Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
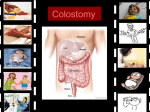
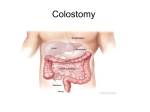
Outline ; ENDOSCOPY INDICATIONS, CONTRAINDICATIONS COMPLICATIONS NURSING RESPONSIBILITIES COLOSTOMY CARE COLOSTOMY IRRIGATION REVIEW OF GASTROINTESTINAL SYSTEM (ALIMENTARY CANAL AND ITS ACCESSORY ORGANS) MOUTH INTESTINE PHARYNX COLON ESOPHAGUS STOMACH, SMALL RECTUM ANAL CANAL ANUS. ENDOSCOPY PROCEDURE NONSURGICAL PROCEDURE USED TO PERFORM: DIAGNOSTIC PROCEDURES • EXAMINE A PERSON'S DIGESTIVE TRACT • VISUALIZE THE GI TRACT • CERTAIN AND THERAPEUTIC PROCEDURES THERAPEUTIC PROCEDURES • REMOVE COMMON BILE DUCT STONES • DILATE STRICTURES • TREAT GASTRIC BLEEDING AND ESOPHAGEAL VARICES. AN ENDOSCOPE HAS : ( FLEXIBLE TUBE WITH A LIGHT AND CAMERA AND CAN BE INSERTED THROUGH THE RECTUM OR MOUTH, DEPENDING ON WHICH PORTION OF THE GI TRACT IS TO BE VIEWED MULTIPURPOSE CHANNELS (AIR INSUFFLATIONS, IRRIGATION, FLUID ASPIRATION, AND THE PASSAGE OF SPECIAL INSTRUMENTS ) AN ENDOSCOPE (WITH A WATER-SOLUBLE LUBRICANT) IS PASSED SMOOTHLY AND SLOWLY ( BACK OF THE MOUTH UPPER PART OF THE SMALL INTESTINE. THE PATIENT WEARS A MOUTH GUARD TO KEEP FROM BITING THE SCOPE. IMAGES OF DIGESTIVE TRACT ARE PRODUCED THROUGH A VIDEO SCREEN MONITOR. http://www.youtube.com/watch?v=W1faSbFuLl8 CAPSULE ENDOSCOPY CAPSULE ENDOSCOPY UTILIZES AN INGESTIBLE CAMERA DEVICE RATHER THAN AN ENDOSCOPE. SWALLOWING A CAPSULE (CAMERA DEVICE), WHICH PASSES THROUGH THE DIGESTIVE SYSTEM WHILE TAKING PICTURES OF THE INTESTINE. CAPSULE (ABOUT THE SIZE OF A LARGE VITAMIN CAPSULE) THAT TAKES MULTIPLE DIGITAL PHOTOS OF THE SMALL BOWEL. THE IMAGES ARE TRANSMITTED VIA SMALL SENSORS ATTACHED TO THE ABDOMEN WITH ADHESIVE STICKERS OR TRANSMITTED WIRELESSLY FROM THE CAPSULE TO RECORDING DEVICE BELTED TO THE PATIENT'S WAIST. CAPSULE ENDOSCOPY No sedation or anesthetic is required. The small bowel is about 6 meters long and the capsule takes about 8 hours to travel through it After approximately 8 hours, the recording device is removed, the physician downloads image data from the recorder to a PC and views the images to make a diagnosis. The capsule will be excreted naturally through the digestive tract. INDICATIONS CONTRAINDICATIONS DYSPHAGIA. ESOPHAGEAL REFLUX SYMPTOMS THAT PERSIST OR RECUR DESPITE APPROPRIATE THERAPY. PERSISTENT VOMITING OF UNKNOWN CAUSE. FOR CONFIRMATION AND SPECIFIC HISTOLOGIC