Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
[CANCER RESEARCH 49, 3104-3108, June 1, 1989]
Correlation between Long-Term Survival in Breast Cancer Patients and
Amplification of Two Putative Oncogene-Coamplification Units:
hst-ll int-2 and c-erbE-2/ear-l1
Hitoshi
I suda,2 Setsuo Hirohashi,3 Yukio Shimosato,
Teruyuki Hirota, Shoichiro Tsugane, Hiroshi Yamamoto,
Nobuyuki Miyajima, Kumao Toyoshima, Tadashi Yamamoto, Jun Yokota, Teruhiko Yoshida, Hiromi Sakamoto,
Masaaki Terada, and Takashi Sugimura
Pathology, Epidemiology and Genetics Divisions, National Cancer Center Research Institute [H. T., S. H., Y. S., T. H., S. T., J. Y., Te. Y., H. S., M. T., T. SJ,
Department of Surgery, National Cancer Center Hospital [H. Y.]; 5-1-1 Tsukiji, Chuo-ku, Tokyo 104, and Institute of Medical Science, University of Tokyo [N. M.,
K. Y., Ta. Y.]; 4-6-1 Shiroganedai, Minato-ku, Tokyo 108, Japan
ABSTRACT
The incidence and association
with 10-year survival of amplificai inn
in five protooncogenes or transforming genes were retrospectively ex
amined using DNAs extracted from formalin-fixed, paraffin-embedded
blocks of tissues obtained from 176 consecutive patients surgically treated
for primary breast carcinoma. The incidences of greater than threefold
amplification of hst-l, ¡nt-2,c-erbB-2, ear-1 (one of c-erb\), and c-myc
were 12, 13, 16, 10, and 4.0%, respectively, hst-l and ¡nt-2were almost
always coamplified (21/22), while c-erftB-2 and ear-1 were frequently
coamplified (18/28) with almost the same copy number. The hst-l and
int-2 pair and the c-erAB-2 and ear-1 pair, localized on chromosomes
Ilql3 and 17q21-22, respectively, in normal cells, were inferred to be
constituents of different amplification units. Amplification of hst-l and/
or ¡nt-2was detected preferentially in the younger age group, and was
correlated with poorer prognosis in cases carrying four or more copies of
the genes. Amplification of c-erbB-2 and/or ear-l was strongly correlated
with poor prognosis in all 176 patients, especially those with lymph node
metastasis. Amplification of c-myc was also correlated with poor prog
nosis. Cox's life-table regression analysis showed that amplification of cerbtt-2
had a prognostic
value, which was independent
of other known
prognostic factors such as lymph node status and tumor size.
INTRODUCTION
In the chromosomes of human cancer cells, homogeneously
staining regions and double minutes are frequently found, and
are believed to represent sites of gene amplification. Since each
amplified DNA sequence is considered to be a unit of several
hundred kilobase pairs (1), it is possible that two oncogenes
localized very closely together on a chromosome may be con
tained in a single amplification unit. In fact, two sets of ampli
fication units containing two oncogenes or transforming genes
are known in human cancers, namely, hst-l and int-2, and cerbB-2 and ear-l (2-5).
hst-l is a transforming gene that has been isolated from two
stomach cancers and from a noncancerous portion of stomach
mucosa of a cancer patient using the NIH/3T3 transfection
assay (6). No viral counterpart of this gene has yet been iden
tified. In human genomic DNA, hst-l is localized on chromo
some 1Iql3 and its locus is very close to that of the int-2 gene
(3). The int-2 gene was first detected in mouse mammary
cancers caused by MMTV4 and its human homologue has been
Received 6/20/88; revised 11/14/88, 1/31/89; accepted 3/2/89.
The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement in
accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1This study was supported in part by a Grant-in-Aid from the Ministry of
Health and Welfare for the Comprehensive Ten-year Strategy for Cancer Control,
Japan, and by a Grant-in-Aid for Scientific Research from the Ministry of
Education, Science and Culture, Japan.
2 Awardee of a Research Resident Fellowship from the Foundation for Pro
motion of Cancer Research.
3To whom requests for reprints should be addressed.
