Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
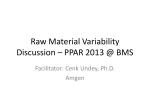
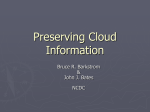
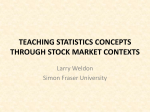
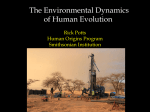
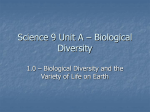
Short- and Long-Term Blood Pressure Variability Present and Future Giuseppe Mancia I experimental animals, that is, the disappearance of some variability components with the persistence or even the increase of others.6 The factors possibly responsible for 24-hour BP variability are illustrated in Figure 1. Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 t has long been known that blood pressure (BP) is characterized by an array of spontaneous variations.1 That is, BP values vary markedly within the 24 hours because of day-night changes but also because of differences among hours, minutes, and even adjacent beats. They also show variations over more prolonged periods because of differences among days, months, and seasons,2 also with a trend for systolic BP to increase over the years and for diastolic BP to display an age-related biphasic change.3 This article summarizes current knowledge on short-term (within the 24 hours) and long-term BP variability. Mention will be made of the following: (1) factors responsible for BP variations and mechanisms through which they occur; (2) the relationship of BP variability with BP mean values in absence and during antihypertensive treatment; and (3) the prognostic significance of BP variability. Current limitations of the studies on BP variability will be also discussed to emphasize what future studies should address. Relationship With 24-Hour BP Mean Early studies with intra-arterial ambulatory BP monitoring have shown that 24-hour, daytime, and nighttime BP variabilities (quantified as the SD of the 24-hour, day, and night mean values) increase from normotensives to patients with a progressively more severe hypertension7 (Figure 2, top left). They have further shown that an increase of BP variability when BP mean increases also occurs within individuals, because the BP SD becomes progressively greater from the half hours in which mean BP is lowest to the half hours in which it is maximal (Figure 2, top right). They have also shown that, from normotensive to hypertensive subjects, the increase in BP SD is proportional to the increase in mean BP, with, thus, no change in the coefficient of variation (Figure 2, bottom left). However, this is not the case within individuals in whom the increase in BP variability associated with an increase in BP mean is more pronounced and accompanied by an increase in its normalized value (Figure 2, bottom right). It is possible that the resetting of the baroreflex that is known to occur during prolonged BP elevations, such as hypertension,8 allows its antioscillatory influence to remain fully operative, thereby attenuating the increase in BP variability that accompanies more transient increases of BP mean. Twenty-Four Hour BP Variability Factors and Mechanisms A large body of evidence shows that, over the 24 hours, BP undergoes marked variations in response to physical activity, sleep, and emotional stimuli of various nature and duration, thereby documenting the profound involvement of behavioral influences on BP variability. However, spontaneous BP variations also occur independently on behavior. For example, throughout the day and night, BP oscillates regularly at different frequencies, presumably because of influences originating within the brain.4 Furthermore, BP varies more or less regularly in response to the mechanical forces generated by ventilation and also shows irregular nonbehaviorally and nonmechanically related changes with a possible origin from humoral influences and even local vasomotor phenomena. Finally, BP variations are opposed throughout the 24 hours by the baroreflex, which makes the magnitude of 24-hour BP variability in a given individual the net effect of prooscillatory and antioscillatory influences.1 Some of these influences operate via the sympathetic nervous system,5 but nonneural mediators are also importantly involved, as shown by the complex effects of sympathectomy on BP variability in Effect of Antihypertensive Treatment Both