Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
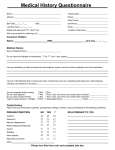
Welcome to Racine Optical Co. Date .................................................. Employer/School ................................................................................ Last ...........................................First ............................. MI .............. Occupation ......................................................................................... Address ................................................................................................ Your DOB ...................................................Age ................................ City ...........................................State ............................ ZIP .............. Insurance Subscriber’s Name & DOB .............................................. Best Phone Number .......................................................................... ............................................................................................................. SSN....................................................................................................... *PLEASE present your MEDICAL & VISION INSURANCE cards for Email Address .................................................................................... our reconds.* Main purpose of your visit today? Check One. ☐ Eye Glasses ☐ Contacts ☐ Vision & Eye Health Are you having problems with your current contacts or glasses? ...................................................................................................................... How did you hear about us? ☐ Radio ☐ Ad ☐ TV ☐ Friend (Please name)........................................................................................... Medical History Do you or any of your family have the following conditions? Name of family physician ................................................................. Condition You Family Relation Blindness ☐☐ ....................................... Date of last physical exam.................................................................. Cataracts ☐☐ ....................................... Current medications (Rx or over the counter). List name of medicaCorneal Problems ☐ ☐ ....................................... tion, including eye drops, vitamins and birth control. Glaucoma ☐☐ ....................................... ........................................................................................................... Lazy Eye ☐ ☐ ....................................... ........................................................................................................... Retinal problems ☐ ☐ ....................................... ........................................................................................................... Diabetes ☐☐ ....................................... Do you have any medication allergies? ☐ Yes ☐ No Heart Disease ☐ ☐ ....................................... If yes, please list ................................................................................ Macular Degeneration ☐ ☐ ....................................... ........................................................................................................... Have you ever been diagnosed or treated for any of the following? ☐ Corneal Abrasion ☐Iritis/Uveitis ☐Eye Injury ☐Lasik / RK ☐Eye Infection ☐Retinal Detachment ☐Other Eye Disorders (List below) ........................................................................................................... ☐Allergies ☐High Blood Pressure ☐ Asthma ☐High Cholesterol ☐ Arthritis ☐Thyroid Problems ☐Cancer ☐Other Medical Issues (List below) .............................................................................................................. Tell us about yourself... Do you currently wear contact lenses?. ☐ Yes ☐ No Check one. ☐ Dailies ☐ 2-Week ☐ Monthlies What solutions used? ......................................................................... If you wear contact lenses, are you satisfied with your vision and comfort? ☐ Yes ☐ No Would you prefer contact lenses to change the color of your eyes? ☐ Yes ☐ No Do you have an interest in a “test drive” of the latest contact lens designs? ☐ Yes ☐ No Patient Eye History Date of last eye exam ........................................................................ Do you experience the following? (Check box if your answer is yes) ☐ Blurry Vision ☐Grittiness ☐Burning Eyes ☐Itchy Eyes ☐ Tearing ☐Occasional Dryness ☐ Headaches ☐Sunlight Sensitivity ☐Double Vision ☐Crossed Eye / Eye Turn ☐Flashes of Light ☐Trouble Seeing at Night ☐ Floaters ☐Uncomfortable Glasses Do you...(Check box if your answer is yes) ☐Work at a computer? ☐Think you’d benefit from thinner, lighter lenses? ☐Spend time outdoors? ☐Have prescription sunglasses? ☐Prefer not to wear glasses at times? ☐Want information on Laser Vision Correction surgery? ☐Have children or family in need of eye care? ☐If you wear bifocals, do the lines or head tilting other you? Payment Policy:. Eyewear and Contact Lenses — A 50% down-payment is required on all purchases with remaining balance to be paid at dispensing. Every pair of eyewear is custom made for your eyes, so returns are subject to a 30% restocking fee. Professional Services — Payment in full is expected at the time of service. If you have vision and/or health insurance, we will submit a claim for you. The balance on your account will remain your responsibility. I agree and understand that regardless of my insurance status, I am ultimately responsible for the balance on my account for any service rendered. I authorize the release of any information necessary to process my insurance claim. Signature ....................................................................................................................................... Date ........................................................................................ Would you like a copy of Racine Optical’s Notice of Privacy Practices for your records? ☐ Yes ☐ No