Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Dysplasia
Dysplasia
• Dysplasia – change of phenotype (size,shape and organization of
tissue)
• is a term used in pathology to refer to an abnormality of
development.[1] This generally consists of an expansion of immature
cells, with a corresponding decrease in the number and location of
mature cells. Dysplasia is often indicative of an early neoplastic
process. The term dysplasia is typically used when the cellular
abnormality is restricted to the originating tissue, as in the case of an
early, in-situ neoplasm
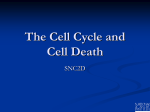
Dysplasia are now usually referred as cervical
intraepithelial neoplasia ( CIN) . They are regarded as
mild, moderate or sever, depending on the degree of
cytological atypia and also the thickness of the
epithelium involved .
CIN I : affecting the deepest 1/3 of the epithelium from
the basal layer up ward
CIN II : Affecting 2/3 of the thickness
CIN III: Affecting full thickness
HPV infection alone and CIN I are grouped together as ‘low – grad
squamous intraepithelial
Lesions (LSIL) and CIN II and CIN III as
‘high –grade SIL (HSIL)
• Microscopic changes
• Dysplasia is characterized by four major pathological microscopic
changes:
• Anisocytosis (cells of unequal size)
• Poikilocytosis (abnormally shaped cells)
• Hyperchromatism (excessive pigmentation)
• Presence of mitotic figures (an unusual number of cells which are
currently dividing).
• Dysplasia is the earliest form of pre-cancerous
lesion which pathologists can recognize in a
pap smear or in a biopsy. Dysplasia can be low
grade or high grade. The risk of low grade
dysplasia transforming into high grade
dysplasia, and eventually cancer, is low.
Treatment is usually straightforward. High
grade dysplasia represents a more advanced
progression towards malignant
transformation.
• Invasive carcinoma is the final step in this sequence. It
is a cancer which has invaded beyond the basement
membrane and has potential to metastasize (spread
to other parts of the body). Invasive carcinoma can
usually be treated, but not always successfully.
However, if it is left untreated, it is almost always fatal.
• Carcinoma in situ, meaning "cancer in place", represents the
transformation of a neoplastic lesion to one in which cells undergo
essentially no maturation, and thus may be considered cancer-like. In
this state, epithelial cells have lost their tissue identity and have
reverted back to a primitive cell form that grows rapidly and with
abnormal regulation for the tissue type. However, this form of cancer
remains localized, and has not invaded past the basement membrane
into tissues below the surface.
Metaplasia
• Metaplasia (Greek: "change in form") is the reversible replacement of
one differentiated cell type with another mature differentiated cell
type. The change from one type of cell to another may generally be a
part of normal maturation process or caused by some sort of
abnormal stimulus. In simplistic terms, it is as if the original cells are
not robust enough to withstand the new environment, and so they
change into another type more suited to the new environment. If the
stimulus that caused metaplasia is removed or ceases, tissues return
to their normal pattern of differentiation. Metaplasia is not
synonymous with dysplasia and is not directly considered
carcinogenic.
•Causes
• When cells are faced with physiological or pathological stresses, they
respond by adapting in any of several ways, one of which is metaplasia. It
is a benign (i.e. non-cancerous) change that occurs as a response to
change of milieu (physiological metaplasia) or chronic physical or
chemical irritation (pathological metaplasia). One example of pathological
irritation is cigarette smoke that causes the mucus-secreting ciliated
pseudo stratified columnar respiratory epithelial cells that line the
airways to be replaced by stratified squamous epithelium, or a stone in
the bile duct that causes the replacement of the secretory columnar
epithelium with stratified squamous epithelium (Squamous metaplasia).
Metaplasia is an adaptation that replaces one type of epithelium with
another that is more likely to be able to withstand the stresses it is faced
with.
DEVELOPMENT OF THE PAP SMEAR
• In 1928 George Papanicolaou initiated the a sampling of vaginal cells,
speculating that these cells would predict which women develop
cervical cancer.
• Together with Dr Herbert Traut , published a monograph in 1947 that
eventually resulted in Pap smears becoming the standard of care in
cervical cancer screening
• The procedure they outlined was modified in 1947 by Ayre,who
collected cervical cells directly using a wooden spatula.
