Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Definition
• Osteoarthritis (also known as OA) is a
common joint disease that most often affects
middle-age to elderly people. It is commonly
referred to as "wear and tear" of the joints.
• In osteoarthritis, the cartilage between the
bones in the joint breaks down.
• This causes the affected bones to slowly get
bigger.
Etiology
• The etiology of OA is multifactorial. Many patients
have more than one risk factor for the development of
OA.
• The most common risk factors for the development of
OA include:
• obesity (The most important preventable risk factor
for OA of the knee, hip, and hand is obesity)
• occupation
• participation in certain sports
• history of joint trauma, and a genetic predisposition.
• Patients with osteoporosis are also less likely to have
OA, possibly due to the opposite influences of body
weight on bone strength and OA risk.
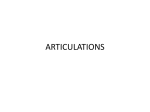
Osteoarthritic Cartilage
• OA most commonly begins with damage to articular
cartilage, through trauma or other injury, excess joint
loading from obesity or other reasons, or instability or
injury of the joint that causes abnormal loading.
• In response to cartilage damage, chondrocyte activity
increases in an attempt to remove and repair the
damage.
• Depending on the degree of damage, the balance
between breakdown and resynthesis of cartilage can be
lost, and a vicious cycle of increasing breakdown can
lead to further cartilage loss.
• Destruction of aggrecans by the proteolytic enzyme
(ADAMTS-5) is considered to play a key role.
Osteoarthritic Cartilage
• Substantial loss of cartilage causes joint space narrowing and
leads to a painful, deformed joint
• Furthermore, the remaining cartilage softens and develops
fibrillations (vertical clefts into the cartilage), and there is splitting,
further loss of cartilage, and exposure of underlying bone.2
• As cartilage is destroyed and the adjacent subchondral bone
undergoes pathologic changes, cartilage is eroded completely,
leaving denuded subchondral bone, which becomes dense, smooth,
and glistening (eburnation).
• A more brittle, stiffer bone results, with decreased weight-bearing
ability and development of sclerosis and microfractures. New bone
formations, or osteophytes, also appear at joint margins distant
from cartilage destruction and are thought to arise from local and
humoral factors. There is direct evidence that osteophytes can help
stabilize osteoarthritic joints.
Clinical Presentation of Osteoarthritis
Age
• Usually elderly
• Gender
• Age <45 more common in men
• Age >45 more common in women
Symptoms
• Pain
• Deep, aching character
• Pain on motion
• Pain with motion early in disease
• Pain with rest late in disease
• Stiffness in affected joints
• Resolves with motion, recurs with rest ("gelling" phenomenon)
• Usually duration <30 minutes
• Often related to weather
• Limited joint motion
• May result in limitations activities of daily living
• Instability of weight-bearing joints
Observation on joint examination(Signs):
• Stiffness in affected joints with or without joint
enlargement
• Bony proliferation or occasional sinusitis
• Local tenderness
• Crepitus (a grating sound or sensation produced
by friction between bone and cartilage or the
fractured parts of a bone).
• Muscle atrophy
• Limited motion with passive/active movement
• Deformity
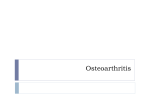
Cartilage loss in OA followed by inflammation
Desired Outcome of treatment
1- educate the patient, family members, and
caregivers.
2-relieve pain and stiffness.
3- maintain or improve joint mobility.
4- limit functional impairment.
5- maintain or improve quality of life.
** Treatment may relieve pain or improve function,
but does not reverse preexisting damage to the
articular cartilage
General Approach to Treatment
Treatment depends on the :
1- distribution and severity of joint involvement.
2- comorbid disease states.
3- concomitant medications.
4- allergies.
Nonpharmacologic Therapy
is an integral part of the treatment plan for all
patients with OA.
• it delay the progression of OA. and to prevent
future functional impairment.
It affect by :
1. number and location of affected joints.
2. degree of functional impairment.
3. body mass index.
4. overall health status..
1- Patient Education
2- Weight Loss
Excess weight increases the biomechanical load on weight-bearing joints and
is the single best predictor of need for eventual joint replacement.
Weight loss of amounts as small as 4% of body weight can lessen OA pain.
3- Exercise
It can improve joint function and can decrease disability, pain, and analgesic
use by OA patients.