4 The abbreviations used are: MMTV, murine mammary tumor virus; CPA,
cyclophosphamide; 5FU, 5-fluorouracil; TNM, primary tumor (T)-nodal involve
ment (N)-distant metastasis (M).
identified on chromosome Ilql3 (7). This gene is considered
to be involved in murine mammary carcinogenesis and its
activation is partly due to integration of the MMTV provirus
genome within it (8). Since the deduced amino acid sequence
of the hst-l product is homologous to those of human fibroblast
growth factors, which are wide-spectrum mitogens, and also to
that of the int-2 protein, all are considered to constitute a gene
family that is involved in cell growth (9). Amplification of hstl is occasionally detected in human cancer tissues and, in all
cases examined up to now, is always accompanied by amplifi
cation of int-2 gene (2, 3).
On the other hand, c-erbB-2 and one of the v-er¿>A-related
genes, ear-l, are localized on chromosomes 17q21 and 17q2122, respectively (5, 10). c-erbB-2, a v-eroB-related gene, is
homologous but not identical to c-erbB-l, and encodes a growth
factor receptor-like molecule (11). ear-l has been cloned from
a cDNA library constructed from mRNA of the human fibro
blast line TIG-1.5 There are multiple c-er¿>A-relatedgenes lo
calized on different chromosomes in the human genome (12).
Recently, the sequence of the \-erbA gene product has been
revealed to be similar to those of the human glucocorticoid,
estrogen and thyroid hormone receptors (12, 13). It has been
reported that the c-erbB-2 gene and one of the c-erbA genes are
often coamplified in both breast carcinoma and tubular adenocarcinoma of the stomach (4, 5).
The biological significance of coamplification of these genes
has not been clarified. It is thus considered very important to
examine the association between gene amplification in cancer
tissue and the prognosis of patients in order to elucidate the
biological role of oncogenes and/or transforming genes.
In human breast carcinomas, amplification of the c-erbB-2
gene has been detected in 10-30% of cases (14). The question
of whether this amplification of c-erbB-2 is correlated with
aggressive clinical behavior of human breast cancer is currently
controversial (14, 15). Its clear association with shorter overall
and disease-free survival time has been shown only by Slamon
et al. (15). Since one of the characteristics of human breast
cancer is its relatively long clinical course after diagnosis,
follow-up for more than 10 years seems to be necessary in order
to discuss the prognosis of affected patients. In the present
study, using DNAs extracted from formalin-fixed, paraffinembedded tissue blocks, we retrospectively examined the inci
dence of amplification and coamplification of five genes, hst-l,
int-2, c-erbB-2, ear-l, and c-myc, and their correlation with
clinical parameters such as age, tumor size, lymph node status,
and disease-free and overall survival in 176 patients with breast
carcinoma for whom it has been possible to follow-up the
postoperative course for more than 10 years.
5 N. Miyajima, unpublished
data.
3104
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1989 American Association for Cancer Research.
ONCOGENE «¡AMPLIFICATION IN HUMAN BREAST CANCER
MATERIALS
regression model (proportional hazards general linear model) and the
SAS program package (SAS Institute Inc., Cary, NC) (25, 26).
AND METHODS
Patients. We selected 176 female patients with primary breast carci
noma that had been consecutively treated by radical or palliative mas
tectomy at the National Cancer Center Hospital, Tokyo, Japan, be
tween December 1974 and October 1976. Radical surgery was per
formed on 164 patients and palliative surgery on 12 patients, the latter
comprising three Stage III and nine Stage IV cases. The subsequent
systemic treatment regimen was mainly chemotherapy. No adjuvant
chemotherapy had been done for 41 Stage I cases, 20 Stage II cases,
and three Stage III cases. The others, namely, 20 Stage I cases, 65
Stage II cases, 18 Stage III cases, and all nine Stage IV cases had been
treated by single-agent chemotherapy using CPA, 5FU or FT207, or
by combination chemotherapy using two to five agents among CPA,
FT207, 5FU, mitomycin C, doxorubicin, methotrexate, vincristine, and
prednisone. Antiestrogen therapy with tamoxifen had not been intro
duced at that time, and androgen therapy or oophorectomy was per
formed in only a few cases. No data on estrogen or progesterone
receptors was available. Sufficient follow-up data were available for all
examined cases; 10 years after the initial operation, 101 patients were
alive, 60 had died from relapsed breast carcinoma and 15 patients had
died of other causes (two of rectal cancer, one of thyroid cancer, one of
hepatitis and 11 of unknown cause). Among these IS patients, only two
had died carrying active breast carcinoma. All cases were classified
according to the clinical TNM stage, the size of the tumor and the
degree of lymph node metastasis. Four clinical TNM stages (I-IV) are
established (16). The tumors were divided into three groups on the
basis of size, i.e., 2.0 cm or less in diameter, more than 2.0 cm to 5.0
cm, and greater than 5.0 cm. The degree of lymph node metastasis was
microscopically determined and divided into three groups according to
the number of metastasis-positive lymph nodes, i.e., no metastasis, one
to three positive nodes on the ipsilateral side, and four or more positive
nodes, including four cases of Stage IV without curative lymph node
dissection. Patients were divided into two groups according to age; 50
years or younger, and 51 years or older.
