Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
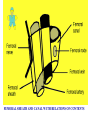
HERNIAS MOSTAFA ABOU ALI PROFFESSOR OF SURGERY QASSIM UNIVERSITY FACULTY OF MEDICINE HERNIAS..DEFENITIONS • Hernia is a protrusion of an organ through the wall that normally contains it • The wall can be the abdominal wall, muscle fascia, diaphragm or foramen magnum. • Hernias can be congenital or acquired • Abdominal wall hernias are common • Account for approximately 10% of general surgical workload • Types Inguinal 73% femoral 17% umblical 8.5 % rare forms 1.5% ( incisional hernia is excluded.) A HERNIA CONSISTS OF : • A sac • Its coverings • Its contents ( all abdominal viscera except liver and pancreas). ABDOMINAL REGIONS WHERE HERNIAS OCCUR HERNIAS…ETIOLOGICAL FACTORS Acquired hernias: • Increased intra-abdominal pressure (e.g. straining or lifting ) • Abdominal weakness (e.g. advancing age or malnutrition) ANATOMY OF THE INGUINAL CANAL • Anterior border is the external oblique aponeurosis • Posterior border is the transversalis fascia • Inferior border is the inguinal ligament • Superior border is the conjoint tendon the lower fibers of internal oblique and transversus abdominis ANATOMY OF INGUINAL CANAL Inguinal canal lies between the superficial and deep inguinal rings Deep ring lies deep to the mid-inguinal point Mid-inguinal point is half way between symphysis pubis and anterior superior iliac spine Not the midpoint of the inguinal ligament In men it contains vas deferens and testicular artery and veins In women it contains the round ligament INGUINAL HERNIAS…INCIDENCE. • 3 %adults will require operation for inguinal hernia • Male : female ratio is 12:1 • Elective : emergency operation 12:1 • Peak incidence is in the 6th decade • 65 %inguinal hernias are indirect • In females inguinal hernias are as common as femoral hernias OBLIQE INGUINAL HERNIA (I) Congenital theory : Due to persistence of all or part of processes vaginalis . (II) Acquired theory : Due to deficiency of factors (shutter mechanism) which prevent herniation. What is an Indirect Hernia? Deep ring • Congenital or acquired weaknesses in TF • Location: lateral to deep epigastric vessels • Protrude through deep inguinal ring; may descend into the scrotum • Men DIRECT INGUINAL HERNIA – Acquired weaknesses in TF – Location: Hesselbach’s – Emerge between the deep epig. artery and rectus abd. muscle and protrude into the ingu. canal but not into the SC. – More difficult to repair?! – Men FACTORS PREVENTING HERNIATION 1- Oblique coarse of the inguinal canal . 2- Contraction of conjoint tendon during coughing or straining (shutter mechanism) . 3- Contraction of cremasteric muscle : Plugging of inguinal canal CLINICAL FEATURES • Irreducible hernias have either a narrow neck or the contents adhere to the sac wall • Obstructed hernias contain obstructed but viable intestine • Strangulated hernias when the venous drainage from the sac contents is compromised CLINICAL FEATURES • Lump at an appropriate anatomical site Increases in size on coughing or straining. It reduces in size or disappears when relaxed or supine position. • Examination may show it to have a cough impulse and to be reducible QUESTIONS MUST BE ANSWERED AT THE END OF GENERAL AND LOCAL EXAMINATION 1- Hernia or not ? 2- Rt or Lt ? 3- Is it inguinal or femoral ? 4- Is it direct or oblique ? 5- What is the content ? 6- Recurrent or not ? 7- Complicated or not ? 8- what is the predisposing factors ? HERNIAS…COMPLICATIONS • • • • Reducible Irreducible Obstructed or incarcerated Strangulated D.DIAGNOSIS of OIH 1- Other hernia direct inguinal hernia 2- Hydrocele femoral hernia congenital & infantile encysted hydrocele of the cord 3- Ectopic or undescended testicle 4- Psoas abscess 5- Inguinal adenitis 6- Endemic funiculitis 7- Lipoma of the cord COMPLICATIONS Obstruction • Irreducible • abdominal pain, • distension and vomiting may occur • The hernia will be tense tender and irreducible Strangulation • become red and tender, • Irreducible • No impulse on cough. • If contains bowel signs of obstruction. Rt. INDIRECT ING. HERNIA Ex. Ring Test? INTERNAL RING TEST HUGE LONG STANDING IDIH COMPLETE INDIRECT INGUINAL HERNIA INGUINAL HERNIA REPAIR RATIONALE TENTION FREE REPAIR MESH REPAIR HERNIA…REPAIR Irrespective of approach used the following will be achieved • • • • Dissection of the sac Reduction / inspection of the contents Ligation of the sac Approximation of the inguinal and pectineal ligaments INGUINAL HERNIA.TYPES OF REPAIR • Bassini repair : Suturing conjoined tendon to inguinal ligament behind the cord . • Lytle repair: Plication of the fascia transversalis . • Shouldice repair : incision of the fascia & double breasting of it . • Halsted ‘s repair Bassini repair plus reinforced by suturing the 2 leaflets of external oblique together behind the cord INGUINAL HERNIA.TYPES OF REPAIR Tanner’s repair: add to the repair