• In1988 ,a workshop was held in Bethesda, Maryland, that provided a
general consensus on how to read Pap smears and initial guidelines
designed to decrease the variability among laboratories in reporting of
result
• A second workshop in 1991 modified these guidelines based on actual
practice and clinical experience
• The Bethesda 1988 and 1991 guidelines both emphasized delineating
SQUAMOUS INTRAEPITHELIAL LESION ---Low grade {LSIL} and high
grade {HSIL}----from atypical squamous cells of unclear significant
{ASC—US}and normal Pap smears.
The Bethesda 2001 consensus panel resulted in the following revisions in
the terminology used to report Pap smear results:
1- Significant changes were made in the management of atypical
squamous cells. The guidelines retained the and added the subcategory of
“ atypical squamous cells favoring HSIL” [ASC-H] . ASC-US carries a
moderately low incidence of CIN 2 or CIN 3 [10%] and very low incidence of
cancer [0.1%],whereas ASC-H is associated with a much higher incidence of
CIN 2 or 3.
• 2- The Bethesda 2001 guidelines also eliminated the categories of
“reactive change Pap smear” and “atypical squamous cells of unclear
significance favoring reactive change Pap smear.
• 3- AGC-US” atypical glandular cell of unclear significance ‘ was
eliminated , primarily to avoid confusion with ASC-US. On average 44%
of women with AGC-US have subsequent tissue examination that yields
a diagnosis of cervical dysplasia, and cancer is diagnosed in 8%.
• 4- The finding of AGC was made more specific in the 2001 guidelines
with the inclusion of two categories:”AGC favoring neoplasia and
“adenocarcinoma in situ”[AIS]
Pap smear Technique and Interpretation
• A- Frequency of screening:
• 1- In USA the most recent recommendation is to screen for the first
time 3 years after the onset of sexual activity Or before age 21
,which ever comes first.
• 2- ACOG recommends annual Pap smear screening /
• AMERICAN CANCER SOCITY recommends every –other-year
screening when using liquid –based cytology
• 3- after age 30 , the interval between screening can be increased to
2-3 years .
• 4- More frequent i.e. annual Pape smears are recommended for
women :
•
a- using DSE
•
b - immunocompromised
•
c- previous history of stage 2 or 3 cervical intraepithelial
neoplsia CIN
D-- INTERPRETATION
• The Bethesda guidelines recommend that 8000—12,000 squamous cells be
obtained for conventional Pap smear but only 5000 cells for a liquid- based
sample
• Cells can obscured by blood , mucous and inflammatory cells
• If more than 75% of the cells are obscured , the sample is inadequate and a new
sample must be tested.
• If 50—75% of the cells are obscured ,the sample is adequate but partially
obscured.
• The presence of endocervical cells [ at least 10] is recommended but not
required in samples from women younger than 40 years of age but required from
women older than 40
1---Negative result
• NILM: negative for intraepithelial lesion or malignancy.
• the normal cells; is optional for the pathologist to add information
about other infection :
• Candidiasis
• Tricomoniasis
• Herpes simplex virus
• Bacterial vaginosis
2--ASC
• The Bethesda guidelines regarding atypical squamous
cells [ ASC ] emphasize the ability to distinguish
between HSIL and LSIL .
• Overall it is thought that 10– 30% of women with a
finding of ASC on a Pap smear have underlying CIN
grade 2 or 3 , and 0.1% may invasive cancer .
•
a--- ASC-US
• It is estimated that 90- 95% of all finding of ASC
fall into this category of ASC-US .
• Women with a Pap smear result of ASC-US have
a 5-7% of having CIN 2 and 3 and 39% of
women with CIN 2 or 3 have a previous
finding of ASC-US on Pap smear
• ASC-US is associated with HPV in about 33- 67%
of cases
b- ASC-H
The category of ASC-H describes atypical cells that are morphologically
suspicious of HSIL but too few in number to qualify as HSIL .
ASC-H is more highly associated with HSIL than ASC-US and is the most
common precursor lesion for CIN . Follow –up of women with a finding
of ASC-H leads to diagnosis of CIN 2 & 3 in 68%.
3--AGC
• Atypical glandular cells is further differentiated according to whether the cells are
:
endocervical
• Endometrial
• Or not otherwise specified.
• This finding is relatively rare ,occurring in 0.17- 1.8% of all Pap smear .