DNA Extraction and Slot-blot Hybridization Analysis. We extracted
DNA by a previously described method from small samples of formalinfixed, paraffin-embedded blocks of each primary tumor and nonneoplastic tissue (resected lymph node or muscle), which had been resected
from the 176 patients and stored at the National Cancer Center Hos
pital (17). By examination of hematoxylin and eosin-stained tissue
sections from each case, we confirmed whether an adequate volume of
cancer tissue was present in the samples. Slot-blot hybridization analy
sis was performed using these DNAs following the method previously
described (17). Probe DNAs used were hsl-l (0.59-kilobase/ivaI ORF1
fragment), int-2 (0.9-kilobase Sad fragment), c-erbB-2 (4.7-kilobase
Dra\ fragment), ear-l (2.1-kilobase £coRI fragment), and c-myc (1.5kilobase, Clal-EcoRl fragment) (5, 7, 18, 19). As the internal controls
for one copy, pE4b-TGH2, a 3.5-kilobase ///»dill fragment on chro
mosome 11q22-q23 (D 11S24), pHF-12-2, a 0.24-kilobase BamHl frag
ment on chromosome 17p (D17S1) and c-mos, a 2.7-kilobase £ce>RI
fragment on chromosome 8 were used (20-22). Serially diluted DNA
extracted from the MKN-7 cell line, in which the c-erbB-2 gene is
amplified by 30-fold, was used as a standard (10). The method used for
calculating the copy number was described previously, and the copy
number was expressed as that per haploid DNA (17). Only those signals
with an intensity of three copies or more were considered to represent
amplification.
Statistical Analysis. We evaluated the incidence of amplification of
each gene in each group for patient age, TNM stage, tumor size, and
lymph node status. The results obtained were analyzed for statistical
significance by the x2 test. Survival curves of patients with gene ampli
fication and those without it were compared. Overall survival curves of
the 176 patients including those who had died of other diseases or
unknown causes were drawn by the Kaplan-Meier method (23). Diseasefree survival curves were drawn for the 164 patients who had undergone
radical surgery. Statistical difference between survival curves was cal
culated using the logrank test (24). The independent prognostic effects
of gene amplification and other clinical parameters that seemed to be
important as prognostic factors were analyzed using Cox's life-table
RESULTS
A\f-l and int-2 Coamplification in Breast Carcinoma. The list1 and int-2 genes were amplified in 21 cases (12%) and 22 cases
(13%), respectively (Table 1). In all 21 cases with amplification
of hst-l, int-2 was coamplified with almost the same copy
number, ranging between three and 12 copies (Fig. 1, Cases A
to C). In only one case, int-2 was independently amplified 6fold (Fig. 1, Case D). The incidence of amplification of hst-\
and/or int-2 was significantly higher in the younger age group
(P = 0.02, Table 2). However, there was no association between
the incidence of hst-l and/or int-2 gene amplification and TNM
stage, lymph node status, or tumor size (Table 2). Although
overall survival and disease-free survival did not show obvious
tendency to be poorer in all 22 cases with hst-l /int-2 amplifi
cation in comparison with the other cases (P > 0.10 and >0.10,
respectively), the groups with an hst-l /int-2 copy number of 4
or more (13 cases) showed poorer prognosis than the other
groups: the difference in the curves for overall survival was
nearly significant (P = 0.068, Fig. 2A), and the difference in
Table 1 Incidence of amplification of the hst-l, int-2, c-erbB-2, ear-l, and c-myc
genes in 176 cases of breast carcinoma
Number of cases
No amplifiThree
Four
2Five
Total ampliGene
cation
copies
copies
copies
fied cases
(12%)°22(13%)28(16%)18(10%
hst-\int-2c-erbB-2ear-lc-myc155154148158169994318896245159421
(4%)
' Numbers in parentheses, percentages of cases with gene amplification.
