Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
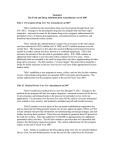
REMS: The New Reality Kuyler Doyle, Principal Consultant, Campbell Alliance Jay Jauregui, Senior Practice Executive, Trade and Distribution Practice Gary Tyson, Senior Vice President, Clinical Development and Medical Affairs Practices Introduction The Food and Drug Administration Amendments Act (FDAAA) of 2007 ushered in an increase in regulatory authority for drug safety enhancement, including the power to require post-approval studies or clinical trials, label changes, or implementation of a Risk Evaluation and Mitigation Strategy (REMS). Since implementation, the number of products requiring REMS programs has continued to rise. Pharmaceutical and biotechnology companies are realizing that the new restrictions from REMS programs are a permanent part of the industry landscape and that they must adapt accordingly. This article highlights the challenges of the new regulatory restrictions, lists potential competitive advantages to these programs, and describes how organizations need to adjust to the evolving risk mitigation landscape. History of Risk Minimization Programs Withdrawals of several high profile drugs from the market elevated concerns about pharmaceutical product safety and increased public scrutiny of FDA practices. In response, Title IX of the FDAAA amended the Federal Food, Drug, and Cosmetic Act (FDCA) to authorize the FDA Secretary to require a REMS program on any product, pre- or post-marketing, if deemed necessary to ensure that the benefits of the drug outweigh its risks. Although this increased regulatory authority appears to be a paradigm shift, drug risk management has evolved over the course of several decades. The original FDCA of 1938 allowed drugs to be marketed once proven to be safe. However, birth defects associated with thalidomide in Europe and Canada during the late 1950s and early 1960s led to the passage of the Kefauver-Harris Amendments in 1962, requiring companies to demonstrate efficacy in addition to safety in order to be marketed. Since then, the FDA process of approval has been founded on a favorable benefit to risk ratio. Table 1 – Modern Risk Minimization Tools Attribute RiskMAP REMS Dates of Activity 2003 to 2007 2007 to present Goals Steps to achieve specific goals and objectives to minimize product risks, while preserving benefits Steps to ensure that the benefits of the drug outweigh the risks Author FDA Congress Key Documentation Premarketing Risk Assessment, Good Pharmacovigilance Practices and Pharmacoepidemiologic Assessment, and Development and Use of Risk Minimization Action Plans, 2005 (finalized) Food and Drug Administration Amendments Act (FDAAA), 2007 Impact on Manufacturers Suggested Mandatory Non-Compliance Penalties None Fines and Possible Injunction Throughout the evolution of risk management, special programs were instituted on a case by case basis for specific drugs as deemed necessary. Early examples emphasized the communication of risks to stakeholders. Initially, prescribers were the primary target of this information in the form of product labels, “Dear Healthcare Provider” letters, or black box warnings. Subsequently, drug makers were required to educate patients regarding product risks, initially in the 1970s through patient package inserts (PPI) that were first implemented with oral contraceptives, and in the late 1990s with mandatory medication guides for select drugs that were distributed to patients at the time of dispensing and included information required for safe and effective use. The FDA implemented its first program that restricted drug access in 1990 with the “no blood, 1 no drug” campaign for clozapine that required a patient blood count to test for agranulocytosis prior to dispensing. In 1998, the FDA approved the use of the teratogenic drug thalidomide, the very product that led to the increased burden of proof for market approval, to relieve complications from leprosy. Drug manufacturer Celgene developed a strict program called the System for Thalidomide Education and Prescribing Safety (S.T.E.P.S.®) in which only registered physicians could prescribe the drug, and then for only one month intervals. Further, pharmacist registration was required to dispense the product, women of childbearing age had to undergo mandatory pregnancy tests, and both men and women had to adhere to birth control methods. Subsequently, REMS: The New Reality Table 2 – Consideration Factors for REMS Requirement Market Stage Factors Size of the population likely to use the drug Seriousness of the disease Expected benefit of the drug with respect to disease Expected duration of treatment Seriousness of known or potential adverse events related to the drug Whether drug is a new molecular entity Pre-approval ew safety information deems a strategy is necessary to ensure the N benefits outweigh the risks “New safety information” may be derived from a clinical trial, an adverse event report, a post approval study, or peer reviewed literature Post-approval Table 3 – Elements of REMS Element Access