Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
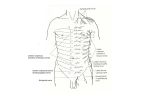
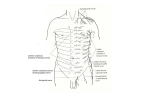
THORACIC WALL Dr. Milton M. Sholley SELFSTUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 5069 Syllabus: 8 pages (Page 8 lists corresponding figures for Grant's Atlas 11 th & 12 th Eds.) Head to Toe Questions in Gross Anatomy: Start questions #216253 Structures: Thoracic vertebrae (T1 T12) Ribs (12 pairs) Sternum (3 parts: manubrium, body, and xiphoid process) Joints: costovertebral, costotransverse, sternocostal, costochondral, manubriosternal, and xiphisternal Costal arch Endothoracic fascia Intercostal muscles (external, internal, innermost) Diaphragm (superior surface) Intercostal nerves Blood supply: Internal thoracic (mammary) arteries These give rise to the Musculophrenic and Superior epigastric arteries Posterior intercostal arteries Anterior intercostal arteries Veins with similar names accompany the above arteries Note: You will need to visualize the outline of internal structures (heart & pericardium, lungs and pleura) on the chest wall after you have seen them (Grant's Atlas: 11 th Ed. Figs. 1.39, 1.40, 1.26A1.26D; 12 th Ed. Figs. 1.39, 1.40, 1.26A1.26D). LECTURE OUTLINE I. General remarks: The thoracic skeleton is shaped like a flattened, truncated cone and encloses the thoracic cavity. The thoracic cavity contains two pleural sacs that cover the two lungs, and between the two pleural sacs is a pericardial sac that covers the heart. There is a space between the two pleural sacs known as the mediastinum, in which are located the pericardial sac and heart, the great vessels, the trachea, and the esophagus. The thoracic skeleton is composed of a sternum anteriorly, 12 thoracic vertebrae posteriorly, and 10 pairs of ribs connecting the vertebrae to the sternum via costal cartilages. Two lower pairs of ribs, which are short, connect with thoracic vertebrae only. These lower ribs together with the costal margins of the inferior ribs and the inferior part of the sternum form the inferior thoracic aperture, which is closed by the abdominal diaphragm. The superior thoracic aperture is a relatively small opening formed by the first pair of ribs, the body of the first thoracic vertebra and the manubrium. Through the superior thoracic aperature, the trachea and esophagus pass from the neck into the thorax and vessels and nerves connect with the neck and the upper limb. II. Thoracic skeleton (Grant's Atlas: 11 th Ed. Figs. 1.9 A&B; 12 th Ed. Figs. 1.9 A&B) A. The sternum is composed of three palpable parts: the manubrium, the body of the sternum, and the xiphoid process (Grant's Atlas: 11 th Ed. Fig. 1.10; 12 th Ed. Fig. 1.10). The superior margin of the manubrium forms the jugular notch, which lies at the level of the 3rd thoracic vertebra on a line projected posteriorly. The manubrium articulates with the upper end body of the sternum (manubriosternal joint) and the xiphoid process articulates with the lower end of the body of the sternum (xiphisternal joint). The manubriosternal and xiphisternal joints may fuse in older individuals. B. The first 7 pairs of ribs connect with the sternum directly via their costal cartilages and are called true ribs (Grant's Atlas: 11 th Ed. Figs. 1.9 A&B; 12 th Ed. Figs. 1.9 A&B). The next 3 pairs of ribs connect with the seventh rib via their costal cartilages and are called false ribs. The 11th and 12th pairs do not connect with the sternum and are called floating ribs. The costal arch is made up of costal cartilages 7 to 10 on both sides. C. How do we count ribs and intercostal spaces in the intact body? The cartilages of the second ribs connect to the sternum at the level of the manubriosternal joint, which has a raised surface which can be easily palpated and is called the sternal angle or Angle of Louis. Below the second rib lies the second intercostal space. Successive ribs have correspondingly numbered intercostal spaces. The apex beat of the heart can be palpated in the fifth intercostal space on the midclavicular line (about 3.5 inches from the midline). The first rib lies under cover of the clavicle and its attached muscles and cannot be palpated. All the other ribs are palpable, some more easily than others. D. Most ribs