neutrality • When final percentages are available, TennCare will host a webinar for all hospitals – THA will send impact information to all hospitals • TennCare bureau will review MCO contract amendment language and contract negotiations should begin in November • No changes will be implemented until all contract amendments have been signed – Amendments will be retroactive to July 1, 2013 Transition of CoverKids to TennCare • On July 30, Blue Cross notified providers CoverKids and pregnant women in HealthyTNBabies would be using the TennCare Select network, effective October 1 – These groups previously used the state employee network • Contract amendment placed providers serving those populations into the TennCare Select network at existing TennCare Select rates • Change was automatic unless provider notified Blue Cross in writing of rejection prior to August 29 Transition of CoverKids to TennCare • The Blue Cross communication states “CoverKids program and HealthyTNBabies program members are not TennCare Select Members” • THA requested clarification from the TennCare bureau on several issues not communicated by Blue Cross – Kids age 6 through18 under 138% of poverty required by the ACA to be moved into Medicaid • Will be implemented beginning January 2014 • Still discussing with CMS whether move will be all at once or at time of recertification • Unclear if they will stay in TennCare Select or be auto-assigned to MCO Transition of CoverKids to TennCare • Women in HealthyTNBabies who were pregnant and under the care of an OB on October 1, 2013 could stay with that OB – OB would be reimbursed under the previous rate • 100 percent Medicare bump will be implemented for doctors that saw kids age 6 through 18 under 138 percent of poverty – Will receive increased payment for selected E&M codes • State does not have spending authority to fund interim payment increase for physicians or hospitals – Agreed to increase all TennCare Select rates effective July 1, 2014 funded by hospital assessment TennCare Benefit Changes • Beginning October 1, 2013 – TC won’t cover • Facets injections • Allergy medicine of any kind • TENS services for chronic lower back pain – These will have limits: • Trigger point injections – only pay for 4 trigger point injections in each muscle group every 6 months TennCare Benefit Changes • Limits, con’t: – Epidural Injections – only pay for 3 epidural shots every 6 months – Urine Drug Screenings – Only pay for 12 urine drug screenings per year • All of above apply to add adults 21 or older TennCare Benefit Changes • Starting October 1 – There will be a $1.50 co-pay for generic prescriptions • Applies if member currently pays a $3 co-pay for brand name prescriptions • Does not apply if member is in CHOICES Group 1 or CHOICES Group 2 – For drugs within member’s monthly limit, won’t pay co-pay for TennCare Benefit Changes • For drugs within member’s monthly limit, won’t pay co-pay for: • Birth control • Medicine received in hospice care • Medicine received in a medical emergency (in the ED) • Medicine member takes while pregnant (ex. vitamins) Insurance Exchange Insurance Exchange Enrollment Opportunity Three-fourths of the uninsured live in 16 states CA TX FL NY GA IL NC OH PA NJ MI AZ VA TN WA IN Data provided by Baptist Healing Trust 16 Expansion Population • Because Medicaid has not been expanded in Tennessee, there will be a donut hole • Those below 100% of federal poverty level AND who do not qualify for Medicaid today are NOT ELIGIBLE FOR THE EXCHANGE • They will have not have access to any health insurance 17 Affordable Care Act includes: • Insurance requirements & regulatory changes • Tax credits and cost-sharing subsidies • Individual mandate/penalties • Establishes essential health benefits 18 QHP Plan Levels of Coverage Levels of Coverage Plan Pays On Average Enrollees Pay on Average* (In addition to the monthly plan premium) Bronze 60% 40% Silver 70% 30% Gold 80% 20% Platinum 90% 10% *Based on the aggregate cost under the plan when benefits are provided to a standard population. This may not be the same for every (or any specific) enrolled person. 19 Enrollment Periods • Initial open enrollment period: October 1, 2013 through March 31, 2014 • Annual open enrollment periods will be October 15 – December 7 in succeeding years • Special enrollment periods available in certain circumstances during the year 20 Initial Open Enrollment Period for the Individual Market October 1, 2013 – March 31, 2014 Enroll during the initial open enrollment period • On or before December 15, 2013 • Between the 1st and 15th day of January – March • Between the 16th and the last day of December - March Coverage is effective • January 1, 2014 • First day of the following month • First day of second following month 21 Apply Online, By Phone or In Person 1. Enter basic information Healthcare.gov has checklist 2. Choose level of coverage 3. Compare health plans 4. Confirm plan selection 5. Apply for coverage Exchange verifies information/determines eligibility 6. Pay first month’s premium 22 New Rules • Cannot be denied coverage • Modified community rating (only can adjust premium for age, tobacco & geography; cannot adjust for gender or health status) • Mandated coverage of 10 essential health benefits determined by HHS 23 Essential Health Benefits – – – – – – – – – – Ambulatory patient services Emergency services Hospitalization, maternity and newborn care Mental health & substance use disorder services, including behavioral health treatment Prescription drugs Rehabilitative & habilitative services & devices Laboratory services Preventive & wellness services Chronic disease management Pediatric services (including oral & vision care) 24 Exchange Eligibility • Marketplace eligibility requires consumer to: – Live in its service area AND – Be a U.S. citizen or national OR – Be a non-citizen who is lawfully present in the U.S. for the entire period for which enrollment is sought – Not be incarcerated 25 Consumer