hst-1
N
B
T
IN
T
N
lnt-2
3x
C-erta^ ear-1
3x
„„
«•-
3x
16
•* 8x I
pHF" _P"¡2
16 —
8x
6x
8x
N
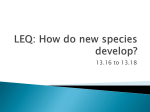
Fig. I. Slot-blot hybridization analysis of DNAs extracted from formalinfixed, paraffin-embedded tissues of six cases of breast carcinoma (A to /•
). DNAs
were extracted by the method previously described (17). Ten->ig samples of DNAs
were applied to BA85 nitrocellulose filters (S&S, Keene, NH), hybridized to "Plabeled probe DNA, washed, autoradiographed and evaluated as previously de
scribed (17). T, DNA from primary breast carcinoma tissue; N, DNA from
nonneoplastic tissue. A and B, cases with amplification of Mr-1. int-2, c-erbB-2,
and ear-l; C, a case with amplification of Mr 1 and /nf-2; D, a case with
amplification of int 1 alone; £,a case with amplification of c-erbB-2 alone; F, a
case without any amplification. The copy numbers of amplified genes are shown
to the right of the hybridized signals of the samples. The signals hybridized with
pHF-12-2 and pE4b-TGH2 represent single copy numbers of chromosomes 17
and 11, respectively. T, tumor; N, normal tissue.
3105
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1989 American Association for Cancer Research.
ONCOGENE COAMPLIFICATION IN HUMAN BREAST CANCER
Table 2 Associationbetweenhst-1, int-2, c-erbB-2,and ear-1 amplificationand
diseaseparameters
were higher in older patients, at Stages III and IV, with a tumor
size of more than 5.0 cm, and with four or more metastatic
casesFactorsAge<50TNM
Number of
nodes, but these differences were not statistically significant
(Table 2). There was no significant association between copy
hst-l/int-2
c-erbB-2/ear-l8(13%)
number110 P"-»19(17%)!
number of c-erbB-2 and number of lymph nodes with metasta
sis.
002
"('-"-6
3(5%) J
Compared with the other cases, overall survival was poorer
666185219747626725450Amplified
in all three groups showing amplification, i.e., in 28 cases with
stageIIIIIIrvTumor
c-erbB-2 including 18 ear-1-amplified cases (P < 0.0005), 18
T11(13%)!
(10%)
T12(14%)
cases
with ear-l amplification (P < 0.01) and 10 cases with
...ci5(24%)
16(29%)
"-'0(0%) f
amplification of c-erbB-2 alone (P < 0.02). As for the 164
f2
J7(9%)
J11(22%)
patients who had received radical surgery, disease-free survival
was significantly shorter in 24 with c-erbB-2 amplification than
(cm)£2.02.1-5.0>5.1Number
size
111
110(13%)
(15%)
in the other 140 without it (P < 0.025). The overall survival
NS4(15%)J-\10(14%)5
(14%) }>1
rate and disease-free survival rate for patients with c-erbB-2
J-v8(11%)
(27%)
amplification dropped abruptly to 46 and 50%, respectively,
positivelymph
of
within 4 years after surgery. In the group with no amplification
nodes01-3>3Total
of c-erbB-2, the survival rate dropped gradually to 71% for
I9(17%)
NS7
(9%) }•
overall survival and to 64% for disease-free survival during the
\11
(14%) JAmplified
(22%) JfNSNIC*C^BNSNS
10-year period. The copy numbers of amplified c-erbB-2 and
°P was calculated by x2 text.
ear-l
genes were also associated with patient prognosis: cases
* The x2 test was done to test between Stages I + II and III + IV. Parentheses:
with more than four copies of c-erbB-2 showed much poorer
percentages of cases showing amplification. NS, not significant.
prognosis for both overall and disease-free survival (P = 0.0002,
Fig. 3A, and P < 0.01, Fig. 3B). Nine cases with more than
four copies of ear-l showed similar tendency for overall survival
(P = 0.0002).
Among the 164 patients who had undergone radical surgery,
lymph node metastasis was positive in 91 cases, and was nega
tive in the other 73. In the latter group, disease-free survival
showed no difference between the nine cases with c-erbB-2
amplification and the other 64 cases without it (P = 0.43) (Fig.