intra-arterial and noninvasive ambulatory BP monitoring have shown that 24-hour, daytime, and, to a lesser extent, nighttime BP SDs all decrease as the corresponding BP mean is reduced by antihypertensive drugs.1 This occurs with a variety of antihypertensive treatments, that is, angiotensinconverting enzyme inhibitors, calcium channel blockers, central agents, and -blockers without or with vasodilator properties given alone or in combination with a diuretic,9–17 suggesting that this is the consequence of BP lowering, per se. Interestingly, in most instances the reduction of the SD has been found to be proportional to the reduction of the mean Received March 5, 2012; first decision April 12, 2012; revision accepted April 12, 2012. From the University of Milano-Bicocca, Milan, Italy. This paper was sent to John E. Hall, Consulting editor, for review by expert referees, editorial decision, and final disposition. Correspondence to Giuseppe Mancia, Department of Medicine, University of Milano-Bicocca, St Gerardo Hospital, via Pergolesi 33, 20900 Monza (MB), Italy. E-mail [email protected] (Hypertension. 2012;60:512-517.) © 2012 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.112.194340 512 Mancia + + Mechanical factors + + + BP variabi lity Ventilation Figure 1. Factors involved in 24 hour blood pressure (BP) variability. The sign “⫹” refers to factors favoring and the sign “⫺” to factors opposing BP variations. The query indicates absence of conclusive evidence. Arterial stiffness ? -/+ Other reflexes ? Genetic factors ? Rhythmic influences (probably largely centra l) + + Baroreflexes Environmental stimuli Prognostic Relevance Intra-arterial and noninvasive BP monitoring studies have shown that, for a given 24-hour BP mean value, cardiac and vascular damage are greater and lower in subjects with, 24h SD * 8 * 6 * Half hour mean (mmHg) * 10 24h SD (mmHg) Half hour mean and SD n = 176 * * 4 2 n=10 n=31 n=69 n=66 N BH MH SH 0 n = 89 130 Mean 12 120 10 110 SD 100 8 90 6 19 3 23 7 19 15 11 Half hour SD (mmHg) Time of the 24 hours Half hour mean SD and CV 24h CV n = 176 10 6 4 2 n=10 n=31 n=69 n=66 N BH MH SH 0 12 n = 89 12 ∆ 10 10 ∆ 8 ∆ 6 ∆ 6 4 4 2 8 Half hour CV (%) 8 Half hour mean (mmHg) 12 24h CV (%) Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 respectively, a greater and lower 24-hour BP SD.19,20 Furthermore, evidence has been obtained that, over a follow-up of several years, an initially greater BP variability leads to a greater progression of the left ventricular mass index or carotid-intima media thickness value.21,22 Finally, and most importantly, in several studies, BP variability within the 24 hours has been found to be an independent predictor of the incidence of cardiovascular events.22–27 For example, Sander et al22 have shown a greater 24-hour BP SD of systolic BP to be accompanied by a greater 3-year incidence of cardiovascular morbid and fatal events. Kikuya et al23 have found that, BP value with, thus, little or no change in the BP coefficient of variation.18 The change of BP variability associated with antihypertensive treatment thus reflects the difference in BP variability between normotensive and hypertensive individuals, making it possible that a baroreflex resetting (this time toward lower BP values) is again involved. 12 513 Vasomotiion ? Humoral ? (endothelial etc) factors Behavioral factors Short and Long-Term BP Variability 2 Lowest Inter- Highest mediate Lowest Inter- Highest mediate Half hour MAP values Figure 2. Top left panel, SD of the 24-hour average value for mean arterial pressure in normotensive subjects (N) and borderline (B), moderate (M), and severe (S) hypertensive (H) patients. Top right panel, Half-hour average values for mean arterial pressure and the corresponding SD for the 24-hour blood pressure (BP) monitoring in normotensive and hypertensive subjects pooled. Bottom left panel, Coefficient of variation (CV) of the 24-hour average value for mean arterial pressure in the subjects of top left panel. Bottom right panel, SD and CV for the half hours with the lowest, intermediate, and highest average values for mean arterial pressure in the subjects of top right panel. Data were collected by intra-arterial ambulatory BP monitoring. Bars refer to the