DIAGNOSIS OF RADIOLOGICALLY DEMONSTRATED LESIONS IN PATIENTS WITH ACTIVE GI BLEEDING OR RECENT BLEEDING. WHEN SAMPLING OF TISSUE OR FLUID IS INDICATED. TREATMENT OF BLEEDING LESIONS SUCH AS ULCERS, TUMORS, REMOVAL OF FOREIGN BODIES. PLACEMENT OF FEEDING OR DRAINAGE TUBES (EG, PERCUTANEOUS ENDOSCOPIC GASTROSTOMY). Acute MI Peritonitis Acute perforation Patients who are taking anticoagulants COMPLICATIONS CARDIOPULMONARY COMPLICATIONS RELATED TO SEDATION AND ANALGESIA (MOST COMMON TYPES) ASPIRATION PNEUMONIA ( ASPIRATION OF GASTRIC CONTENTS INTO THE LUNGS IS COMMON, AND MAY RESULT IN DEATH). INFECTIOUS COMPLICATIONS RELATED TO DIAGNOSTIC ENDOSCOPY (PROCEDURE ITSELF , CONTAMINATED EQUIPMENT) PERFORATION. BLEEDING (INJURY TO GASTRIC OR ABDOMINAL WALL VESSELS) NURSING INTERVENTIONS BEFORE THE PROCEDURE 1) EXPLAIN THE FOLLOWING TO THE PATIENT: 1) THE TYPE OF PROCEDURE, ADVISE THAT SOMEONE MUST ACCOMPANY THE PATIENT TO DRIVE HOME DUE TO THE PATIENT BEING SEDATED. 2) NPO FOR 8 TO 12 HOURS BEFORE THE PROCEDURE TO PREVENT ASPIRATION AND ALLOW FOR COMPLETE VISUALIZATION OF THE STOMACH. 3) REMOVE DENTURES AND PARTIAL PLATES TO FACILITATE PASSING THE SCOPE AND PREVENTING INJURY. 4) INFORM THE HEALTH CARE PROVIDER OF ANY KNOWN ALLERGIES AND CURRENT MEDICATIONS. MEDICATIONS MAY BE HELD UNTIL AFTER THE TEST IS COMPLETED. DESCRIBE WHAT WILL OCCUR DURING AND AFTER THE PROCEDURE TO THE PATIENT : 1) THE THROAT WILL BE ANESTHETIZED WITH A SPRAY OR GARGLE. 2) AN I.V. SEDATIVE WILL BE ADMINISTERED. 3) THE PATIENT WILL BE POSITIONED ON THE LEFT SIDE WITH A TOWEL OR BASIN AT THE MOUTH TO CATCH SECRETIONS AND TO PROVIDE EASY ACCESS FOR THE ENDOSCOPE. 4) A PLASTIC MOUTHPIECE WILL BE USED TO HELP RELAX THE JAW AND PROTECT THE ENDOSCOPE. EMPHASIZE THAT THIS WILL NOT INTERFERE WITH BREATHING. 5) ASK PATIENT TO SWALLOW ONCE WHILE THE ENDOSCOPE IS BEING ADVANCED BUT DO NOT TALK, OR MOVE TONGUE. SECRETIONS SHOULD DRAIN FROM THE SIDE OF THE MOUTH, AND THE MOUTH MAY BE SUCTIONED. 6) AIR IS INSERTED DURING THE PROCEDURE TO PERMIT BETTER VISUALIZATION OF THE GI TRACT. MOST OF THE AIR IS REMOVED AT THE END OF THE PROCEDURE. THE PATIENT MAY FEEL BLOATED, BURP, OR PASS FLATUS FROM REMAINING AIR. AFTER THE PROCEDURE 1) NPO UNTIL THE GAG REFLEX RETURNS (IN 1 TO 2 HOURS) 2) ASSESS OR TEST GAG REFLEX 3) AFTER THE PATIENT’S GAG REFLEX HAS RETURNED, THE NURSE CAN OFFER SALINE GARGLE, AND ORAL ANALGESICS TO RELIEVE MINOR THROAT DISCOMFORT. 