4, Curve A versus B), whereas, in the former group, disease-free
survival was markedly poorer in the 15 cases with c-erbB-2
4
B
6
8 10
Time (years)
survival
oa
uiP1~LP
(%)
Disease-free
,
BI
Ap<0.052
4
4
6
510
Time (years)
4
6
0 10
Time (years)
è 8
10
Time (years)
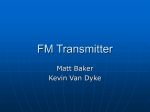
Fig. 2. Survival curves for patient groups with and without Hst-l and/or int-2
amplification. In A, overall survival curves: A, 13 cases with 4-fold or more
amplification of hst-l/int-2; B, nine cases with less than 4-fold amplification of
hst-l/int-2; C, 154 cases with no amplification of these genes. In B, disease-free
survival curves: A, 13 cases with 4-fold or more amplification of hst-l/int-2; B,
nine cases with less than 4-fold amplification of Hst-l/int-2; C, 142 cases with no
amplification of these genes. In B, patients who received palliative surgery were
excluded from the analysis.
the curves for disease-free survival was obviously significant (P
< 0.05, Fig. 2B).
c-erbB-2 and ear-1 Coamplification in Breast Carcinoma. Am
plification of the c-erbB-2 and ear-l genes was observed in 28
cases (16%) and 18 cases (10%), respectively (Table 1). In all
cases with amplification of ear-l, c-erbB-2 was coamplified with
the same copy number, ranging between three- and 16-fold (Fig.
1, Cases A and B). Independent amplification was observed in
10 cases for c-erbB-2, but was not observed for ear-l (Fig. 1,
Case E). The incidences of c-erbB-2 and/or ear-l amplification
Fig. 3. Survival curves for patient groups with and without c-erbB-2 and/or
ear-l amplification. In A, overall survival curves: A, 15 cases with more than 4fold amplification of c-erbB-2/ear-l; B, 13 cases with 4-fold or less amplification
oÕK-erbB-2/ear-l; C, 148 cases with no amplification of these genes. In B, diseasefree survival curves: A, II cases with greater than 4-fold of c-erbB-2/ear-l; B, 13
cases with 4-fold or less amplification of c-erbB-2/ear-l; C, 140 cases with no
amplification of these genes. In B, patients who received palliative surgery were
excluded from the analysis.
3106
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1989 American Association for Cancer Research.
ONCOGENE «(AMPLIFICATION
IN HUMAN BREAST CANCER
Table 4 Proportional hazards general linear models comparing overall and
disease-free survival with prognostic factors in breast carcinoma patients
Factors
Beta
Standard
error
P value
Overallsurvival(N = 1
76)Number
lymphnodesc-<?r*B-2Tumor
of positive
sizeSurgical
therapyhst-l/int-2c-mycAdjuvant
4
chemotherapyMenopausa!
statusear-lDisease-free
6
ÕT 10
Time (years)
Fig. 4. Disease-free survival curves of patient groups with and without lymph
node metastasis. Curves: .I. nine cases with no lymph node metastasis but with
amplificai ion of c-erbB-2; B, 64 cases with no lymph node metastasis or amplifi
cai inn of c-erbB-2; C, 15 cases with both lymph node metastasis and ¡mi
piideation
of c-erbB-2; D, 76 cases with lymph node metastasis but with no amplificai ion of
c-erbB-2.
survival(N=
164)Number
lymphnodesc-erbB-2c-mycTumor
of positive
Table 3 Variables included in proportional hazards general linear model analysis
with their respective scores
sizehst-\/int-2Adjuvant
VariableMenopausa!
chemotherapyear-lMenopausa!
statusTumor
sizeNumber
status0.9981.4970.3750.8490.4760.408-0.122-0.389-0.9920.9111.5771.4850.4340.475-0.06
cm2.
cmaS.l
1-5.0
cm01-3>4beyond
for hst-l/int-2 and c-myc. The postoperative survivals of these
patients were difficult to evaluate due to their small number.
axillarynodesEach
of positive
nodesNoaxillary
ion>3
amplificai
copiesRadical
mastectomyPalliative
mastectomyNot
chemotherapyPre-/perimenopausalPostmenopausal<2.0
doneDoneScores011230123010101
DISCUSSION
c-erbB-2,ear-\,
am piificai ¡onof
c-mycSurgical
hst-l/int-2, or
therapyAdjuvant
amplification than in 76 cases without it (P < 0.01) (Fig. 4,
Curve C versus D). For the curves of overall survival, a similar
correlation was shown (P = 0.94 and P < 0.001, respectively).