SD of the mean. *P⬍0.05; ⌬P⬍0.01. Adapted from Mancia et al7 with permission of the publisher. Copyright © 1983, the American Heart Association, Inc. 514 Hypertension August 2012 CV Mortality DBP variability HR R P value SD 24h 1.13 ((0.98-1.31) 0.098 SD day 1.24 (1.07-1.44) 0.004 SD night 1.13 ((0.97-1.31) 0.11 Day-night ∆ 0.90 (0.78-1.04) 0.16 Residual (erratic) variability 1.24 (1.07-1.43) ( 0.005 0.5 1.0 Figure 3. Risk of cardiovascular mortality for a 1-SD increase in various measures of 24-hours diastolic blood pressure (BP) variability. Data were adjusted for the covariates indicated at the bottom. Numbers in parenthesis refer to 95% CIs. Adapted from Mancia et al.24 2.0 models adjusted for age / gender / smoking / previous CV events / LVMI / serum cholesterol and * Cox glucose / 24h mean DBP Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 in subjects with a daytime SD of systolic BP lower than ⬇16 mm Hg, the rate of cardiovascular mortality as assessed over a multiyear follow-up was significantly less than in subjects with an SD of systolic BP equal or above this value. Verdecchia et al27 have seen that, in initially untreated hypertensive patients followed for 16 years, an enhanced BP variability during the night was an independent predictor of cardiac events. Mancia et al24 have observed that, in the general population of the Pressioni Arteriose Monitorate e Loro Associazioni Study, the 12-year cardiovascular mortality exhibited a positive relationship with the magnitude of the day and night erratic diastolic BP changes that could be detected by eliminating the cyclic components (nocturnal and postprandial BP falls) by Fourier analysis of the 24-hour BP tracing, independent of other potentially confounding demographic and clinical cardiovascular risk factors (Figure 3). Indeed, as shown in Table 1, these erratic BP variations were found to be a predictor of cardiovascular fatal events more important than the mean 24-hour BP value and the difference in day-night BP, for which the relationship with cardiovascular mortality was of a protective nature. They were also found to exceed the prognostic importance of 24-hour BP mean, suggesting a nonmarginal contribution to cardiovascular risk. Current Limitations and the Future Current knowledge on 24-hour BP variability has important limitations (Table 2), which makes future studies in this area important. First, more studies are needed on the factors and mechanisms involved in this phenomenon and, in particular, on the role played by arterial stiffness and genetic factors on Table 1. Multivariate Analysis Showing Diastolic BP Values Independently Predicting CV and All-Cause Death CV Death All-Cause Death the magnitude and patterns of short-term BP variations. Second, some studies have shown short-term BP variability not to predict events after adjustment for potential confounders or have concluded that its prognostic importance is minor vis-à-vis that of mean BP values.28 Thus, additional longitudinal evidence based on an accurate quantification of the variability phenomena (see below) would be desirable. Third, more evidence is needed on whether some drugs or treatment strategies have greater effects on within 24-hour BP variations than others. Furthermore, because 24-hour ambulatory BP has not been used in large-scale trials on antihypertensive treatment (except for small substudies on nonrandomized patients), the protective effect of treatment-induced changes in BP variability with respect to the concomitant changes in BP mean awaits proper documentation. Finally, when using noninvasive ambulatory BP monitoring (the only approach suitable for large, long-term studies) it will be important to more precisely quantify the magnitude of the 24-hour BP variations. This means to space BP readings by ⱕ15 or 20 minutes, because, beyond these intervals, quantification of the 24-hour BP SD can be grossly inaccurate.29 It also means the use of indices other than the SD, because the same SD (or the coefficient of variation) value may be associated with completely different patterns of BP variability. Complementary measures, such as the weighted SD, the frequency distribution, or the BP ranges over the day and night and the average differences between consecutive systolic or diastolic values may offer some advantages.30,31 It should be emphasized, however, that no matter which measure is used, this goal can hardly be obtained via noninvasive automatic Table 2. Twenty-Four h BP Variability: Limitations and Future ● More information on factors/mechanisms involved (eg, arterial stiffness, genetic factors) ● Data from observational studies with larger No. of events/statistical power P Value 2 P Value Variability 30.80 ⬍0.0001 31.69 0.0001 ● Data from randomized trials (protective effect of treatment-induced reduction of BP variability?) 