Low intensity exersice for 30 min at least for 5 days of weak .
Example :
- Swimming and walking (Isometric exercises not isotonic nor weight bearing
exercises).
- Avoid football and basketball sports
Surgery
1- functional disability .
2- severe pain unresponsive to conservative therapy
total joint replacement (arthroplasty) of the knee and hip have
been developed, although there is substantial overlap in
eligibility criteria.
Drug therapy target:
1- relive the pain .
2- stop the progression of the disease .
3- control the inflammation .
The primary objective of medication is to alleviate pain
1. Treatment of Hip and knee OA
.
First-Line Treatments
ACETAMINOPHEN
•
•
first-line treatment for knee and hip .
Compared with oral NSAIDs, acetaminophen may be modestly less
effective, but it has a lower risk of serious GI and cardiovascular
adverse events and as a consequence is preferred over oral NSAIDs
as first-line .
• acetaminophen in all patients without underlying liver disease,
maximum daily dose is 4g/day and its fatal dose is 24 g.
• ADVERSE EVENT:
hepatotoxicity and possibly renal toxicity with long-term use.
ORAL NSAIDS
• nonspecific or COX-2 selective NSAIDs , as a first-line option for
knee and hip OA if the patient fails acetaminophen.
• It providing superior pain relief in comparison to acetaminophen.
but It have higher risks for GI, renal, and cardiovascular adverse events
compared with acetaminophen.
COX-2 inhibitors carry less risk for both minor and serious GI adverse
events in comparison to nonselective NSAIDs
• Proton-pump inhibitors (PPIs) and misoprostol significantly reduce
the occurrence of GI adverse events in those taking NSAIDs.
Avoid
Diclofenac
TOPICAL NSAIDS—KNEE ONLY
•
topical NSAIDs as a first-line option for knee OA if the patient
fails acetaminophen, and is preferred over oral NSAIDs for those
older than 75.
• It provide pain relief for OA similarly to that obtained with oral
NSAIDs but with fewer GI adverse events.
INTRAARTICULAR CORTICOSTEROIDS
• It recommended as alternative first-line treatment for both knee
and hip OA when pain control with acetaminophen or NSAIDs is
suboptimal.
• Injections can also be administered with concomitant oral
analgesic therapy as needed for additional pain control.
• It safe and well tolerated, but should not be administered more
frequently than once every
3 months due to risks of systemic adverse effects.
Also its effect last for 4-8 weeks.
TRAMADOL
• is a narcotic-like pain reliever used to treat moderate to severe
pain.
• is recommended as an alternative first-line treatment of knee
and hip pain as add on therapy due to OA in patients who
have failed treatment with other first line drugs, and are not
able to receive intraarticular corticosteroids.
• Adverse event :
Nausea, vomiting, constipation, lightheadedness,
somnolence, dizziness, drowsiness, or headache may occur.
Capsaicin
• is an active component of chili peppers.
• As cream or gel It has been found to relieve joint
pain from osteoarthritis in some people when rubbed into the skin
over affected joints.
• Its used as first line for elderly pt .
• Or as add on therapy
Second-Line Treatments
OPIOID ANALGESICS
• ITS NARCOTIC ANALGESIC
• It the primary second-line medication for both knee and hip OA.
• Patients who are at high surgical risk, precluding joint arthroplasty,
are also candidates for opioid therapy.
• Opioids provide effective short-term pain control in patients with
OA, not used for long term .
• Adverse effects:
nausea, vomiting, constipation, somnolence, and dry mouth. Serious
events include falls, respiratory depression, and addiction.
DULOXETINE
• Duloxetine can be used as adjunctive treatment in patients
with a partial response to first-line analgesics, add-on
therapy.
• It given in moderate doses of 60 mg/day.
• Adverse events :
GI with nausea, vomiting, and constipation.
.
INTRAARTICULAR HYALURONIC ACID
• Its not routinely recommend the use of intraarticular HA injections
for knee OA ,it not appear to provide clinically meaningful
improvement in pain and/or function scores.
• Limited efficacy and risks of serious events limit the routine use of
these agents.
•
serious adverse events such as: increased pain, joint swelling, and
stiffness.
• Even glucosamine & chondroitin are constituents of the cartilage
they have no approved role in OA management.
2. Treatment of Hand OA