Amplification of c-myc Gene in Breast Carcinoma. Amplifi
cation of the c-myc gene was observed in seven cases (4.0%),
the copy number ranging from three to 16. The cases with cmyc amplification were more frequent in older patient group
(P < 0.1). There was a significant difference in overall survival
between the group showing amplification of c-myc (seven cases)
and the rest (169 cases) (P < 0.02), and in disease-free survival
between the former group (six cases) and the latter (158 cases)
Prognostic Value of Amplification of Each Gene as an Inde
pendent Factor. Variables listed in Table 3 were included in the
analysis using a step-wise proportional hazards linear model.
The estimated prognostic value of each variable for overall
survival among the 176 patients, and for disease-free survival
among the 164 patients who had undergone radical surgery is
shown in Table 4. Two variables, i.e., nodal status and ampli
fication of c-erbB-2 were shown to be significant for the predic
tion of overall survival. For prediction of disease-free survival,
three variables, i.e., lymph node status, amplification of c-erbB2 and amplification of c-myc, were found to be significant.
Tumor size showed nearly significant value only in the analysis
for the cases treated by radical surgery. The effects of amplifi
cation of ear-l and hst-l/int-2 and adjuvant chemotherapy were
not significant in both analyses.
Coamplification of Oncogenes Localized on Different Chro
mosomes. Coamplification of genes on different chromosomes
was occasionally observed; four cases for c-erbB-2/ ear-l and
hst-l/int-2, one case for c-erbB-2/ear-l and c-myc, and one case
In the present 176 cases of breast carcinoma, both hst-l and
int-2 were almost always present in a putative amplification
unit in 95% of the cases examined, while both c-erbB-2 and
ear-l were frequently contained in another putative amplifica
tion unit in 67% of cases. The domain containing hst-l and int1 in one of the units seemed to be relatively invariable and to
belong to an essential part of the unit, ear-l appeared to be
peripherally located on the other putative unit, and often drop
ping out from that containing the c-erbB-2 gene.
Amplification of c-erbB-2 was confirmed to be a factor indi
cating a poorer prognosis in breast carcinoma patients, and was
independent of other known prognostic factors such as lymph
node status and tumor size. The copy number was also corre
lated with prognosis. A tendency for early recurrence of carci
noma and early death in patients with c-erbB-2 amplification
was shown only in the group with lymph node metastasis. These
results suggest the importance of examining c-erbB-2 amplifi
cation in cancer tissues of patients with positive lymph node
metastasis. When an increase in the copy number of this gene
is detected in surgically resected cancer tissue from such pa
tients, it would be better to treat them with powerful adjuvant
systemic therapy in order to prolong their survival. Amplifica
tion of ear-l may exert an enhancing action on tumor aggres
siveness either by itself or in cooperation with the c-erbB-2
gene, as in the case of their viral counterparts \-erb\ and verbB in avian erythroblastosis virus, where the former enhances
the action of the latter (13).
Although amplification of the unit containing hst-l and int2, the ear-l gene and the c-myc gene were correlated with the
prognosis in the univariate analysis, the independent impor
tance of them as a prognostic factor was lower than that of cerbB-2 amplification. Amplification of hst-l and/or int-2 was
preferentially detected in the younger patient age group and
thus may have some association with the hormonal status of
the patient.
The incidence of amplification of c-myc and c-erbB-2 in this
3107
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1989 American Association for Cancer Research.
ONCOGENE COAMPLIFICATION
study differed to various extents compared with previous re
ports (15, 27). In particular, amplification of c-myc was rare in
this study. A difference of race may be one of the possible
reasons for this variable incidence. Another possible cause was
the criteria employed for determination of gene amplification.
In this study, we did not count a copy number of 2 as amplifi
cation because of the difficulty involved in its reproducible
evaluation. In the majority of cases showing amplification of cmyc, its copy number may be less than 3. Underestimation of
the copy number of a gene might occur because of contaminat
ing stromal cells and lymphocytes (15), or tumor cell hetero
geneity in studies of human tumor tissues. Therefore, it is
always necessary to confirm that cancer cells are dominant in
the sampled tissue before evaluating the copy number of a
specific DNA by histológica! examination.
ACKNOWLEDGMENTS
The authors are grateful to Dr. C. Dickson (Imperial Cancer Re
search Fund Laboratories, London, UK) for the DNA probe SS6
(human int-2, Sad fragment), to Dr. T. Glaser (Massachusetts Institute
of Technology, Cambridge, MA) for the DNA probe pE4b-TGH2
(D11S24), and to Dr. R. White (University of Utah Medical Center,
Salt Lake City, UT) for the DNA probe pHF12-2 (D17S1). The c-mos
gene was obtained from the American Type Culture Collection, Rockville, MD. We are also grateful to H. Yoshida for her excellent technical
work.
