Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
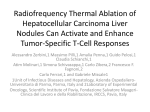
Europace (2008) 10, 1428–1433 doi:10.1093/europace/eun283 Electrophysiology study and radiofrequency catheter ablation of atriofascicular tracts with decremental properties (Mahaim fibre) at the tricuspid annulus Shomu Bohora, Santosh Kumar Dora*, Narayanan Namboodiri, Ajitkumar Valaparambil, and Jaganmohan Tharakan Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala 695011, India Received 5 April 2008; accepted after revision 21 September 2008; online publish-ahead-of-print 19 October 2008 KEYWORDS Mahaim fibre; Electrophysiology study; Radiofrequency ablation Aims The aim was to study the common mapping methods for Mahaim fibre and their role in radiofrequency (RF) ablation. Methods and results Fifteen patients having Mahaim fibre tachycardia underwent electrophysiological study. Mahaim fibre mapping methods like (i) Mahaim potential (M), (ii) shortest atrial stimulus-to-preexcitation (STP), and (iii) mechanical trauma induced loss of conduction were studied. Accessory pathway mapping was performed by M potential in 10 patients (67%), shortest atrial STP in 3 patients (20%), and mechanical trauma in 2 patients (13%). Mahaim fibre was localized at right atrial freewall of tricuspid annulus (8–10 o’clock) in 13 patients (87%), at 6.30 o’clock in one patient, and at 5 o’clock in 1 patient. Fourteen patients underwent RF ablation. Thirteen patients had complete loss of conduction over accessory pathway and one had partial modification with a conduction delay. Radiofrequency ablation was not performed in one patient (shortest STP group) due to its closeness to the compact atrioventricular node. Mahaim junctional acceleration during RF ablation was observed in all patients of M potential, 1 patient of mechanical trauma, and none of the atrial STP group. One patient (M potential group) had tachycardia recurrence during follow-up. Conclusion Mahaim fibre is commonly located between 8 and 10 o’clock at tricuspid annulus. M potential guides to successful RF ablation in most patients. Mahaim junctional acceleration is commonly seen during RF ablation guided by M potential map. Introduction Methods Mahaim fibre leads to wide QRS tachycardia and was first described by Mahaim and Benatt.1 It is associated with the characteristic electrophysiological (EP) features.2–7 Although initially the Mahaim fibre was thought to be nodofascicular, later studies showed it to be atriofascicular8–17 pathway. Various mapping techniques have been described in the literature to localize the Mahaim fibre. We tried to evaluate the usefulness of these mapping techniques with regard to the results of radiofrequency (RF) ablation. All consecutive cases of Mahaim fibre tachycardia who underwent EP study from January 2002 to June 2007 in our centre were included in the study. Various EP properties of Mahaim fibre, techniques used to localize it, results of catheter ablation, and follow-up data were analysed. Aim of the study The aim was to study different mapping methods and their role in RF ablation outcome in Mahaim fibre tachycardia. * Corresponding author. Tel: þ91 471 2524466; fax: þ91 471 2446433. E-mail address: [email protected] EP study During the study period, of the 510 patients who underwent EP study with the intention of RF ablation, 15 were found to have accessory pathway with the characteristics of Mahaim fibre. As per the standard protocol of our institute, quadripolar catheters were placed at right ventricular (RV) apex, His bundle (HB), and right atrium. A decapolar catheter was positioned in the coronary sinus via right internal jugular vein. The RV catheter was used to record right bundle (RB) from either the proximal or distal poles. Programmed atrial stimulation was performed to determine the antegrade conduction pattern to ventricle. The refractory periods of atrioventricular (AV) node and accessory pathway were noted. Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected]. Mapping methods for Mahaim fibre and their role in RF ablation Programmed stimulation was performed at RV apex to determine the retrograde conduction pattern to the atrium. The relationship of M potential, RB, and HB was studied during sinus rhythm and tachycardia. The criteria for the presence of Mahaim fibre conduction included (i) baseline normal QRS or manifest pre-excitation with left bundle branch block morphology, (ii) programmed atrial pacing leading to manifest pre-excitation and increase in AV interval along with shortening of HV interval at shorter pacing cycle lengths, (iii) absence of retrograde conduction over the accessory pathway during ventricular stimulation, and (iv) RB electrogram preceding HB activation during antegrade pre-excitation and SVT. Mapping and RF ablation Once the presence of Mahaim accessory pathway was confirmed by the EP properties described above, the mapping was performed to localize it using a 4 mm deflectable tip ablation catheter (Stinger, CR Bard Inc., MA, USA). Mapping was initiated at the lateral tricuspid annulus due to its common location at that region. The tricuspid annulus was mapped during sinus rhythm in left anterior oblique and right anterior oblique fluoroscopy projections. Three mapping strategies were adopted with the following order of preference: (i) M potential, which is defined as a discrete deflection between atrial and ventricular signal with the interval between the M potential and ventricular electrogram remaining constant during the AV delay produced by atrial pacing, (ii) shortest stimulus-to-preexcitation (STP) interval defined by the shortest interval from a paced atrial site to the pre-excited QRS, and (iii) mechanical trauma induced loss of conduction over Mahaim fibre. Long sheath (SR-0, Daig, St Jude Medical, MN, USA) was routinely used in all cases to facilitate the stability of the ablation catheter. A Bard EP recording system was used for all the procedures (CR Bard Inc.). After localizing M potential, RF energy was delivered at that site. Other strategies of localizing the Mahaim fibre were attempted in cases of failure to obtain the M potential or unsuccessful ablation at the site of best presumed M potential despite the delivery of optimal energy. The RF generator used was from either of the two manufacturers (EPT-1000, Boston Scientific, MA, USA or IBI-1500T11, St Jude Medical, MN, USA). A stimulation study was performed after RF ablation to establish the absence of antegrade conduction over the Mahaim fibre and non-inducibility of the tachycardia. Results Of the 510 patients who underwent EP study during the study period, 15 were found to have Mahaim fibre mediated tachycardia. Baseline characteristics of these patients are mentioned in Table 1. Of them, 11 patients had tachycardia in spite of good compliance to medications. Fourteen patients had a documented wide QRS tachycardia of left bundle branch morphology. Two had associated Ebstein’s anomaly of the tricuspid valve, whereas others had structurally normal heart. The QRS axis during the tachycardia varied from þ45 to 260º. Table 2 shows the EP characteristics of the patients studied. Atrial pacing protocol showed manifest preexcitation with decremental AV conduction in all patients. Ventricular pacing showed retrograde decremental conduction via the AV node. During absence of pre-excitation, the HV interval was positive, whereas during pre-excitation it was negative (Figure 1). The relationship of M potential, HB and RB during sinus rhythm with preexcitation has been shown (Figure 2). The tachycardia could be induced in 13 patients, and in all the cases, QRS morphology during tachycardia was same as pre-excited QRS during atrial pacing. The 1429 Table 1 Baseline characteristics Number of patients Age Clinical features Palpitation Syncope Duration of symptoms Associated structural heart disease Ebstein’s anomaly Drugs Calcium channel blocker Betablocker Amiodarone Combination of two or more No drugs ECG Minimal