• The presence of these cells has serious medical implications because women with
a finding of AGC have a 9.7 times higher risk of progressing to CIN 2
• a : AGC favoring neoplasia :
•
This finding may correspond with high-grade lesions on tissue examination
[27-96% of the time]
b- Adenocarcinoma in situ [ AIS ] :
It corresponds with high rates of advance lesions on
tissue examination. A finding of AIS corresponds with
high rates of advanced lesions on tissue examination
4– LSIL and HSIL
• Studies have shown that the finding of LSIL is more variable and less
reproducible than HSIL,
and repeatable in only 80% of smear.
Bethesda guidelines further specify [with features suspicious of
invasion ] when histologic evidence supporting cancer is present.
E- counseling women with abnormal Pap
smear
• Women with abnormal Pap smear findings should be counseled that
HPV infection has been linked with the development of cervical
cancer, and that HPV is the most common viral STD , affecting up to
70% of the sexually active population
• Endometritis
A- acute/ apart from infections at operations and by instrumentation it is either
puerperal
gonococcal
The regrowth of new surface endometrium during each cycle prevents the persistence
of any infection which not deep seated can be treated accordingly
B- chronic :
T.B
Senile
other causes
It is a rare disease between the menarche and menopause because of regrowth of
endometrium
It is caused when the uterus is permanently injured or when there is a chance for its
continuously infected like :
foreign body
Malignant disease of the uterus
Infected polyp
Retained gestational products
Chronic salpingio-oopheritis
Pelvic cellulitis from radiation
Endometrial burn due to radiation
• Microscopically there is large collection of plasma cells and f
• Clinical features :
1- purulent discharge from the uterus
2- menorrhagia
IN ANY SIGNS OF INFCETION ---- SEND FOR CULTURE TO EXCLUD T.B
Treatment :
find the cause and treat accordingly
If there is wide spread infection then treat by hysterectomy
Senile endometritis :
The endometrium lose its resistance ,and not shed repeatedly
It may be associated with senile vaginitis
The endometrium infiltrated by macrophages known as foam cells the epithelium
become destroyed lead to granulation tissue that lead to pus exudation if is collect
in the cavity lead to pyomertra , because the cervix is narrow due to senility
atrophied myometrium
The uterus enlarge and become thin , pyrometera may cause
squamous metaplasia or rarely ruptured spontaneously :
• Clinical features:
1- purulent very offensive post menopausal discharge , some times
bloody stained
2- Sometime intermittent discharge
3- uterus is enlarge
D.D:
1- Ca of the uterus
2- if there is pyometra then DO dilatation of the cervix that lead to
drainage of pus+ antibiotics for 1-2 weeks and then do curettage for DD
Treatment : if the patient fit for surgery then hysterectomy after
exclusion of Ca
• UTERINE POLYPS
1- endometrial polyps
usually multiple , and may be apart of hyperplastic endometrium, at
menopause are single or few in number ,
Pathology :
small, pink ,pale projecting from the endometrium ,some time has
long stalk that make it projecting through the cervix or the vulva ,
atypical cellular changes or squamous metaplasia can occur
,adenocarcinoma can occur also
• 2- fibroid polyp :
sub mucosal fibroids can protrude in to the cavity or
pass through the cervix into the vagina
, its surface covered by endometrium ,it cause
spasmodic dysmenorrhea ,menorrhagia ,
3- Adenomayomatous polyp
Contain smooth muscle + endometrial elements
Usually coexist with adenomyosis ,causing heavy
menses but regular, cramping , some time causing
intermenstrual spotting ,malignant changes can occur
with it
• Placental polyp:
It is rare ,due to organization of small retained pieces of
placental tissue, it cause intermenstrual bleeding ,it
may cause sever hemorrhage on removal , treated by
excision , send for biopsy
Asherman ΄s syndrome
• When there is endometrial damage to endometrium ,the whole thickness ,
i.e. beyond the basal layer ,caused by :
1- excessive curettage for retained products , after miscarriage , for 2ndry
PPH
2- T.B ,schistosomasis
3- ENDOMETRIAL RESCTION( ABLATION)
It cause : it cause fibrosis and adhesion
Hypo menorrhea, amenorrhea, infertility
Treatment by :
Resection by hysteroscopy + inert IUCD+ HRT
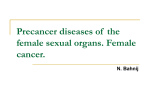
Uterine fibroid
• Definition:
Uterine leiomyoma are benign tumors compose of uterine muscles plus
fibrous connective tissue
• It is common mass in uterus and body
• It is present in 20% of all female
• It is of unknown cause
• It is may be found out side the uterine organ
Vagina , broad ligament ,utero .sacral ligament, vulva,
• Inevitably female sex hormones have been incriminated . Because it is
rarely appear before puberty and after menopause , and there is a
rapid growth during pregnancy, and frequently seen in condition
associated with hyper estrongism that not antagonized by
progesterone like anovulation , end . Polyp , endometrial hyperplasia,
it is more in negros than in white women
• Grossly :
It is firm , round tumor in the uterine wall which is its
self is hypertrophied it has a pseudo capsule which
differentiate it from adenomyosis
Since the blood supply at the periphery so the center is
susptible to degenerative changes ,
ON cutting the tumor is solid, smooth, pinkish or white
, the surface has whorl- like appearance
Microscopically:
It composed of groups & bundles of smooth muscle in a
twisted whorl fashion ,with some connective tissue .