REFERENCES
1. Kinzler, K. W., Zehnbauer, B. A., Brodeur, G. M., Seeger, R. C., Trent, J.
M., Meltzer, P. S., and Vogelstein, B. Amplification units containing human
N-myc and c-myc genes. Proc. Nati. Acad. Sci. USA, 83: 1031-1035, 1986.
2. Tsutsumi, M.. Sakamoto, H., Yoshida, T., Kakizoe, T., Koiso, K.. Sugimura,
T., and Terada, M. Coamplification of the hst-1 and int-2 gene in human
cancers. Gann, 79: 428-432, 1988.
3. Yoshida, M. C., Wada, M., Satoh, H., Yoshida, T., Sakamoto, H., Miyagawa,
K., Yokota, J., Koda, T., Kakimmm. M., Sugimura, T., and Terada, M.
Human HST1 (IISII I) gene maps to chromosome band 1Iql3 and coamplifies with the INT2 gene in human cancer. Proc. Nati. Acad. Sci. USA, 85:
4861-4864, 1988.
4. van de Vijver, M., van de Bersselaar, R., Deville, P., Cornelisse, C., Peterse,
J., and Nusse, R. Amplification of the neu (c-erbB-2) oncogene in human
mammary tumors is relatively frequent and is often accompanied by ampli
fication of the linked c-erbA oncogene. Mol. Cell Biol., 7: 2019-2023, 1987.
5. Yokota, J., Vaniamolo. T., Miyajima, N., Toyoshima, K., Nomura, N.,
Sakamoto, H., Yoshida, T., Terada, M., and Sugimura, T. Genetic alterations
of the c-erbB-2 oncogene occur frequently in tubular adenocarcinoma of the
stomach and are often accompanied by amplification of the \-erb\ homo
logue. Oncogene, 2: 283-287, 1988.
6. Sakamoto, H., Mori, M., Taira, M., Yoshida, T., Matsukawa, S., Shimizu,
K., Sekiguchi, M., Terada, M., and Sugimura, T. Transforming gene from
human stomach cancers and a noncancerous portion of stomach mucosa.
Proc. Nati. Acad. Sci. USA, 83: 3997-4001, 1986.
7. Casey, G., Smith, R., McGillivray, D., Peters, G., and Dickson, C. Charac
terization and chromosome assignment of human homolog of int-2, a poten
IN HUMAN BREAST CANCER
tial proto-oncogene. Mol. Cell Biol., 6: 502-510, 1986.
8. Moore, R., Casey, G., Brookes, S., Dixon, M., Peters, G., and Dickson, C.
Sequence, topography and protein coding potential of mouse int-2: a putative
oncogene activated by mouse mammary tumor virus. EMBO J., 5:919-924,
1986.
9. Yoshida, T., Miyagawa, K., Odagiri, H., Sakamoto, H., Little, P. F. R.,
Terada, M., and Sugimura, T. Genomic sequence of AJÕ,
a transforming gene
encoding a protein homologous to fibroblast growth factors and the int-2encoded protein. Proc. Nati. Acad. Sci. USA, 84: 7305-7309, 1987.
10. Fukushige, S., Matsubara, K., Yoshida, M., Sasaki, M., Suzuki, T., Semba,
K., Toyoshima, K., and Yamamoto, T. Localization of a novel v-Ã-réB-related
gene, c-erbB-2, on human chromosome 17 and its amplification in a gastric
cancer cell line. Mol. Cell Biol., 6:955-958, 1986.
11. Yamamoto, T., Ikawa, S., Akiyama, T., Semba, K., Nomura, N., Miyajima,
N., Saito, T., and Toyoshima, K. Similarity of protein encoded by the human
c-erb-B-2 gene to epidermal growth factor receptor. Nature (Lond.), 319:
230-234, 1986.
12. Weinberger, C., Thompson, C. C., Ong, E. S., Lebo, R., Gruol, D. J., and
Evans, R. M. The c-erb-A gene encodes a thyroid hormone receptor. Nature
(Lond.), 324:641-646, 1986.