2Day/night (inverse) 21.34 0.001 19.87 0.001 ● Head-to-head comparisons of different drugs/drug combinations 24-h mean 16.11 0.003 16.40 0.002 ● More precise assessment of 24-h SD/CV Diastolic BP Value 2 BP indicates blood pressure; CV, cardiovascular. Data show adjustment of age, sex, cholesterol, glucose, smoking, previous CV events, and left ventricular hypertrophy. Data are from a 12-y follow-up of the general population recruited in the Pressione Arteriose Monitorate e Loro Associazioni Study. ● Need of beat-to-beat BP measuring devices (not interfering with subjects activity/sleep) for mechanistic/prognostic studies of variability components including speed of BP changes BP indicates blood pressure; CV, cardiovascular. Mancia Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 ambulatory BP monitoring, which provides ⬍0.1% of the BP values that occur over the 24 hours. Furthermore, because noninvasive automatic BP measurements require the patient to stop any activity at the time of measurement, this approach does not capture BP variability in truly real-life conditions. Finally, although in a previous study intra-arterially measured nighttime BP fall was found to be superimposable with and without concomitant noninvasive ambulatory BP monitoring,32 the possibility that cuff inflations (and the accompanying noise) alter sleep pattern and its cardiovascular effects, at least in some patients, cannot be excluded. The most important progress for BP variability will, therefore, be to develop devices that measure beat-to-beat ambulatory BP noninvasively without restriction at a cost that could make their use in large and long-term studies feasible. Beat-to-beat BP monitoring would also allow us to apply methods such as restricted or broad-band spectral analysis to the recorded tracing, thereby detecting even subtle differences in the magnitude and type of BP variations.33 It would even permit us to assess on a large scale the speed of the BP changes during the frequent pressor and depressor episodes that occur spontaneously over the 24 hours. BP has been shown to change faster in hypertensive than in normotensive subjects throughout the day and night,34 but no data are available on whether the potentially greater traumatic effect of faster BP changes on the heart and the vessel wall favors organ damage and increases the risk of cardiovascular events. Long-Term BP Variability Evidence Information on the factors involved in long-term BP variations are scattered and incomplete. Behavioral changes are regarded to play a major role on day-to-day BP variations, particularly those making the ambulatory BP values of the working days, and of Monday in particular, different from those of the weekend.35 Changes in temperature are thought to be the main reason for the lower BP that characterizes summer as compared with winter months.36 Large artery stiffening is known to be majorly responsible for the progressive BP changes that occur with aging.37 Little is known, on the other hand, about the factors responsible for the BP difference that has been observed between visits spaced by months or years in observational studies and antihypertensive drug trials.38–40 These differences, however, have been shown to have a prognostic value. For example, in the hypertensive patients with a history of coronary disease of the International Verapamil-Trandolapril Study,40 the incidence of cardiovascular morbid and fatal events increased progressively as the number of on-treatment visits in which BP was controlled to ⬍140/90 mm Hg increased from ⬍25% to ⱖ75%, irrespective of the mean BP value throughout the treatment period. Even