Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
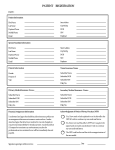
Welcome to Our Office Mr. Dr. Mrs. Ms. Patient Information Today’s Date: ___________ Name: _________________________________ _____ Date of Birth: ______________ Age: _____ Street Address: _________________________________ Social Security #: __________________ City:___________________________________ State: ______ Zip: _______________ Home #: ____________________ Cell #: ____________________ Work #: _________________ Email Address: ________________________________________________________________________ (Used only to send information and confirming appointments) Race: _____________ Ethnicity: _________________ Primary Language: _________________________ Employer: _____________________________________ Occupation:_____________________________ Parent/Spouse Name: _________________________________ Phone #: _________________________ Address: _____________________________________________________________________________ VISION PLAN (Circle one): VSP/Nassau County/Davis/Eye Med/ Other: _____________________ Primary MEDICAL Insurance Information Policy holder Name: __________________________ SS#: ___________________ DOB: ______________ Insurance Co: ___________________________________ ID/Policy #: ____________________________ Relationship to patient: __________________ Employer: ______________________________________ Secondary Insurance to File Name: ______________________________________ SS#: _________________ DOB: _______________ Insurance Co: _________________ ID/Policy #: _______________ Relationship to patient: ___________ General Health Do you have Y N Family Do you have Y N Family Diabetes Asthma Hypertension Cancer Heart Problems Blindness Kidney Problems Arthritis Thyroid Problems Other Do you have Y N Family High Cholesterol Multiple Sclerosis Macular degeneration Headaches/Migraine Name of PCP: ______________________________________ Phone #: ___________________________ Address: _____________________________________________________________________________ Last Eye Exam : ______________________ Last General Physical Exam :_________________________ List Medical Conditions for which you are being treated: _______________________________________ _____________________________________________________________________________________ Current Medications:____________________________________________________________________ _____________________________________________________________________________________ List all medications you are ALLERGIC to: ___________________________________________________ _____________________________________________________________________________________ PATIENT HISTORY Vision Correction History (please check any that apply) Amblyopia (Lazy Eye) Blurred vision at a distance Blurred vision at near Burning Double vision Drooping eyelid Dryness Eye pain/soreness Floaters or spots Fluctuating vision Foreign body sensation Halos Regular Headaches Stopped wearing contacts Stopped wearing glasses Infection of eye/lid Itching Loss of peripheral vision Glasses History (check all that apply) What glasses do you own? Loss of vision Mucous discharge Redness Sandy or gritty feeling Sensitivity to light/glare Strabismus (crossed eyed) Tired eyes Watery eyes Check any that apply: Allergic to nickel I do not want to wear glasses Incorrect prescription Need spare glasses Need sunglasses with UV Problems with current glasses Problems with glare How many hours per day do you spend using a computer? ___ Problems with night vision Backup pair Bifocals Distance Progressive lens Reading Safety glasses Single vision Sports glasses Sunglasses Trifocals Contact Lens History (check all that apply) What brand of contact do you wear? ___________ Check any that apply: I do not wear contacts How old are your current contacts? ________________ Incorrect prescription How often do you replace them? __________________ Interested in refractive laser surgery What solution do you use for soaking? ______________ Need spare contacts What is your typical wearing schedule? ______________ Problems with current contacts Would like to change my eye color Referral Info: How did you learn about our office? (Circle Appropriate Source) Relative / Friend/ HMO Ins / Location/ Doctor Referral/ Internet Family Member who are patients here: ______________________________________________ ______________________________________________________________________________ If you are a new patients, who may we thank for referring you? __________________________