Education Assessments Description Timetable for Submission of Assessments of the REMS equired of all REMS R Assess by 18 months, by 3 years, and in 7th year after REMS approval FDA may increase frequency of assessments or eliminate requirements after 3 years Assessment within 15 days for cause Medication Guide or PPI edication guides are distributed to patients when drug is dispensed M Patient package inserts may be required if they might help mitigate serious risks of the drug Communication Plan to Healthcare Professionals ecessary when FDA determines a plan may support implementation of N an element of REMS May be through letters to healthcare providers or through professional societies about drug risks and safety protocols Elements to Assure Safe Use (ETASU) E TASU need to be commensurate with risk Must be posted publicly within 30 days of being imposed with an explanation of how elements will mitigate risk Will not be unduly burdensome on patient access (due to life threatening diseases or difficulty accessing healthcare) To the extent practicable, should minimize the burden on the health care system and should be compatible with current distribution system ETASU options: Prescribers must have training or certification Pharmacies, practitioners, or healthcare settings that dispense the drug must be certified Drug must be dispensed only in certain healthcare settings Drug is dispensed to patients only with documentation of safe-use conditions, such as laboratory test results Patients must be subjected to monitoring Patients must enroll in a registry Implementation System ay by required to monitor and evaluate implementation of ETASU eleM ments by those responsible, and to work to improve implementation 2 thalidomide has been found to be effective for other indications as well, including multiple myeloma, and the S.T.E.P.S. program continues to be in use. Programs such as S.T.E.P.S. helped pave the way for the modern era of risk minimization. Following the Prescription Drug User Fee Act (PDUFA) and attempts at shortened review cycles, there were concerns about the marketing of products prior to being fully vetted as safe. In response, the FDA established a new risk management system with PDUFA III in 2002, and published final guidance for its Risk Minimization Action Plan (RiskMAP) in 2005. The goal of the RiskMAP was to elevate the appropriate use of products and to decrease adverse events. Sixteen accepted RiskMAPs were carried over and deemed approved REMS when the FDAAA went into effect in March of 2008. In fact, many of the post-marketing elements that define REMS programs also made up RiskMAPs, including the education of patients and physicians and restricted access, although there are also distinct differences (Table 1). While RiskMAPs were voluntary, the FDA now has the ability to mandate these restrictions based on the powers provided in the FDAAA amendment, and can impose fines of up to $250,000 per violation on manufacturers for non-compliance. Components of REMS Programs A REMS can be required of any manufacturer in all stages of development, including pre-licensure, review, and post-market. To determine if a REMS is needed, the FDA examines risks for serious side effects, potential for misuse of the drug, and whether off-label usage needs to be minimized. During the drug review process, the FDA will consider the amount of information known on the product or drug class in relation to the size of the target population, treatment length, number of reported adverse events, and severity of the indication to be treated (Table 2). REMS may be requested of products that are already on the market due to reports of adverse events via post-marketing surveillance, or due to safety concerns arising from new data from phase 4 studies or literature reviews. All REMS must include a timetable for submission of program assessments, which are required to be completed by 18 months, 3 years, and in the 7th year. The other REMS elements vary at a level commensurate to the risk anticipated by the FDA, and may consist of education-based mandates or elements to ensure safe use (ETASU)(Table 3). Figure 1 – Four Tiers of REMS Complexity Less Severe More Severe Minimal Low T imetable for submission of assessments Medication guides or patient package inserts Specific package insert language Periodic adverse events reports and continuous monitoring C ommunication plan to disseminate safety information to healthcare providers Educational material packages Patient acknowledgement forms (e.g., understanding of risk) Follow-up surveys to assess the educational program Educational elements can contain requirements for medication guide outreach, PPI, or the need for a communication plan to healthcare providers. ETASU include access restrictions via patient testing or screening for eligibility, patient registry and tracking, prescriber training or certification, and drug distribution limited to certified pharmacies or healthcare settings. REMS programs may further require approval of an implementation system to monitor and evaluate ETASU execution. Based upon the severity of the requirements, REMS generally fall into one of four tiers in severity (Figure 1). As perceived risk with the drug increases, the complexity of the REMS elevates accordingly. While most REMS programs required thus far have fallen into the “minimal” category and nearly 75% have required only medication guides (Figure 2), complex REMS have also been employed. The drug Entereg® (Adolor and GSK) facilitates healing following bowel resection, but is required to have the most severe form of REMS where access is controlled due to evidence of increased ischemic cardiovascular events. The manufacturers established the Entereg Access Support and Education (E.A.S.E.