pre-excitation during sinus rhythm No pre-excitation ECG documented tachycardia Tachycardia rate QRS axis during tachycardia 15:7 males and 8 females 12–44 years 15 2 0.2–20 years 2 11 4 3 4 1 9 6 14 183.53 + 18.53/min (156–220) þ458 to 2608 Table 2 Electrophysiological characteristics Sinus cycle length AH interval HV interval Antegrade refractory period AV node Mahaim fibre SVT cycle length Mahaim fibre localization 8–10 o’clock 5 o’clock 6.30 o’clock Other associated tachycardias AVNRT Atrial flutter 818.8 + 130 (548–1032) ms 82.9 + 16.1 (58–120) ms 41.1 + 6.72 (30–54) ms 297 + 70.72 (210–420) ms 296.25 + 47.79 (230–360) ms 329.73 + 71.86 (262-440) ms 13 1 1 2 2 M potential could be mapped in 10 patients, shortest STP in 3 patients, and catheter trauma induced loss of preexcitation in 2 patients (Figure 2). The Mahaim fibre was localized between 8 and 10 o’clock of tricuspid annulus in 13 patients and at 6.30 and 5 o’clock in one each (Figure 3). Radiofrequency ablation was delivered in temperature-controlled mode at a target temperature of 558C and power output of 30 W in all the cases. The ablation time ranged from 120 to 500 (180 + 28) s. All patients in the M potential group had successful RF ablation. However, one patient had recurrence of tachycardia after 2 months, who underwent M-potential-guided successful ablation in another sitting. All other patients of this group remained free of tachycardia at follow-up. In the shortest STP group, one patient had successful RF ablation. Another had partial modification of Mahaim fibre conduction following RF ablation giving rise to prolonged antegrade conduction time. In this patient, the tachycardia was no more inducible. Mahaim fibre was localized close to the compact 1430 S. Bohora et al. Figure 1 (A) Burst atrial pacing shows pre-excited QRS. The right bundle (RB) precedes His bundle (HB). The last beat shows a sinus beat with narrow QRS. Note that the HB precedes RB. (B) Wide QRS tachycardia with left bundle branch block morphology similar to pre-excited QRS as seen in A. Note that the RB precedes HB. HRAD, high right atrium distal; HBED, His bundle electrogram distal; CSP, coronary sinus proximal dipole; and CSD, coronary sinus distal dipole. Figure 2 During sinus rhythm with wide QRS M precedes right bundle (RB), which in turn precedes His bundle (HB), indicating retrograde activation of the proximal part of RB up to HB. RFD, radiofrequency distal. All other abbreviations are same as Figure 1. Mapping methods for Mahaim fibre and their role in RF ablation 1431 Figure 3 Solid circles show the sites where Mahaim fibre was located at the tricuspid annulus. Figure 4 Radiofrequency ablation at the site of Mahaim fibre location resulting transient Mahaim junctional acceleration. The QRS morphology is similar to Mahaim tachycardia. HRAP, high right atrium proximal. All other abbreviations are same as Figure 2. AV node in one patient and thus ablation was not attempted. Two patients had intermittent loss of pre-excitation on mechanical trauma during catheter manipulation at the lateral tricuspid annulus. Both had successful RF ablation at the same site. Radiofrequency ablation resulted in Mahaim junctional acceleration (MJA) in all the patients of the M potential group and in one of the two patients who had localization by ‘bump mapping’ (Figure 4). Time to 1432 S. Bohora et al. junctional acceleration during RF ablation ranged from 3 to 25 (7 + 3.5) s. None of the shortest STP group had MJA during RF ablation. Programmed atrial stimulation showed dual AV node physiology and inducible AV re-entrant tachycardia (AVNRT) in two patients. Both of them underwent successful slow pathway ablation. Typical atrial flutter was inducible in two patients, of whom one underwent successful cavotricuspid isthmus ablation. The other patient with atrial flutter, had 2:1 AV conduction over the parahisian accessory pathway with Mahaim fibre like properties, had Ebstein’s anomaly and hence ablation of the isthmus or accessory