13. Green, S., Walter, P., Kumar, V., Krust, A., Bornert, J-M., Argos, P., and
Chambón, P. Human oestrogen receptor cDNA: sequence, expression and
homology to v-erb-A. Nature (Lond.), 320: 134-139, 1986.
14. Ali, I. U., Campbell, G., Lidereau, R., Callahan, R., Slamon, D. J., and
Clark, G. M. Amplification of c-ereB-2 and aggressive human breast tumors?
Science (Wash. DC), 240:1795-1798, 1988.
15. Slamon, D. J., Clark, G. M., Wong, S. G., Levin, W. J., Ullrich, A., and
McGuire, W. L. Human breast cancer: correlation of relapse and survival
with amplification of the HER-2/neu oncogene. Science (Wash. DC), 235:
177-182, 1987.
16. Bealirs. O. H., and Myers, M. H. Manual for Staging of Cancer, Ed. 2, pp.
127-133. Philadelphia: J. B. Lippincott Company, 1983.
17. Tsuda, H., Shimosato, Y., Upton, M. P., Yokota, J., Terada, M., Ohira. M.,
Sugimura, T., and Hirohashi, S. Retrospective study on amplification of Nmir and c-myc genes in pediatrie solid tumors and its association with
prognosis and tumor differentiation. Lab. Invest., 59:321-327, 1988.
18. Taira, M., Yoshida, T., Miyagawa, K., Sakamoto, H., Terada, M., and
Sugimura, T. cDNA sequence of human transforming gene hst and identifi
cation of the coding sequence required for transforming activity. Proc. Nati.
Acad. Sci. USA, 84: 2980-2984, 1987.
19. Alitalo, K., Schwab, M., Lin, C. C., Varmus, H. E., and Bishop, J. M.
Homogeneously staining chromosomal regions contain amplified copies of
an abundantly expressed cellular oncogene (c-myc) in malignant neuroendocrine cells from a human colon carcinoma. Proc. Nati. Acad. Sci. USA, 80:
1707-1711,1983.
20. Glaser, T., Gerhard, D., Payne, C., Jones, C., and Housman, D. Three
polymorphic DNA markers from chromosome 11. Cytogenet. Cell Genet.,
40:643,1985.
21. Barker, D., and White, R. More base pair change polymorphisms at sites
containing CpG. Cytogenet. Cell Genet., 32: 253, 1983.
22. Watson, R., Oskarsson, M., and Vande Woude, G. F. Human DNA sequence
homologous to the transforming gene (mos) of Moloney murine sarcoma
virus. Proc. Nati. Acad. Sci. USA, 79:4078-4082, 1982.
23. Kaplan, E. L., and Meier, P. Nonparametric estimation from incomplete
observations. J. Am. Stat. Assoc., 53:457-481, 1958.
24. Peto, R., Pike, M. C., Armitage, P., Breslow, N. E., Cox, D. R., Howard, S.
V., Mantel, N., McPherson, K., Peto, J., and Smith, P. G. Design and
analysis of randomized clinical trials requiring prolonged observation of each
patient II. Analysis and examples. Br. J. Cancer, 35: 1-39, 1977.
25. Cox, D. R. Regression models and life-tables. J. R. Stat. Soc., 34: 187-220,
1972.
26. Harrell, F. E., Jr. The PHGLM procedure. In: R. P. Hastings, (ed.), Supple
mentary Library User's Guide, pp. 267-294. Cary, SAS Institute Inc., 1983.
27. Escot, C., Theillet, C., Lidereau, R., Spyratos, F., Chámpeme, M-E., Gest,
J., and Callahan, R. Genetic alteration of the c-myc protooncogene (MY(')
in human primary breast carcinomas. Proc. Nati. Acad. Sci. USA, 83:48344838, 1986.
3108
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1989 American Association for Cancer Research.
Correlation between Long-Term Survival in Breast Cancer
Patients and Amplification of Two Putative
Oncogene-Coamplification Units: hst-1/int-2 and c-erbB-2/ear-1
Hitoshi Tsuda, Setsuo Hirohashi, Yukio Shimosato, et al.
Cancer Res 1989;49:3104-3108.
Updated version
E-mail alerts
Reprints and
Subscriptions
Permissions
Access the most recent version of this article at:
http://cancerres.aacrjournals.org/content/49/11/3104
Sign up to receive free email-alerts related to this article or journal.
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Department at [email protected].
To request permission to re-use all or part of this article, contact the AACR Publications
Department at [email protected].
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1989 American Association for Cancer Research.