Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Trichinosis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Neonatal infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Oesophagostomum wikipedia , lookup
Sarcocystis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
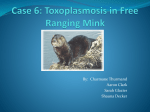
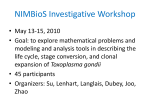
Europace (2006) 8, 221–223 doi:10.1093/europace/euj046 CASE REPORT Complete atrioventricular block associated with toxoplasma myocarditis Matteo Mariani, Massimo Pagani, Corinna Inserra, and Stefano De Servi* Department of Cardiovascular Disease, Unit of Cardiology, Ospedale Civile di Legnano, Via Candiani, 2Legnano, Milan, Italy Received 16 April 2005; accepted after revision 21 November 2005; online publish-ahead-of-print 13 February 2006 KEYWORDS Toxoplasma; Myocarditis Myocarditis has been described during and after a wide variety of infectious agents: viral, rickettsial, bacterial, protozoal, and metazoal diseases may cause cardiac inflammation. We report a case of toxoplasma myocarditis in a young healthy man. A 19-year-old man, with a medical history of paracetamolinduced coma, developed symptoms of fever, nausea, and vomiting. He was taking no medication at the time of admission to the hospital. Physical examination revealed hepatomegalia as the only abnormal finding. After a few days of hospitalization, he was discharged with a diagnosis of acute viral hepatitis associated with junctional bradycardia with a period of sinus bradycardia (Figure 1) raising a suspicion of viral myocarditis. One week later, he complained of dyspnoea during light physical activity. Physical examination revealed only bradycardia. ECG showed complete atrioventricular (AV) block, with a narrow QRS at a rate of 32 bpm and an atrial rate of 66 bpm (Figure 2); cardiac enzymes and echocardiography were normal. An ergometric test showed no increase of heart rate on physical activity. All serological tests were normal or negative (including HIV) except the IgM and IgG titres to Toxoplasma gondii, respectively, 1.94 IU/mL (International Unit) (negative ,1, positive 1.75) and IgG 56 IU/mL (negative ,10, positive 15). No myocardial biopsy was performed. Further, patient history indicated that he had worked as a gardener 1 month before the symptoms started. Thoracic and abdominal computed tomography was performed without evidence of abnormal findings. Cranial magnetic resonance showed small areas (in the occipitoparietal brain cortex bilaterally and in the right hemisphere of cerebellum) of low density probably related to toxoplasma infection (Figure 3). Therapy with antibiotics (co-trimixazole) was started. * Corresponding author. Tel: þ39 0331 449513; fax: þ39 0331 449810. E-mail address: [email protected] Several electrocardiograms and 24 h recordings showed constant complete AV block with a junctional rate of 32 bpm. After 3 weeks of antibiotic therapy, electrocardiogram showed no change. Considering the complete AV block and echocardiographic findings (early right atrial and right ventricular enlargement), we decided to implant a dualchamber pacemaker. Two months later, the patient had resumed a normal life with unrestricted physical activity without symptoms. A new echocardiogram showed normal diameters of right atrium and ventricle, a normal left ventricular ejection fraction. During pacemaker interrogation, AV block was still present (the patient was pacemakerdependent). T. gondii is a zoonotic infection; in areas of Europe (France, Germany, Switzerland, and Spain), the prevalence of latent T. gondii infection is high with reports of 50–70% of population testing seropositive for anti-toxoplasma antibodies (10–40% in the USA).1 The parasite infects all orders of mammals, but cats are the most common hosts. Cats excrete T. gondii oocysts in their faeces and ingestion of faecally contaminated material by humans leads to primary T. gondii infection (undercooked meat is a second route of infection).2,3 Our patient, working as a gardener, had probably been infected by the first way of contamination (he denied having eaten undercooked meat). Toxoplasmosis manifests as encephalitis, pneumonitis (usually in immunosuppressed patients), chorioretinitis, and myocarditis. However, myocardial involvement is uncommon; manifestations of toxoplasma myocarditis may include arrhythmias (atrial and ventricular), sudden death, AV block, pericarditis, and heart failure. Antibiotic & The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: [email protected] 222 M. Mariani et al. treatment of toxoplasma myocarditis has a variable response and has no effect on the cystic form. Our patient had two toxoplasmosis manifestations: cerebral lesions, documented by cranial magnetic resonance, Figure 1 Rhythm strip showing period of normal sinus rhythm 1 week before AV block. Figure 2 Rhythm strip showing atrioventricular block, with junctional rate of 32 bpm and an atrial rate of 66 bpm. Figure 3 and myocardial involvement with complete AV block (no lesions were found in the lungs and retina). The elevation of IgM titre of toxoplasma indicated a recent infection and combined with the clinical history, we believe that this patient probably had toxoplasma myocarditis involving the conduction system with persistent complete AV block. To our knowledge, this patient is the second AV block case related to toxoplasma infection described in the literature. Duffield et al. 4 described a case of T. gondii myocarditis that resulted in recurrent, symptomatic AV block in a 25-year-old woman. On the contrary, our patient developed constant AV block. Dual-chamber pacemakers were implanted in both the patients. Protozoal myocarditis includes trypanosomiasis, prevalent in Central and South America,5 and toxoplasmosis that occurs most commonly in immunosuppressed patients with malignant diseases and also occasionally in patients with the acquired immunodeficiency syndrome and after cardiac or bone marrow transplantation.6 We believe that the importance of this case is related to the high probability of implanting pacemaker when T. gondii myocarditis involves the conduction tissue of the heart, even if appropriate antibiotic therapy is used. Cranial magnetic resonance showing small areas of low density in the left occipito-parietal brain cortex probably related to toxoplasma infection. AV block with toxoplasma myocarditis References 1. Derouin F, Thuilliez P, Garin Y. Value and limitations of toxoplasmosis serology in HIV patients. Pathol Biol 1991;39:255–9. 2. Frenkel J, Dubey J, Miller N. Toxoplasma gondii in cats: fecal stages identified as coccidian oocysts. Science 1970;167:893–6. 3. Bearman M, McCabe R, Wong S, Remington J. Toxoplasma gondii. In: Mandell G, Bennett J, Dolin R, eds. Douglas and Bennett’s Principles and 223 Practice of Infectious Diseases. Vol. 2. New York: Churchill Livingstone, 1995;2455–69. 4. Duffield JS, Jacob AJ, Miller HC. Recurrent, life-threatening atrioventricular dissociation associated with toxoplasma myocarditis. Heart 1996; 76:453–4. 5. Hagar JM, Rahimtoola SH. Chagas’ heart disease. Curr Probl Cardiol 1995;20:825. 6. Hofman P, Drici MD, Gibelin P et al. Prevalence of Toxoplasma myocarditis in patients with the acquired immunodeficiency syndrome. Br Heart J 1993;70:376.