pathway was not attempted. The patients had a mean follow-up of 18 + 5.4 months. There was only one recurrence of tachycardia in the M-potential-guided RF ablation group as mentioned above. All other patients remained free of symptoms at follow-up. the view that MJA during ablation is a dependable marker of successful ablation. Concomitant presence of other types of tachyarrhythmias in patients with Mahaim fibre-mediated tachycardia has been described in the literature.4,13,16–19 Our study showed typical AVNRT and typical atrial flutter in two patients each. No previous cases of co-existing atrial flutter and Mahaim fibre have been reported. Discussion Conclusion The EP property of the Mahaim fibre is characterized by decremental antegrade conduction over the accessory pathway.3,4,6,10 All our patients had EP properties consistent with Mahaim fibre conduction. There are several reports on ablation of Mahaim accessory pathway with a high success rate.4,7,12–19 Various ablation strategies are described in the literature. The recording of M Potential is associated with high degree of acute procedural success.4,7,15–19 In our study, M potential could be recorded in 67% of patients and RF ablation resulted in abolition of conduction over accessory pathway in all. M potential remains an easy and effective way of mapping and ablating the Mahaim fibre. Shortest STP as a mapping method for Mahaim fibre localization has remained inconsistent in the literature.12,17–19 This method involves stimulation at many locations of tricuspid annulus and is time consuming. Mahaim fibre was localized by this method in three of our patients one of whom had an RF ablation resulting in partial modification, with prolonged antegrade conduction. However, in the absence of a proper M potential, this method remains helpful in localizing Mahaim fibre. Mahaim fibre is located very close to the endocardium and thus catheter movement-related mechanical trauma resulting in transient loss of conduction is not uncommon. Mapping and RF ablation guided by this method has occasionally been useful. Cappato et al.14 showed a very high immediate success rate with this method but there was high recurrence at follow-up. This can be due to delivery of RF ablation at a wrong site leading to high recurrence at follow-up. Unintentional mechanical trauma during catheter positioning sometimes results in abolition of conduction over the pathway for minutes to hours.12,17 In our study, two patients underwent successful RF ablation with this method with no recurrence noted on follow-up. However, this should still be the least preferred method of RF ablation in Mahaim fibre. Radiofrequency ablation of Mahaim fibre often gives rise to MJA, which is considered as a marker of successful ablation.4,13,18,19 Twelve of our patients had MJA, of which only one had recurrence that was successfully ablated again with the same approach. Our study also confirms to M potential can be mapped at the lateral tricuspid annulus in majority of patients having Mahaim fibre tachycardia, which can guide to successful RF ablation. This approach often results in MJA compared with other approaches for ablation and reliably predicts long-term procedural outcome. Coexistence of other tachyarrhythmias is not uncommon. Limitations This is an observational and retrospective study. However, we included all consecutive cases of Mahaim fibre mediated tachycardia undergoing EP study since January 2002. This study consists of only 15 patients which is a small number but compares well with many other studies published in the literature. This is a single centre study and Mahaim fibre mediated tachycardia is relatively rare. Acknowledgements We are grateful to Mr K. Suji and Ms Setu, technical assistants, EP lab, for their assistance during study of these cases. Conflict of interest: none declared. References 1. Mahaim I, Benatt A. Nouvelles récherches sur les connections supérieures de la branche du faisceau de His-Tawara avec cloison interventriculaire. Cardiologia 1937;1:61–76. 