more impressively, in the high-risk hypertensive patients of the Anglo-Scandinavian Cardiac Outcome Trial, the incidence of cardiovascular events, and of stroke in particular, increased progressively as the SD or the coefficient of variation of the on-treatment BP mean increased from the lowest to the highest decile value.38 This implies that physicians should pay attention to consistency of BP control over Short and Long-Term BP Variability 515 Table 3. Visit-to-Visit Intra-Individual BP Variability: Limitations and Future ● Derived from post hoc analysis of data/comparisons of nonrandomized groups ● Several visits needed/patients with early events excluded ● Limited information on factors involved/could reflect different timing of BP measurement and/or adherence to treatment ● Low correlation with visit-to-visit variability of 24-h mean BP ● Use of interindividual variability as a surrogate for intraindividual variability questionable BP indicates blood pressure. time, because lack of control at any given visit may have adverse prognostic consequences, a conclusion recently reached also by the Ongoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial in which the risk of a cardiovascular event showed a relationship with the BP status in the immediately preceding visit.41 This may not be an easy goal to achieve, however, because an unstable BP control is a common phenomenon not only in clinical practice but also in trials. In the European Lacidipine Study on Atherosclerosis, for example, ⬇40% to 50% of the treated hypertensive patients achieved a BP ⬍140/90 mm Hg at each yearly visit, whereas in only approximately one third of them was BP control achieved for the entire 4-year duration of treatment.42 Limitations Before concluding that consistency of BP control represents an additional important goal of antihypertensive treatment, important limitations of current evidence on visit-to-visit BP variability should be mentioned (Table 3). Fourth, visit-tovisit BP variability has been studied by a post hoc approach, which means that comparisons have involved nonrandomized groups, a condition that does not guarantee that factors other than those under study play a role. Second, because a number of values is needed to quantify BP variability, patients experiencing an early event have been excluded, limiting the analysis to the later part of a trial. Third, the variability of visit-to-visit on-treatment clinic BP has shown a very limited relationship (correlation coefficients between 0.10 and 0.20) with the concomitant visit-to-visit variability of on-treatment 24-hour mean BP,43 which means that consistency of clinic BP control may not reflect that of 24-hour BP control, that is, a measure of recognized prognostic importance.44–46 Fourth, no conclusive data exist on the effect of different drugs or treatment regimens on visit-to-visit BP variability, because, in absence of data from individual subjects, this has been quantified by the more or less wide range of the BP-lowering effect of treatment in the whole group of patients.47 Although this “interindividual” variability has been claimed to be significantly related to the “intraindividual” one, it is not easy to understand why the more or less uniform BP effect of an antihypertensive drug in a large group of patients should measure the tendency of the BP-lowering effect of treatment in a given individual to be more or less sustained with time. Finally, much more will have to be learned regarding the factors responsible for between-visit BP variations during 516 Hypertension August 2012 antihypertensive treatment. Although it cannot be excluded that neurohumoral and structural characteristics of the cardiovascular system are involved, it will be important to know the contribution of more practical factors, such as the different timing of BP measurements at different visits, that is, the fact that at one visit BP measurements may be closer to drug administration that at another visit, and the role played by patient adherence to the prescribed treatment regimen, because adherence to treatment has been shown to be prognostically important.48,49 Progress on all of above points will be possible, if at variance from what has been done in the past,50 future trials will collect precise information on intraindividual BP variability during the treatment. Disclosures 15. 