articulate with the vertebral column at both of two joints (See Figures 4 and 5 of this syllabus and Grant's Atlas: 11 th Ed. Fig. 1.12; 12 th Ed. Fig. 1.12). These two joints are the costovertebral joint, between the head of the rib and the vertebral bodies, and the costotransverse joint, between the tubercle and the transverse process of the rib. The bony shaft of each rib is directly united to its cartilage (costochondral synchondrosis or costochondral joint). The costal cartilages of the upper seven ribs articulate with the sternum directly (sternocostal joint). The costal cartilages of ribs 8, 9 and 10 form interchondral joints. III. Muscles of the thoracic wall (Grant's Atlas: 11 th Ed. Figs.1.161.20; 12 th Ed. Figs.1.16 1.20) A. There are 11 intercostal spaces and each contains an external, an internal, and an innermost intercostal muscle layer (Grant's Atlas: 11 th Ed. Fig. 1.18; 12 th Ed. Fig. 1.18). All three are thin sheets of muscle whose fibers run from one rib to the next. The external intercostal muscle closes the intercostal space posteriorly and laterally, but not anteriorly, where it is continued as the external intercostal membrane, through which the internal intercostal muscle can be seen. The internal intercostal muscle closes the intercostal space anteriorly and laterally and posteriorly it is continued as an internal intercostal membrane. The innermost intercostal muscle lies in the intercostal space posteriorly and laterally and both its anterior and posterior ends are continued as membranes. Intercostal Space Transverse CT Plane Internal thoracic a. Ant. intercostal a. Transversus thoracis m. External intercostal m. Thoracic aorta Internal intercostal m. Innermost intercostal m. Right Intercostal n. Nerves are shown on the right side. Arteries are shown on the left side. Post. intercostal a. Dorsal Left Reoriented from: Grant’s Atlas, 12 th Ed., Fig. 1.18, p. 20 Please study Grant's Atlas Figure 1.18 (12 th Ed.). This diagram is that drawing flipped vertically to simulate the orientation that is routinely used to study CT and MRI images. B. The subcostal muscles are placed posteriorly and span two to three intercostal spaces. In many bodies these are poorly developed and inconspicuous. C. The transversus thoracis (Grant's Atlas: 11 th Ed. Fig. 1.20; 12 th Ed. Fig. 1.20) is a thin layer of muscle in the thoracic cavity whose fibers fan out from the posterior surface of the lower part of the sternum to the neighboring costal cartilages. It is part of the same layer as the innermost intercostal muscle. IV. V. D. The diaphragm (Grant's Atlas: 11 th Ed. Fig. 1.20; 12 th Ed. Fig. 1.20) is a curved musculotendinous sheet intervening between the thoracic and abdominal cavities and closes the inferior thoracic aperture. E. The diaphragm and intercostal muscles bring about respiratory movements necessary for breathing. Fascias of the thoracic wall A. The external fascias have already been seen, including the superficial fascia enclosing the breast tissue and the deep fascia enclosing the pectoralis major and minor muscles (Grant's Atlas: 11 th Ed. Fig. 1.4B; 12 th Ed. Fig. 1.4B). Posteriorly the deep fascia thickens to become the thoracolumbar fascia covering the erector spinae muscle (Grant's Atlas: 11 th Ed. Fig. 4.29; 12 th Ed. Fig. 4.32). B. The endothoracic fascia, consisting of loose connective tissue, covers the internal surface of the rib cage and superior surface of the diaphragm. It becomes thickened over the superior thoracic aperture and fuses with the apical or cervical pleura. Do not try to find this as a separate layer in the laboratory. Nerves of the thoracic wall Anterior surface 5a “Typical” Spinal Nerve (T2 T11) and its branches in relation to body surfaces Intercostal 1. Dorsal root Vein 5b 2. Ventral root Artery RIB 2 3. Spinal nerve Nerve 5 4. Dorsal ramus 4a. Medial branch 4b. Lateral branch 5. Ventral ramus 5a. Anterior branch 5b. Lateral branch Gray ramus communicans 3 1 4a 4 Innermost intercostal muscle 4b Posterior surface A. Sympathetic trunk White ramus communicans Grant’s Atlas, 12 th Ed., Fig. 1.15, p. 17 Anteriorly and laterally, the thoracic wall is innervated by ventral rami of T1 to T12 spinal nerves. The T1 ventral ramus also gives a major contribution to the brachial