Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
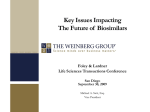
Impact of market access factors in the adoption of biosimilar anti-TNFs across Europe A PRECISION BRIEF Introduction The recent entry of biosimilar anti-TNFs into the European marketplace has attracted considerable attention. Much Figure 1. Biosimilar infliximab discount vs uptake Country averages, based on data reported by respondents, N=54 of the commentary to date has centered 100% threatens pharma company revenue streams and will drive significant cost savings for payers. But price only tells part of the story. Structural and perceptual differences have led to considerable heterogeneity in the levels of discounting and uptake across – and even within – European markets. Our research explores the market access considerations other than price that play an important role in biosimilar adoption rates. Reported biosimilar UPTAKE (% total infliximab) on price: how competitive discounting 80% 60% 40% 20% 0% 0% 20% 40% 60% 80% 100% Reported average biosimilar NET discount (vs Remicade’s list price) To support this research, we conducted a total of 54 in-depth interviews, across 9 European markets,* targeting a mix of payer and clinicians who play an influential role in decision making for anti-TNF biosimilars in their respective markets (detailed sample available on request). Prescribing Behavior With Biosimilar Anti-TNFs Initiating naïve patients on a biosimilar anti-TNF is widely accepted, but attitudes toward switching vary considerably across markets. In the case of infliximab, clinicians in Norway and Poland have now switched the majority of their stable Remicade patients to the cheaper Remsima or Inflectra biosimilar. In Germany, 54 The number of in-depth interviews across 9 European markets Netherlands, Spain, and the UK, many of the more progressive centers have also now switched, but clinicians in France, Italy, and Portugal remain largely resistant. Figure 2. Likelihood of infliximab biosimilar prescribing Average answers based on 1-5 rating, payers and physicians answers, N=54 Market Naïve patients Switch patient stable on Remicade Switch patient stable on other anti-TNF 80% 2 of respondents claim that infliximab-naïve, eligible, patients receive an infliximab biosimilar exclusively *France, Germany, Italy, Netherlands, Norway, Poland, Portugal, Spain, UK. 20% of respondents note widespread switching But price is not the main barrier to switching (only 14% of respondents say it is). Most (54%) cite the need for more data and experience with biosimilar infliximab, because biosimilars are not identical to the originator product in the same way that small molecules are. This leads to clinical and ethical concerns with switching a stable patient to a biosimilar purely for economic reasons. The outcomes of the NOR-SWITCH study are expected to address these concerns, providing increased confidence in the safety of switching. But for ethical reasons, most clinicians would never switch a patient stable on a different anti-TNF to infliximab biosimilar based solely on cost. Prescribing practices for the subcutaneous biosimilar anti-TNFs (ie, etanercept and adalimumab) are expected to follow a similar pattern. However, switching may come sooner as etanercept has low immunogenicity rates; by the time biosimilar adalimumab becomes available, switching is likely to be accepted. The Role of Market Access Tools in Biosimilar Adoption Although discounting plays an important role in biosimilar adoption rates, without the right initiatives to incentivize their implementation, it can be a blunt instrument. Payers (and manufacturers) have a number of tools at their disposal to influence the adoption of biosimilars – and these can be exerted at different points in the decision-making chain. Figure 3. Biosimilar decision points Guidelines and recommendations Tendering and contracting Rx quotas Automatic substitution policies Purchasing Prescribing Dispensing PAYER TOOLS Purchasing – Tendering and Contracting Tendering and contracting represent important means of driving discounts and uptake of biosimilars. With some exceptions in Germany and France, anti-TNFs are classed as hospital products in most markets, with local payers incentivized to seek favorable discounts as they keep the difference between the negotiated net price and the formal reimbursement price. NOR-SWITCH is a randomized double-blind, parallel-group study to evaluate the safety and efficacy of switching from originator to biosimilar infliximab compared with continued treatment with originator infliximab in patients with rheumatoid arthritis, spondyloarthritis, psoriatic arthritis, ulcerative colitis, Crohn’s disease, and chronic plaque psoriasis. 3 However, because authorities have yet to advocate the interchangeability of biosimilar anti-TNFs, most markets are still using nonexclusive tenders, allowing clinicians to retain their freedom to prescribe (limiting biosimilars to naïve patients only in many cases). Class tenders are only used in cost-conscious markets (eg, Norway and the UK), where anti-TNFs are considered undifferentiated. However, these contracts only apply to treatment-naïve patients, and clinicians are not forced to switch patients. Exclusive tenders are uncommon outside Poland. Figure 4. Tender types and implications for formulary inclusions Nonexclusive Tender Formulary inclusion Implications Exclusive Tender Class Tender Both originator and typically one biosimilar on formulary Only one product per INN in formulary for both naïve and switch patients All products within class are included in formulary but sorted by cost Physicians will prescribe based on personal choice, guidelines, and controls All legacy patients are switched to tender winner Prescribing order determined for class; physicians hold option to deviate from guidance Applicable Markets Prescribing – Guidelines and Recommendations National payer guidelines remain heavily influenced by clinicians, with medical societies devoted to specific diseases tending to form the basis for their recommendations. However, regional and local payers tend to be more progressive in their guidance, either recommending or enforcing the use of infliximab biosimilars in naïve patients. Payers seldom actively recommend switching patients – although, again, there is considerable intra-market variability in this. Regions such as Andalucia in Spain, Tuscany in Italy, and Southampton in the UK are all engaged in driving biosimilar adoption, working closely with clinicians to create mechanisms that allow effective switching programs. Figure 5. Guidelines and recommendations Payer driven Regional variation Regional variation Local variation Physician driven Conservative 4 Progressive Prescribing – Quotas Biosimilar prescribing quotas are employed in Germany