16. 17. 18. 19. None. 20. References Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 1. Parati G, Di Rienzo M, Mancia G, Zanchetti A. Blood pressure variability. In: Handbook of Hypertension, Zanchetti A, eds. Amsterdam, the Netherlands: Elsevier; 1997:117–169. 2. Sega R, Cesana G, Bombelli M, Grassi G, Stella ML, Zanchetti A, Mancia G. Seasonal variations in home and ambulatory blood pressure in the PAMELA population: Pressione Arteriose Monitorate E Loro Associazioni. J Hypertens. 1998;16:1585–1592. 3. Wolf-Maier K, Cooper RS, Banegas JR, Giampaoli S, Hense HW, Joffres M, Kastarinen M, Poulter N, Primatesta P, Rodríguez-Artalejo F, Stegmayr B, Thamm M, Tuomilehto J, Vanuzzo D, Vescio F. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA. 2003;289:2363–2369. 4. Parati G, Castiglioni P, Di Rienzo M, Omboni S, Pedotti A, Mancia G. Sequential spectral analysis of 24-hour blood pressure and pulse interval in humans. Hypertension. 1990;16:414–421. 5. Narkiewicz K, Winnicki M, Schroeder K, Philips BG, Kato M, Cwalina E, Somers VK. Relationship between muscle sympathetic nerve activity and diurnal blood pressure profile. Hypertension. 2002;39:168–172. 6. Daffonchio A, Franzelli C, Radaelli A, Castiglioni P, Di Rienzo M, Mancia G, Ferrari AU. Sympathectomy and cardiovascular spectral components in conscious normotensive rats. Hypertension. 1995;25: 1287–1293. 7. Mancia G, Ferrari A, Gregorini L, Parati G, Pomidossi G, Bertinieri G, Grassi G, di Rienzo M, Pedotti A, Zanchetti A. Blood pressure and heart rate variabilities in normotensive and hypertensive human beings. Circ Res. 1983;53:96–104. 8. Grassi G, Cattaneo BM, Seravalle G, Lanfranchi A, Mancia G. Baroreflex control of sympathetic nerve activity in essential and secondary hypertension. Hypertension. 1998;31:68–72. 9. Ferrari AU, Buccino N, Pedotti A, Mancia G, Zanchetti A. Labetalol and 24 hour monitoring of arterial blood pressure in hypertensive patients. J Cardiovasc Pharmacol. 1981;3:S42–S52. 10. Mancia G, Ferrari AU, Gregorini L, Parati G, Pomidossi G, Bertinieri G, Zanchetti A. Evaluation of a slow release clonidine preparation by direct continuous blood pressure recording in essential hypertensive patients. J Cardiovasc Pharmacol. 1981;3:1193–1202. 11. Mancia G, Ferrari AU, Pomidossi G, Parati G, Bertinieri G, Grassi G, Gregorini L, Di Rienzo M, Zanchetti A. Twenty-four hour blood pressure profile and blood pressure variability in untreated hypertension and during antihypertensive treatment with once-a-day nadolol. Am Heart J. 1984;108:1078–1083. 12. Pomidossi G, Parati G, Motolese M, Mancia G, Zanchetti A. Hemodynamic effects of once a day administration of combined clorthalidone and metoprolol retard in essential hypertension. Int J Clin Pharmacol Ther Toxicol. 1984;12:665–671. 13. Pomidossi G, Parati G, Malaspina D, Camesasca C, Motolese M, Zanchetti A, Mancia G. Antihypertensive effect of a new formulation of a slow release oxeprenolol in essential hypertension. J Cardiovasc Pharmacol. 1987;10:593–598. 14. Parati G, Pomidossi G, Casadei R, Ravogli A, Trazzi S, Mutti E, Mancia G. 24 h ambulatory non-invasive blood pressure monitoring in the 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. assessment of the antihypertensive action of celiprolol. J Internat Med Res. 1988;16:52A–61A. Mancia G, De Cesaris R, Fogari R, Lattuada S, Montemurro G, Palombo C, Porcellati C, Ranieri G, Tettamanti F, Verdecchia P, Marelli C, Omboni S, Ravogli A, Zanchetti A. Evaluation of the antihypertensive effect of once-a-day trandolapril by 24 hour ambulatory blood pressure monitoring. Am J Cardiol. 1992;70:60D–66D. The Italian Verapamil Study Group. 4 hour antihypertensive effect of verapamil sustained release 240 mg vs nitrandipine and enalapril in essential hypertension. High Blood Press. 1993;2:241–248. Omboni S, Ravogli A, Fogari R, Riva D, Mancia G. Effect of once-a-day fosinopril on 24h ambulatory blood pressure in mild to moderate essential hypertension. High Blood Press. 1994;3:103–107. Mancia G, Omboni S, Ravogli A, Parati G, Zanchetti A. Ambulatory blood pressure monitoring in the evaluation of antihypertensive treatment: additional information from a large data-base. Blood Press. 