Assistance • Applicant may be eligible for two forms of assistance to afford coverage in the health insurance marketplace: – Premium tax credits – Cost-sharing subsidies 26 Premium Tax Credit • Eligibility for the premium tax credit is based on: – Household income and family size (previous year end) – Income between 100% to 400% of the federal poverty level • $23,550 - $94,200 for family of four in 2013 – Not eligible for government-sponsored coverage or affordable employer-sponsored insurance 27 Premium Tax Credit • Amount of the premium tax credit depends on: – Actual household income as a percentage of the federal poverty level and family size – The premium for the second lowest cost silver level qualified health plan, adjusted for the age of the covered person – A sliding scale that increases the taxpayer’s own contribution towards the premium cost as income increases 28 Cost-Sharing Reduction • Cost-sharing subsidies for those that receive premium tax credit – People with income between 100% and 250% of federal poverty level • Federal government shares in cost of co-pays and deductibles • Silver plans only 29 Resources & Training 30 National Consumer Information • Provider-focused website – www.marketplace.cms.gov • CMS consumer-focused website • www.HealthCare.gov • 24-hour CMS consumer call center for the individual exchange • • • • 800-318-2596 1-855-889-4325 (TTY) Now providing general information Starting 10/1/13 – eligibility & enrollment assistance 31 Outreach Efforts for Enrollment • Important terms to understand: – Navigators receive funding from CMS to conduct outreach. • There are two in Tennessee: – Structured Employment Economic Development Corporation (SEEDCO) – Tennessee Primary Care Association – Certified application counselors (CACs) are trained individuals who provide consumer enrollment assistance. They are accredited by CMS, but are not funded by CMS. – Certified Enrollment Entity (CEE) is a designation hospitals must apply for and be granted by CMS before their employees can be trained and accredited CACs. http://marketplace.cms.gov/help-us/cac-apply.html 32 CAC Training • CAC training modules are posted online at the health insurance marketplace • Remember, your organization must first be a registered CEE in order for employees to complete the training • Modules are available at: http://marketplace.cms.gov/training/get-training.html CAC Training • CMS backlog with CAC application responses • CMS Consumer Support team has established the following email address for CAC-related questions: [email protected]. – Include the organization name – and topic in subject line – and be sure to include contact info with email • TDCI Emergency Rules • Last week, the Tennessee Department of Commerce & Insurance (TDCI) released emergency rules (http://state.tn.us/sos/rules_filings/09-29-13.pdf) requiring registration for navigators and certified application counselors for the new health insurance exchange. TDCI Emergency Rules • The department also has released: – FAQ 1 Offering educational information • (http://www.tn.gov/insurance/documents/9_20NavigatorFAQ1.pdf) – FAQ 2 Application forms, fingerprinting and background check requirements (http://www.tn.gov/insurance/documents/9-20NavigatorFAQ2.pdf) - Registration requirements and application for navigator or certified application counselor (CAC) ENTITY (http://www.tn.gov/insurance/documents/navigator_entity_packet_2013.pdf) - Registration requirements and application for navigator or certified application counselor INDIVIDUAL (http://www.tn.gov/insurance/documents/navigator_individual_packet_2013.pdf) Insurance Exchange Enrollment • Enrollment of uninsured critical issue for hospitals • CMS navigator grant for Tennessee exchange enrollment only $1.4 million • Tennessee hospitals saw 345,000 uninsured individuals in EDs in 2011 (out of 889,000 uninsured statewide) • THA will make $3 million of grant funds available to hospitals – Grant amounts will be based on the level of uninsured each member facility serves in the ED – The minimum grant amount would be $10,000 37 THA Grants • $3 million in grants available to acute care and research hospitals who are THA members • Grant amounts will be based on 2011 JAR uninsured ED volume • Deadline for application is Oct. 31, but applications will be funded as they are received • Criteria and details in package emailed to CEOs • Questions: email [email protected] THA Grants • Grant information/application sent to hospital CEOs – Acute care hospitals – Hospital systems containing acute care hospitals OR – Research hospitals • System hospitals may apply individually or as a system • Approved grant uses will be flexible so they can be tailored to your community 39 THA Grants • Include (but not limited to): – Salary/benefit costs of hospital staff (or temporary staff) to become certified as CACs (explain health coverage options to uninsured & assist with enrollment) – Independent contractor fees to provide or assist with community education – Cost to print educational materials – Cost to analyze hospital data for a targeted campaign effort 40 THA Grants • Partnering with not-for-profit organizations that specialize in working with populations that lack insurance. Examples include: – Project Access – Tennessee Health Care Campaign • Partner with local insurance agents/brokers to work with uninsured individuals 41 THA Grants • Quarterly reports will be required to include successes & obstacles so hospitals can learn from each other • THA will provide exchange resource materials • Questions: email [email protected] 42 THA Resources • THA website – Resource guide for Tennessee hospitals – List of Tennessee agents/brokers who have committed to assist individual exchange applicants – THA grant information – Sample hospital application – THA grant application – Webinar/audio recording 43 THA Resources • Materials hospitals can customize and use locally – Brochures – Posters – Tent Cards – Stickers 44 Questions? 45