a releasing incision in the rectus sheath to in avoid tension suture line Blood good’s repair: triangular flap of ant rectus sheath wall is turned downward behind its lateral border and sutured to the inguinal ligament . INGUINAL HERNIA.TYPES OF REPAIR • Shouldice or Liechtenstein now regarded as 'gold standard' as judged by low risk of recurrence • Laparoscopic hernia repair: Should be reserved for bilateral or recurrent hernia SPERMATIC CORD STRENTHENING OF THE POSTERIOR WALL OF TH ING. CANAL INCESION INDIRECT INGUINAL HERNIA MESH REPAIR Hernia Sac Vas Deference Hernia Sac Twisted Spermatic Cord with the Vas Preparation of the Mesh for Mesh Repair Right direct inguinal hernia, the sac was coming from the posterior wall of the inguinal canal. The cord is elevated separate from the sac. Left direct inguinal hernia. the sac is separated from the cord. direct inguinal hernia, the sac was fully reduced Spermatic Cord The superior edge of the mesh was tacked down to the aponeurosis or muscle of the internal oblique with a few interrupted sutures. Mesh in place and fixed Laparoscopic Trans-abdominal pre-peritoneal prosthetic Fixation. Mesh in Place Spermatic Cord Peritoneal closure on the pre-peritoneal mesh MORTALITY OF ELECTIVE HERNIA REPAIR The mortality of elective hernia repair increases with age MORTALITY OF STRANGULATED HERNIA REPAIR • 10 %patients with strangulation give no previous history of a hernia • The peak incidence of hernia strangulation is approximately 80 years • In those with acute onset of a hernia the greatest risk is in the first 3 months • Risk of strangulation depends on type of hernia - Femoral is approximately 40% - Direct inguinal is approximately 3% MORTALITY OF STRANGULATED HERNIA REPAIR • The mortality of surgery for strangulated hernias has changed little over the past 50 years • Operative mortality remains at approximately 10% • Is ten times greater than that following an elective repair • Risk of death is dependent on : -Age -Presence of necrotic bowel requiring resection COMPLICATIONS OF HERNIA SURGERY • • • • • Urinary retention Scrotal haematoma Damage to the ileoinguinal nerve Ischaemic orchitis Recurrent hernia TRUSSES • • • • 40000 sold annually in UK 20 %purchased prior to seeing a doctor 45 %have no instruction on fitting 75 %fit whilst standing up ! RECURRENT INGUINAL HERNIA • Recurrence rate varies with herniorrhaphy technique and duration of follow up • With Bassini and darn repairs may be as high as 20% • With Shouldice and Lichtenstein repairs recurrence rates <1% have been reported RECURRENT INGUINAL HERNIA Factor involved in recurrence include : - Inadequate preoperative selection - Type of hernia - Type of operation - Postoperative wound infection RECURRENT HERNIA REPAIR • Recurrent hernias should be repaired using a mesh technique • Can be performed as either an open or a laparoscopic procedure • Patients should be consented for a possible orchidectomy FEMORAL HERNIAS…INCIDINCE. • Account for 7% of all abdominal wall hernia • Female : male ratio is 4:1 • Commonest in middle aged and elderly women • Rare in children • More common in parous ANATOMY OF THE FEMORAL CANAL • Anterior border is the inguinal ligament • Posterior border is the pectineal ligament • Medial border is the lacunar ligament • Lateral border is the femoral vein FEMORAL SHEATH AND CANAL WI TH RELATIONS OF CONTENTS Pubic Tubercle Right Femoral Hernia FEMORAL HERNIA…REPAIR All uncomplicated femoral hernias should be repaired as an urgent elective procedure Three classical approaches to the femoral canal have been described – Low (Lockwood) – Transinguinal (Lotheissen) – High (McEvedy) SPECIAL TYPES OF HERNIA Richter's hernia • Partial enterocele • presents with strangulation and obstruction SPECIAL TYPES OF HERNIA • Maydl's hernia W loop strangulation, Strangulated bowel within abdominal cavity • Litter's hernia Strangulated Meckel's diverticulum Can cause small bowel fistula CONGENITAL INGUINAL HERNA • Presence of an PATENT processes vaginalis . • The hernia reaches down to the bottom of the scrotum. • The testis lies among the contents of the sac • Although congenital , it may appear in adult life . • Herniotomy can be performed at any age provided a skilled anaesthetist and surgeon are available. Incarcerated Congenital Inguinal Hernia LEFT CONGENITAL INGUINAL HERNIA SUBCUTANEIUS HERNIOTOMY DISECTED SAC VAS DEFRENCE VD TRANSFEXSION LIGATION AT THE NECK Wound Closure With Subcuticulr Fine Sutures Previous Rt. H Repair CONGENITAL UMBLICAL HERNIA OXOMPHALUS MINOR Infantile Umblical Hernia • Due to week umblical scar • Repair is not urgent as it can close spontaneously • If persist or became more wide, repair at 2y age. • Very rare to be complicated • Just remove the granuloma • No truss ADULT AQUIRED PARAUMBLICAL HERNIA PATIENT IS STRAINING HUGE VENTRAL HERNIA WITH PENDULUS ABDOMEN HUGE VENTRAL HERNIA WITH PENDULUS ABDOMEN