4) PLACE THE PATIENT IN THE SIM’S POSITION UNTIL HE OR SHE IS AWAKE AND THEN PLACE THE PATIENT IN THE SEMIFOWLER’S POSITION UNTIL READY FOR DISCHARGE. 5) OBSERVE FOR SIGNS OF PERFORATION, SUCH AS PAIN, BLEEDING, UNUSUAL DIFFICULTY SWALLOWING, AND AN ELEVATED TEMPERATURE. 6) BED REST UNTIL FULLY ALERT ( FOR SEDATED PATIENTS). 7) MONITOR PR AND BP FOR CHANGES THAT CAN OCCUR WITH SEDATION. 8) INSTRUCT THE PATIENT NOT TO DRIVE FOR 10 TO 12 HOURS IF SEDATION WAS USED. COLOSTOMY • OPENING THROUGH THE ABDOMINAL WALL IN THE COLON • A SURGICAL PROCEDURE IN WHICH AN OPENING (STOMA) IS FORMED BY DRAWING THE HEALTHY END OF THE LARGE INTESTINE OR COLON THROUGH AN INCISION IN THE ANTERIOR ABDOMINAL WALL AND SUTURING IT INTO PLACE. • THIS OPENING, IN CONJUNCTION WITH THE ATTACHED STOMA APPLIANCE, PROVIDES AN ALTERNATIVE CHANNEL FOR FECES TO LEAVE THE BODY. • IT MAY BE REVERSIBLE OR IRREVERSIBLE DEPENDING ON THE CIRCUMSTANCES. COLOSTOMY OSTOMY APPLIANCE CONSIST OF : • SKIN BARRIER • POUCH – CAN BE CLOSED OR DRAINABLE • ADJUSTABLE OSTOMY BELT CLASSIFICATION OF COLOSTOMY 1. ACCORDING TO STATUS A. PERMANENT – TO PROVIDE MEANS OF ELIMINATION WHEN THE RECTUM OR ANUS IS NON FUNCTIONAL ( BIRTH DEFECT / CANCER) B. TEMPORARY – FOR TRAUMATIC INJURIES OR INFLAMMATORY CONDITIONS OF THE BOWEL, ALLOWING THE BOWEL TO REST AND HEAL CLASSIFICATION OF COLOSTOMY 2. ACCORDING TO CONSTRUCTION OF THE STOMA a. SINGLE – ONE END OF THE BOWEL IS BROUGHT OUT THROUGH AN ABDOMINAL OPENING B. LOOP – LOOP OF BOWEL IS BROUGHT INTO THE ABDOMINAL WALL AND SUPPORTED BY A PLASTIC BRIDGE , OR A PIECE OF RUBBER TUBING; HAS TWO OPENINGS (PROXIMAL AND DISTAL) CLASSIFICATION OF COLOSTOMY 2. CONSTRUCTION OF THE STOMA (CONT.) C. DIVIDED COLOSTOMY – TWO EDGES OF BOWEL BROUGHT OUT INTO THE ABDOMEN BUT SEPARATED FROM EACH OTHER D. DOUBLE BARREL - PROXIMAL AND DISTAL LOOPS OF BOWEL ARE SUTURED TOGETHER FOR ABOUT 10 CM AND BOTH ENDS ARE BROUGHT UP INTO THE ABDOMINAL WALL Divided colostomy – Double barrel INDICATIONS • COLON CANCER • DIVERTICULITIS – INFLAMMATION OF SMALL, BULGING POUCHES THAT FORMS IN THE LININGS OF THE DIGESTIVE TRACT • INJURY - • FECAL INCONTINENCE - IS A LACK OF CONTROL OVER DEFECATION LEADING TO INVOLUNTARY LOSS OF BOWEL CONTENTS—INCLUDING FLATUS (GAS), LIQUID STOOL ELEMENTS AND MUCUS, OR SOLID FECES. OSTOMY MANAGEMENT CONSISTS OF GROUP OF NURSING INTERVENTIONS THAT MAY BE NECESSARY AFTER FECAL