plexus, and thus T1 is not a “typical spinal nerve”. T1 T11 ventral rami form intercostal nerves, but T12 is subcostal in position and is called the subcostal nerve. All are sensory to overlying skin and underlying parietal pleura and motor to intercostal muscles. Intercostal nerves T1 to T6 are confined to the thoracic wall, but T7 to T12 extend to the abdomen where they are motor to abdominal muscles (Grant's Atlas: 11 th Ed. Figs. 2.2 & 2.5; 12 th Ed. Figs. 2.3 & 2.5). Superior to the sternal angle, the skin is innervated by supraclavicular nerves C3 and C4 (Grant's Atlas: 11 th Ed. Fig. 8.1; 12 th Ed. Fig. 8.1). VI. B. All the ventral rami have lateral and anterior cutaneous branches to the skin (Grant's Atlas: 11 th Ed. Fig. 1.18; 12 th Ed. Fig. 1.18). Lateral branches of T2 and T3 form intercostobrachial nerves to the skin of the arm (Grant's Atlas: 11 th Ed. Fig. 6.20A; 12 th Ed. Fig. 6.20A) and the lateral cutaneous branch of T12 reaches the lateral area of the groin and buttocks (Grant's Atlas: 11 th Ed. Fig. 2.2A; 12 th Ed. Fig. 2.3A). C. Posteriorly, over the paravertebral musculature of the back, the dorsal rami of T1 to T12 innervate skin and the deep back muscles (Grant's Atlas: 11 th Ed. Figs. 4.28 & 4.30; 12 th Ed. Figs. 4.31 & 4.33). Blood supply of the thoracic wall A. Two internal thoracic arteries arise from the right and left subclavian arteries and descend vertically, posterior to the costal cartilages, on either side of the sternum (Grants Atlas: 11 th Ed. Fig. 1.20; 12 th Ed. Fig. 1.20). Behind the 6th costal cartilage each internal thoracic artery divides into its two terminal branches, the musculophrenic and superior epigastric arteries. The superior epigastric artery anastomoses with the inferior epigastric artery on the posterior surface of the rectus abdominis muscle of the abdomen (Grant's Atlas: 11 th Ed. Fig. 2.5; 12 th Ed. Fig. 2.5). The anterior intercostal arteries arise from the internal thoracic artery (Grant's Atlas: 11 th Ed. Fig. 1.18; 12 th Ed. Fig. 1.18), on each side, and lie in a horizontal position in the upper five intercostal spaces along the lower border of each rib. In the lower five spaces, similar branches arise from the musculophrenic artery. The internal thoracic artery also gives off perforating branches to the skin and breast in the 2nd, 3rd and 4th intercostal spaces and these vessels enlarge during lactation. Other small branches of the internal thoracic artery go to the mediastinum, thymus, pericardium (pericardiophrenic artery Grant's Atlas: 11 th Ed. Fig. 1.75; 12 th Ed. Fig. 1.76) and sternum. B. The descending thoracic aorta, which lies on the left side of the vertebral column, gives off posterior intercostal arteries to intercostal spaces (Grant's Atlas: 11 th Ed. Fig. 1.70C; 12 th Ed. Fig. 1.72C), except the first two intercostal spaces which receive blood from the supreme intercostal artery given off by the costocervical branch of the subclavian artery. The posterior intercostal arteries of the upper six spaces terminate by anastomosing with the corresponding anterior intercostal arteries (Grant's Atlas: 11 th Ed. Fig. 1.18; 12 th Ed. Fig. 1.18). Those of the lower spaces, like the corresponding nerves, continue to the abdominal wall. C. VII. Veins accompany the above arteries and their branches and have similar names. The intercostal veins anastomose in the same manner as the arteries. Most posterior intercostal veins on the right terminate in the azygos vein, while most of those on the left terminate in the hemiazygous or accessory hemiazygous veins. The azygous vein lies on the right and the hemiazygous and accessory hemiazygous veins lie on the left along the bodies of the vertebra (Grant's Atlas: 11 th Ed. Figs. 1.73 & 1.74; 12 th Ed. Figs. 1.75 & 1.76). The veins of the first intercostal spaces are called supreme intercostal veins and drain into the brachiocephalic veins (Grant's Atlas: 11 th Ed. Fig. 1.74; 12 th Ed. Fig. 1.76); and the veins of the second through fourth intercostal spaces form superior intercostal veins, which in turn drain into the azygous arch on the right and the brachiocephalic vein on the left. The internal thoracic veins, which receive the anterior intercostal veins, also drain into the brachiocephalic veins. Lymphatic