Types:
1- intramural : the most common
2- sub serous myomas: projecting to wards the
peritoneal cavity ± pedicle may reach a large size
without producing symptoms
3-interligamantory tumor
4- sub mucosal
5-cervical
FIBROIDS MAY BE SINGLE OR MULITIPLE
Depending on size, number , location
1- Symptomless
CLINICAL FEATUERS
- Discovered accidentally by abdominal examination ,pelvic examination, U/S, laparotomy,
2- Abnormal uterine bleeding: heavy, prolong
MAY be due to enlargement of uterine cavity by sub mucous fibroids ,or due to increase in vascularity, or due to necrosis of
endometrium overlying the sub mucous myoma,frequently myoma may associated with polyps and endometrial
hyperplasia
3- Intermenstrual bleeding in case of submucuse fibroid
4- pain:
a- reappearance of dysmenorrhea ,congestive type, due to increase vascularity
b- Backache incase of posterior fibroids of moderate size with retroversion
c –colicky pain in case of sub mucous uterus
d- torsion
e- degenerative changes
f- abdominal distention
g- pressure symptoms:
On venacava= edema
On bladder = frequency
Or dyspnea
Degenerative changes:
Due to either arterial , venous , or secondary infections
or malignant transformation
1- hyaline degeneration
2- cystic degeneration
3-red degenerations
4- calcifications
5- necrosis
6- sarcomatous changes
7- infection
Hyaline degeneration the tumor become soft ,and like
jelly ,the cells fused together and become a structure
less esonophilic mass
Liquefaction may occur after menopause lead to cystic
cavity
FAT may be deposited in fibroid with release of fatty
acids then undergo saponification ,Co3 and Po4 in
blood react upon the soppy mass lead to deposition of
CaCo3 and calcium phosphate ͢
Gritty on section of the tissue or
Thin peripheral shall that can be seen by X -ray
Necrosis
Necrobiosis ( Red degeneration)
a- diffuse
b- local
Usually in pregnancy or near menopause that lead to
fibromyomatous pattern,( thrombosis of peripheral
vessels, absence of cell nuclei, the blood vessels
distended and become thin wall and engorged with R.
B. C.s ,the tumor stained red and resemble raw meat ,it
give fishy odor on cutting due to fatty acids, cystic
degeneration may occur in the center and the cyst full
with greasy brown debris
Fatty degeneration
Atrophy
Torsion
Sarcomatous changes that occur in 0.5% of fibroids, 2/3
of sarcoma of the uterus arise from uterine fibroids
Infections
Physical signs and differential diagnosis
• Pelvic or abdominal mass
D.D
- Pregnancy
- Ovarian tumor
- endometrial or cervical polyp
- Adenomyosis
-
Treatment
1- Conservative
For small and no symptoms frequent U/S every 6
months .
2- surgical :
myomectomy :
a- laparotomy
b- laparoscopy
hysterectomy
LH RH agonist
Uterine artery embolisation
ENDOMETRIAL
HYPERPLASIA
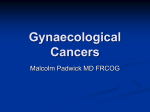
• What is endometrial hyperplasia?