™) program, which restricts drug dispensing to only registered hospitals and tracks the patient to limit the duration of therapy. Advanced Complex Certification and training of prescribers Certification and training of pharmacists and site-of-service staff Recertification and product release approval at each dispense Limited distribution to only registered sites of service (e.g., hospitals) Regular audits of prescribers and dispense locations Not only does the FDA have the power to require REMS for individual products, it can also mandate REMS for entire drug classes. This power has been exercised for fluoroquinolone antimicrobials, requiring label changes and medication guides. In February 2009, the FDA notified manufacturers of opioid drugs that a class-wide REMS was in development. Due to the tens of millions of prescriptions written for opioid drugs each year, implementing a REMS for this drug class will be a massive undertaking. Other classes of drugs discussed as possibly requiring REMS are the erythropoietins, tumor necrosis factor blockers, antidepressants, botulinum toxins, and anti-epileptics. Challenges of REMS Although an increased focus on drug safety is a positive advancement, the new regulatory authority provided to the FDA certainly poses challenges to drug manufacturers and can obviously impact the bottom line (Table 3). As the requirements for REMS programs are still relatively new, they add an additional layer of preparation and uncertainty into the regulatory process for new drugs. Also, REMS negotiations can assign additional time to the approval process and lead to costly launch delays. 3 P atient screening Patient enrollment into registries Patient record audits (e.g., duration of therapy limits) Implementation systems In addition to revenue impact from a delayed launch, there are also clear and significant costs associated with these programs. In its simplest form, medication guides to satisfy REMS requirements add substantial costs for production and dissemination. Effective training programs may need to be developed and employed for healthcare providers. Maintaining patient and physician registries is not a trivial feat, and will require expenditures for software to manage and track confidential data. Registries will also necessitate budgeting for full time employees or contractors to design, implement, and administer. Further, scheduled REMS assessments require sponsors to reveal that their program is effective. The assessments need to demonstrate whether the ETASU are meeting their goals, so these data will have to be tracked and analyzed. The more rigorous the REMS program becomes, access is increasingly restricted to patients, likely shrinking volume in sales. Even the lightest REMS requirements, medication guides, can be a burden on prescribers when they include a patient-physician agreement to sign. The additional paperwork associated with REMS can dissuade physicians from prescribing the product. Further, REMS that include limits to distribution or duration of therapy can lead REMS: The New Reality Figure 2 – Profile of Accepted REMS Programs to a reduction in revenue, making the product less commercially attractive to the manufacturer. Potential Advantages 100% 80% 60% 40% 20% 0% MG Only MG + CP MG + ETASU + IS MG + CP + ETASU + IS CP + ETASU + IS MG = Medication Guide ETASU = Elements to Assure Safe Use CP = Communication Plan IS = Implementation System Note: n=89. Data obtained from FDA website November, 2009 When properly planned and executed, REMS programs can also offer some potential advantages (Table 4). First, through its mandated programs to improve drug safety, REMS has provided the ability for the FDA to approve products that likely would have never made it to market. Patients with indications that have high unmet needs desperately want new medications, and are frequently willing to accept some risk for the potential benefits. In requiring both the patients and physicians to be well versed with the risks associated with the products, the FDA is allowing these medications to move forward by making sure the practitioner and patient fully comprehend correct use of the product as well as possible outcomes. At the same time, a clearer understanding of proper usage of the drug can lead to increased adherence, helping to maintain sales while potentially reducing the risks associated with improper use. REMS programs allow organizations