drainage A. The lymph nodes of the thorax are parietal and visceral nodes (the visceral nodes will be considered later). The parietal nodes are sternal, phrenic (diaphragmatic), and intercostal. B. The sternal (also called parasternal or internal thoracic) nodes (Grant's Atlas: 11 th Ed. Fig. 1.8; 12 th Ed. Fig. 1.8) are present along the upper part of the internal thoracic artery, one or two in each of the upper four or five intercostal spaces. They receive lymphatic vessels from the medial part of the breast, the diaphragm, intercostal spaces and the costal pleura. Their efferent vessels join the bronchomediastinal trunk (more about this later). These important nodes provide a route by which cancer of the breast can spread to the lungs, mediastinum and liver. The parasternal nodes are sometimes invaded by metastasis from carcinoma of the breast at the same time as or before the axillary nodes. C. The phrenic nodes occur in several groups on the thoracic surface of the diaphragm, posterior part of the diaphragm and near the left phrenic nerve and inferior vena cava. They are interconnected by lymphatic channels. They receive lymphatic vessels from the diaphragm, liver, stomach and esophagus, and from the lower intercostal spaces and pericardium. They send their efferent vessels to either the anteriorly located parasternal nodes or to posterior mediastinal nodes. D. The intercostal nodes are located at the vertebral end of each intercostal space. They receive lymphatic vessels from structures along the adjacent blood vessels and parietal pleura. The nodes in the upper intercostal spaces drain into the thoracic duct (Grant's Atlas: 11 th Ed. Fig. 1.74; 12 th Ed. Fig. 1.75). Those in the lower spaces generally drain into a vessel on each side that descends to the cisterna chyli in the abdomen. VIII. Respiratory movements (ECA, Fig 2.6, p. 59) A. CVJ The thoracic cavity expands in three directions (vertically, anteroposteriorly, and laterally) to bring about inspiration. The vertical expansion is caused by the contraction (and therefore lowering) of the diaphragm; the anteroposterior expansion (“pumphandle action”) is caused by the intercostal muscles raising the curved ribs, and the lateral expansion (“buckethandle action”) is also caused by the intercostal muscles raising the curved ribs. Quiet expiration is caused by elastic recoil of the lungs and rib cartilages. Costovertebral joints (CVJ) The head of a typical rib has two articular surfaces and forms costovertebral joints with the vertebral body of its own number and another CVJ with the vertebra above. T6 CVJ T7 Costotransverse joint (CTJ) The tubercle of a typical rib forms a costotransverse joint with the transverse process of the vertebra of the same number. CTJ The CTJs of ribs 17 rotate, causing the “pump handle” movement of the ribs, which increases the anteriorposterior dimension of the thorax. The CTJs of ribs 810 glide, causing the “buckethandle” movement of the ribs, which increases the transverse dimension of the thorax. 7th rib Posterolateral view B. Grant’s Atlas, 12 th Ed., Fig. 1.12B, p. 14 Grant’s Atlas, 12 th Ed., Fig. 1.12C, p. 14 During vigorous breathing other muscles become involved. In forced expiration the abdominal muscles, including the internal and external obliques and transversus, contract, thereby compressing the abdominal organs and forcing the passive diaphragm upward The scalene and sternocleidomastoid muscles in the neck aid in vigorous inspiration by pulling upward on the first rib and sternum, respectively. Other muscles that attach to the thoracic walls also may become involved when the subject’s arm is fixed by gripping a stationary object. Figures from Grant's Atlas of Anatomy (11 th Ed.) 1.39, page 44 and 1.40, page 45 1.26A,B,C,D, pages 3031 1.9A, page 10 1.9B, page 11 1.10A,B,&C, page12 1.12B, page 14 1.18, page 20 1.19, page 22 1.20, page 23 1.15, page 17 1.42, page 48 1.64B, page 68 1.71, page 74 1.73, page 76 1.74, page 77 Figures from Grant's Atlas of Anatomy (12 th Ed.) 1.39, page 44 and 1.40, page 45 1.26A,B,C,D, pages 3031 1.9A, page 10 1.9B, page 11 1.10A,B,&C, page12 1.12B, page 14 1.18, page 20 1.19, page 22 1.20, page 23 1.15, page 17 1.42, page 48 1.66B, page 70 1.73, page 76 1.75, page 78 1.75, page 79