1995; 4:148–156. Parati G, Pomidossi G, Albini F, Malaspina D, Mancia G. Relationship of 24-hour blood pressure mean and variability to severity of target-organ damage in hypertension. J Hypertens. 1987;5:93–98. Mancia G, Parati G, Hennig M, Flatau B, Omboni S, Glavina F, Costa B, Scherz R, Bond G, Zanchetti A, for the ELSA Investigators. Relation between blood pressure variability and carotid artery damage in hypertension: baseline data from the European Lacidipine Study on Atherosclerosis (ELSA). J Hypertens. 2001;19:1981–1989. Frattola A, Parati G, Cuspidi C, Albini F, Mancia G. Prognostic value of 24-hour blood pressure variability. J Hypertens. 1993;11:1133–1137. Sander D, Kukla C, Klingelhöfer J, Winbeck K, Conrad B. Relationship between circadian blood pressure patterns and progression of early carotid atherosclerosis: a 3-year follow-up study. Circulation. 2000;102: 1536–1541. Kikuya M, Ohkubo T, Metoki H, Asayama K, Hara A, Obara T, Inoue R, Hoshi H, Hashimoto J, Totsune K, Satoh H, Imai Y. Day-by-day variability of blood pressure and heart rate at home as a novel predictor of prognosis: the Ohasama Study. Hypertension. 2008;52:1045–1050. Mancia G, Bombelli M, Facchetti R, Madotto F, Corrao G, Trevano QF, Grassi G, Sega R. Long-term prognostic value of blood pressure variability in the general population: results of the Pressioni Arteriose Monitorate e Loro Associazioni Study. Hypertension. 2007;49:1265–1270. Dawson SL, Manktelow BN, Robinson TG, Panerai RB, Potter JF. Which parameters of beat-to-beat blood pressure and variability best predict early outcome after acute ischemic stroke? Stroke. 2000;31:463–468. Pringle E, Phillips C, Thijs L, Davidson C, Staessen JA, de Leeuw PW, Jaaskivi M, Nachev C, Parati G, O’Brien ET, Tuomilehto J, Webster J, Bulpitt CJ, Fagard RH, for the Syst-Eur investigators. Systolic blood pressure variability as a risk factor for stroke and cardiovascular mortality in the elderly hypertensive population. J Hypertens. 2003;21:2251–2257. Verdecchia P, Angeli F, Gattobigio R, Rapicetta C, Reboldi G. Impact of blood pressure variability on cardiac and cerebrovascular complications in hypertension. Am J Hypertens. 2007;20:154–161. Hansen TW, Thijs L, Li Y, Boggia J, Kikuya M, Björklund-Bodegård K, Richart T, Ohkubo T, Jeppesen J, Torp-Pedersen C, Dolan E, Kuznetsova T, Stolarz-Skrzypek K, Tikhonoff V, Malyutina S, Casiglia E, Nikitin Y, Lind L, Sandoya E, Kawecka-Jaszcz K, Imai Y, Wang J, Ibsen H, O’Brien E, Staessen JA, for the International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes Investigators. Prognostic value of reading-to-reading blood pressure variability over 24 hours in 8938 subjects from 11 populations. Hypertension. 2010;55: 1049–1057. Di Rienzo M, Grassi G, Pedotti A, Mancia G. Continuous vs intermittent blood pressure measurements in estimating 24-hour average blood pressure. Hypertension. 1983;5:264–269. Bilo G, Giglio A, Styczkiewicz K, Caldara G, Maronati A, KaweckaJaszcz K, Mancia G, Parati G. A new method for assessing 24h blood pressure variability after excluding the contribution of nocturnal blood pressure fall. J Hypertens. 2007;25:2058–2066. Castiglioni P, Parati G. Present trends and future directions in the analysis of cardiovascular variability. J Hypertens. 2011;29:1285–1288. Villani A, Parati G, Groppelli A, Omboni S, Di Rienzo M, Mancia G. Noninvasive automatic blood pressure monitoring does not attenuate nighttime hypertension: evidence from 24 h intraarterial blood pressure monitoring. Am J Hypertens. 1992;5:744–747. Castiglioni P, Daffonchio A, Ferrari AU, Mancia G, Pedotti A, Di Rienzo M. Blood pressure and heart rate variability in conscious rats before and Mancia 34. 35. 36. 37. 38. Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 39. 40. 41. after autonomic blockade: evaluation by broad band spectral analysis. Comput Cardiol. 1993:487–490. Mancia G, Parati G, Castiglioni P, Tordi R, Tortorici E, Glavina F, Di Rienzo M. Daily life blood pressure changes are steeper in hypertensive than in normotensive subjects. Hypertension. 