to establish relationships via registries with two key stakeholders, patients and physicians. Up-to-date patient registries allow active monitoring of drug usage, Table 3 – REMS Challenges Challenge Description How to Prepare Regulatory Uncertainty EMS requirements are relatively new, and add an R additional layer to the approval process Can lead to delay of launch , thereby reducing revenue P roactively plan for REMS and communicate with regulatory officials during development Plan REMS programs early enough to avoid approval delays Costs Associated with REMS Programs EMS programs will increase costs R Tracking patient information will require management software and full time employees I ntegrate REMS planning into the organization and design SOP around the activities that emphasize efficiencies Design REMS programs that specifically match program activities with drug risk to minimize scale of the program Paperwork Can Dissuade Healthcare Providers from Prescribing I ncreased REMS complexity expands the requirements for healthcare providers to track patients, amplifying workload More work for prescribers can dissuade drug use, thereby reducing sales E stablish a knowledgeable and dedicated group that can design effective REMS programs with the stakeholders in mind to minimize burden 4 Table 4 – Potential REMS Advantages Advantage Description How to Benefit Ability to Market Drugs with Some Safety Risk EMS provides ability for FDA to approve products R that likely would not have made it to market Requires patients and physicians to be fully aware of the drug and its risks P rovides a means to fulfill unmet needs in the market Clearer understanding of safe use of the drug could lower risk and maximize benefit, thereby increasing adherence Ability to Establish Relationships with Stakeholders EMS requirements for registration or training of R patients and physicians provides an opportunity to establish a relationship with key stakeholders eep stakeholder needs in mind when developing K REMS programs When done effectively, can provide positive impact on the brand and the drug manufacturer Complex REMS Could Lengthen Life Cycle eneric entrants are required to establish a single G shared REMS system for ETASU unless burdensome or patented Access restrictions could make it difficult for generic manufacturers to obtain product for equivalency testing evelop a novel, distinguishing REMS program that D contains unique components with potential for intellectual property adherence, and adverse events. Interestingly, patient registries also share many aspects in common with health management or support programs developed for some specialty drugs. As such, REMS registries provide an opportunity for companies to establish a connection with patients through personalized interactions regarding adherence and safe use or by setting up web portals for peers who are undergoing the same treatment and who are looking for relevant information regarding their disease and therapy. When carried out effectively, these programs can build communities that foster brand loyalty. In a time when therapeutic areas are becoming increasingly crowded, patients and physicians have options for their product of choice. A well designed REMS registry and information network can be an effective means of brand differentiation and could, depending on the level of unmet need, potentially allow for premium pricing to offset the costs of the program. Distinguishing factors within REMS programs will also come into play when class-wide REMS are required. Although many view REMS that limit distribution as measures to restrict access, they could also in effect increase the lifecycle of a drug. Restrictive REMS hold the potential to stave off generic competition, as they may find the space less attractive due to the complex and costly programs. The FDAAA states that upon generic entry, the new competitor must use a single, shared system of ETASU with the originator product. This requires generic manufacturers to work with the innovator companies to establish the single system, or request a waiver for this requirement if the burden of creating it outweighs the benefits. Another potential to waive the single system requirement comes if the innovator company has active patents related to their novel risk mitigation plans, and the generic manufacturer is unsuccessful in obtaining a license to use aspects of the ETASU. Some companies have already filed patents for elements of their risk mitigation programs, such as patient screening algorithms, and a novel REMS program could remain a barrier to entry, point of market differentiation, or source of revenue through license agreements. Further, the limited product distribution imposed by REMS can make it difficult for generic competitors to acquire the drug in order to perform the comparative evaluations required for the abbreviated approval process, as already seen with Celgene’s Revlimid®, thereby delaying entry into the market. How to Adapt Although Title IX of the FDAAA provides authority to ensure post-market drug safety, there is likely