and Italy (and to a lesser extent in Spain), and are considered more flexible than some of the other controls (eg, exclusive tenders, automatic pharmacy substitution) as they do not restrict clinician prescribing decisions at the individual patient level. But to be effective, the authorities need to implement the right accompanying incentives and penalties for adherence (see case study below). Figure 6. Case Study: Biosimilar prescription quotas exist in Germany and Italy, but are set up and enforced differently Similar levels of discount (~40% vs Remicade list price) Germany High Incentive to meet/ surpass Rx quota Biosimilar infliximab quotas introduced in 2 of 17 regions (from 10%-40%); expected to expand to 15 regions in 2016 Level of switching correlated to quota level Physicians fearful of audits and subjected to financial penalties if quotas are not met Incentive contracts between KKs and physicians stipulating savings sharing if quotas are surpassed Italy Low Incentive to meet/ surpass Rx quota Some regions introduced target infliximab biosimilar quotas, but are currently low (~10%) Physicians reach target quotas with naïve patients only Payers track prescription levels and demand explanations from physicians that fail to comply No financial rewards or penalties in place Dispensing – Automatic Substitution Policies Automatic substitution is seen as the most extreme tool available to payers and is unlikely to be implemented over the short-to-medium term (three to five years). As a nationallevel tool, its implementation would require a strong consensus of originator-to-biosimilar interchangeability among key decision makers, not just with a specific INN but across all biosimilars. To date, only France has implemented an automatic pharmacy substitution policy for biologics, but this only applies to naïve patients and is almost never enforced. 5 Figure 7. Automatic substitution rules across markets Low High Discount Potential Law Prohibits Automatic Substitution Guidelines Recommend Against Automatic Substitution High No Law/Guidelines But Automatic Substitution Occurring Conditional Automatic Substitution Automatic Substitution Low Physician Control Structural Considerations in the Adoption of Biosimilars Each market operates a different framework for funding and decision making, and this structural variability can lead to important differences in the influences and incentives for biosimilar adoption. The way in which cost savings are realized across the different stakeholders is a central consideration. Clinicians and local payers recognise the need to generate savings for their healthcare systems, but unless those savings can be retained – or partially retained – in their organization, there is little incentive to change existing practices. Figure 8. Incentive required to overcome risk of using less established biosimilar and added effort to educate patients Incentive required to convince physicians to change established processes and share responsibility on use of biosimilars Uptake Physician How savings generated by biosimilar use are shared among stakeholders will define the strength of the incentives for biosimilar adoption 6 Market Access Incentive required to establish new policy, pathways, and processes, and impact the interaction with other stakeholders Budget Hospital Reimbursement Savings Sharing Savings Payer In many organizations, savings-sharing mechanisms are already in place (eg, in the UK), but their effectiveness varies – depending on the extent to which the savings are realized “on the ground.” In Italy and Spain, fixed drug budgets are aligned with biosimilar adoption as the savings can be used to fund additional staff, equipment, treatment of additional patients, or the use of innovative new therapeutics. By contrast, in France, where SC anti-TNFs are hospital-prescribed but dispensed and funded outside of the hospital, there are no incentives for clinicians to prescribe the biosimilar alternative, as their institution in no way benefits from the resulting cost savings. Key Insights Price sensitivity to biosimilars currently applies mostly to the naïve-patient segment. ■■ This is the segment that physicians and payers see as being in the target position for recently launched biosimilars ■■ Lack of experience and data on the safety and efficacy when patients stable on the originator are switched to a biosimilar version, not price, is the main barrier to widespread switching Lack of consensus on the interchangeability between originator and biosimilar is reflected across the market access tools employed by payers to drive biosimilar use. ■■ In most markets, nonexclusive tenders are conducted where biosimilars only compete for naïve patients, with payers actively guiding use in this patient population ■■ While a few more progressive organizations are already conducting “winner-takes-all” exclusive tenders, others opt for alternative market access tools such as prescribing quotas that give physicians greater power of choice on an individual patient basis ■■ Automatic pharmacy substitution is seen as a very effective tool for biosimilar adoption but requires national-level consensus on the interchangeability between originator and biosimilar irrespective of the INN; thus it is not likely to be implemented in the near to medium term Structural factors impact how savings generated are distributed across stakeholders, and thus how incentives for biosimilar adoption vary between stakeholder types, impacting uptake. 7 Translating Insights Into Strategy Segmenting your customers beyond discount level, across and within markets, is essential for a successful biosimilar market access strategy Figure 9. Biosimilar Manufacturers Originator Manufacturers Avoid over-discounting with late adopters as this may be a blunt instrument Avoid reactionary discounting in conservative, slow-toswitch markets Use evidence from early adopters to communicate best practices Look for opportunities to partly offset discounts with increased volumes Precision for Value supports resourcing decisions and commercial excellence for global pharmaceutical and life sciences clients through the demonstration and communication of product value and outcomes. Precision has assembled a global team of industry-leading evidence, pricing and market access experts with decades of combined experience in advising clients on their payer strategy across the product life cycle. Combining this experience with our wide-ranging integrated services offers healthcare innovators uniquely robust global pricing, health economics, and market access services. Visit www.precisionforvalue.com for more information. Authors: Andre Vidal Pinheiro, Mansi Vithlani, Kyle Sarnataro, and Alex Grosvenor Alex Grosvenor [email protected] Andre Vidal Pinheiro [email protected] © 2016. All rights reserved.