2. Gallagher JJ, Smith WM, Kasell JH, Benson DW Jr, Sterba R, Grant AO. Role of Mahaim fibres in cardiac arrhythmias in man. Circulation 1981; 64:176–89. 3. Gillette PC, Garson A Jr, Cooley DA, McNamara DG. Prolonged and decremental antegrade conduction properties in right anterior accessory connections: wide QRS antidromic tachycardia of left bundle branch block pattern without Wolff–Parkinson–White configuration in sinus rhythm. Am Heart J 1982;103:66–74. 4. McClelland JH, Wang X, Beckman KJ, Hazlitt HA, Prior MI, Nakagawa H et al. Radiofrequency catheter ablation of right atriofascicular (Mahaim) accessory pathways guided by accessory pathway activation potentials. Circulation 1994;89:2655–66. 5. Haissaguerre M, Warin JF, Le Metayer P, Maraud L, De Roy L, Montserrat P et al. Catheter ablation of Mahaim fibers with preservation of atrioventricular nodal conduction. Circulation 1990;82:418–27. 6. Tchou PJ, Keim SG, Kinn RM, Rist KE, Setter SF, Adhar G. Electrophysiologic evidence for an ectopic node-His like atrioventricular conduction system in an atriofascicular pathway. Pacing Clin Electrophysiol 1992; 15:51. 7. Haissaguerre M, Cauchemez B, Marcus F, Le Metayer P, Lauribe P, Poquet F et al. Characteristics of the ventricular insertion sites of accessory pathways with anterograde decremental conduction properties. Circulation 1995;91:1077–85. 8. Becker AE, Anderson RH, Path MRC, Durrer D, Wellens HJJ. The anatomical substrates of Wolff–Parkinson–White syndrome: a clinic-pathologic correlation in seven patients. Circulation 1978;57:870–9. 9. Bhandari A, Morady F, Shen EN, Schwartz AB, Botvinick E, Scheinman MM. Catheter-induced His bundle ablation in a patient with reentrant Mapping methods for Mahaim fibre and their role in RF ablation 10. 11. 12. 13. 14. tachycardia associated with a nodoventricular tract. J Am Coll Cardiol 1984;4:611–6. Tchou P, Lehmann MH, Jazayeri M, Akhtar M. Atriofascicular connection or a nodoventricular Mahaim fiber? Electrophysiologic elucidation of the pathway and associated reentrant circuit. Circulation 1988;77: 837–48. Klein GJ, Guiraudon GM, Kerr CR, Sharma AD, Yee R, Szabo T et al. ‘Nodoventricular’ accessory pathway: evidence for a distinct accessory atrioventricular pathway with atrioventricular node-like properties. J Am Coll Cardiol 1988;11:1035–40. Klein L, Hackett FK, Zipes DP, Miles WM. Radiofrequency catheter ablation of Mahaim fibers at the tricuspid annulus. Circulation 1993;87: 738–47. Grogin HR, Randall JL, Kwasman M, Epstein LM, Schamp DJ, Lesh MD et al. Radiofrequency catheter ablation of atriofascicular and nodoventricular Mahaim tracts. Circulation 1994;90:272–81. Cappato R, Schluter M, Weiss C, Siebels J, Hebe J, Duckeck W et al. Catheter-induced mechanical conduction block of right-sided accessory 1433 15. 16. 17. 18. 19. fibers with Mahaim-type preexcitation to guide radiofrequency ablation. Circulation 1994;90:282–90. Brugada J, Martinez-Sanchez J, Kuzmicic B, Figueiredo MO, Matas M, Pava LF et al. Radiofrequency catheter ablation of atriofascicular pathways guided by discrete electrical potentials recorded at the tricuspid annulus. Pacing Clin Electrophysiol 1995;18:1388–94. Heal SC, Davies DW, Ward DE, Garrat CJ, Rowland E. Radiofrequency catheter ablation of Mahaim tachycardia by targeting Mahaim potentials at the tricuspid annulus. Br Heart J 1995;73:250–7. Kottkamp H, Hindricks G, Shenasa H, Chen X, Wichter T, Borggrefe M et al. Variants of preexcitation-specialized atriofascicular pathways, nodofascicular pathways, and fasciculoventricular pathways: electrophysiologic findings and target sites for radiofrequency catheter ablation. J Cardiovasc Electrophysiol 1996;7:916–30. Sternick EB, Gerken LM, Vrandecic MO. Appraisal of ‘Mahaim’ automatic tachycardia. J Cardiovasc Electrophysiol 2002;13:244–9. Singh B, Gupta RK, Dhall A, Ghose T, Trehan R, Kaul U. Mahaim automatic accelerated rhythm: a marker of successful radiofrequency ablation. Indian Heart J 2004;56:215–9.