• Endometrial hyperplasia occurs when the endometrium,
the lining of the uterus, becomes too thick. It is not
cancer, but in some cases, it can lead to cancer of the
uterus.
• How does the endometrium normally change throughout
the menstrual cycle?
• The endometrium changes throughout the menstrual
cycle in response to hormones. During the first part of the
cycle, the hormone estrogen is made by the ovaries.
Estrogen causes the lining to grow and thicken to prepare
the uterus for pregnancy. In the middle of the cycle, an
egg is released from one of the ovaries (ovulation).
Following ovulation, levels of another hormone called
progesterone begin to increase. Progesterone prepares
the endometrium to receive and nourish a fertilized egg. If
pregnancy does not occur, estrogen and progesterone
levels decrease. The decrease in progesterone triggers
menstruation, or shedding of the lining. Once the lining is
completely shed, a new menstrual cycle begins.
• What causes endometrial hyperplasia?
• Endometrial hyperplasia most often is caused by excess estrogen
without progesterone. If ovulation does not occur, progesterone is
not made, and the lining is not shed. The endometrium may
continue to grow in response to estrogen. The cells that make up the
lining may crowd together and may become abnormal. This
condition, called hyperplasia, may lead to cancer in some women.
• When does endometrial hyperplasia occur?
• Endometrial hyperplasia usually occurs after menopause, when
ovulation stops and progesterone is no longer made. It also can
occur during perimenopause, when ovulation may not occur
regularly. Listed as follows are other situations in which women may
have high levels of estrogen and not enough progesterone:
• • Use of medications that act like estrogen
• • Long-term use of high doses of estrogen after menopause (in
women who have not had a hysterectomy)
• • Irregular menstrual periods, especially associated with polycystic
ovary syndrome or infertility
• • Obesity
• What risk factors are associated with endometrial
hyperplasia?
• Endometrial hyperplasia is more likely to occur in women
with the following risk factors:
• • Age older than 35 years
• • White race
• • Never having been pregnant
• • Older age at menopause
• • Early age when menstruation started
• • Personal history of certain conditions, such as diabetes
mellitus, polycystic ovary syndrome, gallbladder disease,
or
• thyroid disease
• • Obesity
• • Cigarette smoking
• • Family history of ovarian, colon, or uterine cancer
• What are the types of endometrial hyperplasia?
• Endometrial hyperplasia is classified as simple or
complex. It also is classified by whether certain cell
changes are present
• or absent. If abnormal changes are present, it is called
atypical. The terms are combined to describe the
exact kind of
• hyperplasia:
• • Simple hyperplasia
• • Complex hyperplasia
• • Simple atypical hyperplasia
• • Complex atypical hyperplasia
• What are signs and symptoms of endometrial
hyperplasia?
• The most common sign of hyperplasia is abnormal
uterine bleeding. • Bleeding during the menstrual
period that is heavier or lasts longer than usual
• • Menstrual cycles that are shorter than 21 days
(counting from the first day of the menstrual period
to the first day of the
• next menstrual period)
• • Any bleeding after menopause
• How is endometrial hyperplasia diagnosed?
• Transvaginal ultrasound may be done to measure the
thickness of the endometrium. Thick, it may mean
that endometrial hyperplasia is present.
• The only way to tell for certain that cancer is present
is to take a small sample of tissue from the
endometrium and study it under microscope.
• This can be done with an endometrial biopsy, dilation
and curettage, or hysteroscopy
• What treatments are available for endometrial
hyperplasia?
• In many cases, endometrial hyperplasia can be treated
with progestin. Progestin is given orally, in a shot, in an
intrauterine device, or as a vaginal cream.
• How much and how long the treatment take
• it depends on age and the type of hyperplasia.
• Treatment with progestin may cause vaginal bleeding like
a menstrual period.
• If there is atypical hyperplasia, especially complex
atypical hyperplasia, the risk of cancer is increased.
Hysterectomy
• usually is the best treatment option if the patient do not
want to have any more children.
prevention of endometrial hyperplasia
Taking estrogen after menopause, also need to take
progestin or progesterone.
If menstrual periods are irregular, birth control pills
(oral contraceptives) may be recommended. They
contain
• estrogen along with progestin. Other forms of
progestin also may be taken.
• • If overweight present, losing weight may help. The
risk of endometrial cancer increases with the degree
of obesity