2003;42:277–282. Murakami S, Otsuka K, Kubo Y, Shinagawa M, Matsuoka O, Yamanaka T, Nunoda S, Ohkawa S, Kitaura Y. Weekly variation of home and ambulatory blood pressure and relation between arterial stiffness and blood pressure measurements in community-dwelling hypertensives. Clin Exp Hypertens. 2005;27:231–239. Modesti PA, Morabito M, Bertolozzi I, Massetti L, Panci G, Lumachi C, Giglio A, Bilo G, Caldara G, Lonati L, Orlandini S, Maracchi G, Mancia G, Gensini GF, Parati G. Weather-related changes in 24-hour blood pressure profile: effects of age and implications for hypertension management. Hypertension. 2006;47:155–161. Reference Values for Arterial Stiffness’ Collaborators. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: establishing normal reference values. Eur Heart J. 2010;31:2338–2350. Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlöf B, Sever PS, Poulter NR. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010;375:895–905. Muntner P, Shimbo D, Tonelli M, Reynolds K, Arnett DK, Oparil S. The relationship between visit-to-visit variability in systolic blood pressure and all-cause mortality in the general population: findings from NAHNES III, 1988 to 1994. Hypertension. 2011;57:160–166. Mancia G, Messerli F, Bakris G, Zhou Q, Champion A, Pepine CJ. Blood pressure control and improved cardiovascular outcomes in the International Verapamil SR-Trandolapril Study. Hypertension. 2007;50: 299–305. Mancia G, Schumacher H, Redon J, Verdecchia P, Schmieder R, Jennings G, Yusoff K, Ryden L, Liu GL, Teo K, Sleight P, Yusuf S. Blood pressure targets recommended by guidelines and incidence of cardiovascular and renal events in the Ongoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial (ONTARGET). Circulation. 2011;124: 1727–1736. Short and Long-Term BP Variability 517 42. Mancia G, Parati G, Bilo G, Maronati A, Omboni S, Baurecht H, Hennig M, Zanchetti A. Assessment of long-term antihypertensive treatment by clinic and ambulatory blood pressure: data from the European Lacidipine Study on Atherosclerosis. J Hypertens. 2007;25:1087–1094. 43. Mancia G, Facchetti R, Parati G, Zanchetti A. Visit-to-visit blood pressure variability in the European lacidipine study on atherosclerosis: methodological aspects and effects of antihypertensive treatment. J Hypertens. 2012;30:1241–1251. 44. Staessen JA, Thijs L, Fagard R, O’Brien ET, Clement D, de Leeuw PW, Mancia G, Nachev C, Palatini P, Parati G, Tuomilehto J, Webster J. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension: Systolic Hypertension in Europe Trial Investigators. JAMA. 1999;282: 539–546. 45. Dolan E. Stanton A, Thijs L, Hinedi K, Atkins N, McClory S, Den Hond E, McCormack P, Staessen JA, O’Brien E. Superiority of ambulatory over clinic blood pressure measurements in predicting mortality: the Dublin Outcome Study. Hypertension. 2005;46:156–161. 46. Sega R, Facchetti R, Bombelli M, Cesana G, Corrao G, Grassi G, Mancia G. Prognostic value of ambulatory and home blood pressures compared with office blood pressure in the general population: follow-up results from the Pressioni Arteriose Monitorate e Loro Associazioni (PAMELA) Study. Circulation. 2005;111:1777–1783. 47. Webb AJ, Fischer U, Mehta Z, Rothwell PM. Effects of antihypertensivedrug class on interindividual variation in blood pressure and risk of stroke: a systematic review and meta-analysis. Lancet. 2010;375:906–915. 48. Simpson SH, Eurich DT, Majumdar SR, Padwal RS, Tsuyuki RT, Varney J, Johnson JA. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ. 2006;333:315. 49. Corrao G, Parodi A, Nicotra F, Zambon A, Merlino L, Cesana G, Mancia G. Better compliance to antihypertensive medications reduces cardiovascular risk. J Hypertens. 2011;29:610–618. 50. Fischer U, Webb AJS, Howard SC, Rothwell PM. Reporting of consistency of blood pressure control in randomised controlled trials of antihypertensive drugs: a systematic review of 1372 trial reports. J Hypertens. In press. Short- and Long-Term Blood Pressure Variability: Present and Future Giuseppe Mancia Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 Hypertension. 2012;60:512-517; originally published online June 25, 2012; doi: 10.1161/HYPERTENSIONAHA.112.194340 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2012 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/60/2/512 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/