DIVERSION SURGERY • STOMA ASSESSMENT • APPLICATION OF STOMA TO COLLECT FECES AND PROTECT SKIN • PROMOTION OF SELF CARE ASSESSMENT Assess for: Normal Abnormal Color Healthy pink, red and slightly moist Dusky pink / bluish (cyanosis) suggest inadequate circulation to the stoma Size and shape New stoma are swollen; swelling decreases in 2-3 weeks or as long as 6 weeks Protrude slightly from the abdomen Failure to recede may indicate blockage Position Must remain on the abdominal surface If stoma retracts, feces may enter the abdominal cavity and cause peritonitis; Prolapse must be reported to the doctor Stomal bleeding Slight bleeding Report other bleeding Complaints Burning sensation under the skin may indicate skin breakdown Abdominal discomfort / distention CHANGE OF OSTOMY APPLIANCE • ORDINARILY THE POUCH MUST BE EMPTIED OR CHANGED A COUPLE OF TIMES A DAY DEPENDING ON THE FREQUENCY OF ACTIVITY • CAN BE APPLIED FOR UP TO 7 DAYS • TWICE A WEEK • CHANGE WHENEVER THE STOOL LEAKS ONTO THE PERISTOMAL SKIN • EVERY 24 – 48 HRS IF THE SKIN IS ERYTHEMATOUS, ERODED, DENUDED OR ULCERATED • MORE FREQUENT CHANGES IF CLIENT COMPLAINS OF PAIN OR DISCOMFORT • THE POUCH IS EMPTIED WHEN IT IS ONE THIRD TO ONE HALF FULL • IF THE POUCH OVERFILLS, IT CAN CAUSE SEPARATION OF THE SKIN BARRIER AND STOOL COMES IN CONTACT WITH THE SKIN PURPOSE OF CHANGING OSTOMY APPLIANCE • TO ASSESS AND CARE FOR PERISTOMAL SKIN • TO COLLECT STOOL FOR ASSESSMENT OF THE AMOUNT AND TYPE OF OUTPUT • MINIMIZE ODORS FOR THE CLIENT’S COMFORT AND SELF ESTEEM COLOSTOMY IRRIGATION • A WAY TO REGULATE BOWEL MOVEMENTS BY EMPTYING THE COLON AT A SCHEDULED TIME • INVOLVES INFUSING WATER INTO THE COLON THROUGH THE STOMA STIMULATING THE COLON TO EMPTY. • ALLOWS FOR THE PERSON TO NOT WEAR A POUCH, BUT RATHER JUST A GAUZE CAP OVER THE STOMA • SCHEDULED IRRIGATION IS DONE FOR TIMES THAT ARE CONVENIENT • TO IRRIGATE, A CATHETER IS PLACED INSIDE THE STOMA, AND FLUSHED WITH WATER, WHICH ALLOWS THE FECES TO COME OUT OF THE BODY INTO AN IRRIGATION SLEEVE. • MOST COLOSTOMATES IRRIGATE ONCE A DAY OR EVERY OTHER DAY, THOUGH THIS DEPENDS ON THE PERSON, THEIR FOOD INTAKE, AND THEIR HEALTH REFERENCES • KOZIER & ERBS’ FUNDAMENTALS OF NURSING . EIGHTH ED. 2008 • POTTER PERRY. BASIC NURSING 6TH ED..MOSBY, MISSOURI, 2006. • HTTP://WWW.CANCER.ORG/TREATMENT/TREATMENTSANDSIDEEFFECTS/PHYSICALSIDEEFFEC TS/OSTOMIES/COLOSTOMYGUIDE/COLOSTOMY-IRRIGATION