to be increasingly less uncertainty surrounding the need for REMS requirements for new drugs, and 5 companies will be required to take a close look at safety issues earlier in the development process. To adjust to the emerging risk mitigation environment, pharmaceutical companies need to alter their outlook, preparation, and execution of REMS. Outlook To minimize the possibility of regulatory delays due to REMS negotiations, organizations need to adopt a proactive outlook toward risk mitigation rather than a reactive one. Manufacturers should pursue pre-submission interactions with regulatory officials during the development process to limit late surprises that could impede launch. Pre-submission interactions with the FDA will allow discussions of drug safety profiles that could inform product managers regarding needs for appropriate REMS requirements. Organizations must assess the impact of REMS activities on all stakeholders when developing potential REMS programs. As REMS requirements could potentially be used for competitive advantages, the pursuit of novel programs that benefit patients and physicians while minimizing the paperwork burden could be beneficial. The formation of a knowledgeable and dedicated group to design effective and innovative REMS could afford organizations the ability to develop programs that set the bar for a drug class. REMS: The New Reality Preparation Since the development and negotiation of REMS programs can require a considerable amount of time, companies need to initiate preparation for a REMS proposal early in new product planning. If clinical trials suggest that there may be some safety issues that the FDA will scrutinize, the manufacturer should assume they will need a REMS program. Analysis of FDA actions related to the prior negotiation and approval of REMS programs will help to plan proposals for pipeline products. REMS should be designed to match associated risks of the drug with specific activities, thereby keeping the scope of the program in check to control costs. Marketing will need to determine how a proposed REMS program would likely affect the revenue forecast and commercial viability of a product. Planning ahead will help alleviate the challenges associated with late stage design and negotiation of a complex REMS. Execution As REMS programs appear to be a part of the permanent regulatory process, organizations must also improve the ability to assess, plan, and implement programs by integrating them into the company DNA and making them part of a new routine. Clearly the clinical, regulatory, safety, distribution, marketing, sales, and medical affairs functions need to be involved in REMS scenario planning for new products. Although committees that develop REMS programs will be cross-functional in nature, a permanent “home” for the management of activities must be established within the organization and a standard operating procedure (SOP) developed. Inclusive discussions with internal stakeholders to define the SOP will define roles and responsibilities for REMS development and facilitate buy-in to the protocol, a requirement to make REMS execution an efficient process. Companies must also define REMS activities that will be performed in-house versus outsourced, and vender partners must be established. A means to monitor REMS effectiveness must also be generated, including the ability for sales and medical affairs field teams to report back on prescriber sentiments towards requirements. Efficiencies in REMS design and execution will further help provide credibility to the FDA that can facilitate future program negotiations and minimize costly delays. Conclusion REMS is clearly part of the new landscape of the pharmaceutical industry. Companies must accept this reality and adjust their organizations accordingly. Comprehension of the potential REMS triggers, www.campbellalliance.com (888) 297-2001 6 the program approval process, and early planning will help alleviate some of the challenges posed by a complex REMS and will help avoid costly delays to drug approval. Companies need to integrate REMS development as a permanent part of the organization and work to create a SOP that will allow for best practice development in the assessment, planning, and implementation of programs. A full appreciation of the impact of REMS requirements on key stakeholders is critical to the generation of programs to reduce risk while remaining commercially viable. Through establishment of skill sets needed to understand and generate effective REMS programs, companies will be able to capitalize on potential competitive advantages of a well-designed REMS, despite the associated challenges. Note This white paper is being offered as a background article in preparation for the public release in early 2010 of Campbell Alliance’s survey results regarding the “State of REMS Today.” The survey will provide a snapshot of how companies across the industry are currently planning and executing REMS programs. To set up a time for us to share the results of this research, please contact Gary Tyson. Gary Tyson [email protected]