Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
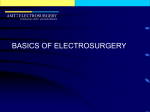
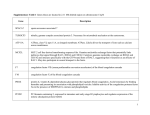
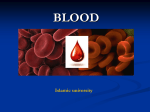
868 Theme Issue Article Coagulation proteases and CVD In vivo activation and functions of the protease factor XII Jenny Björkqvist1,2; Katrin F. Nickel1,2,3; Evi Stavrou4; Thomas Renné1,2,3 1Department of Molecular Medicine and Surgery, Karolinska Institutet, Stockholm, Sweden; 2Center of Molecular Medicine, Karolinska Institutet, Stockholm, Sweden; 3Institute of Clinical Chemistry and Laboratory Medicine, University Medical Center Hamburg, Hamburg, Germany; 4Department of Medicine, Hematology and Oncology Division, Case Western Reserve University; Louis Stokes Veterans Administration Hospital; University Hospital Case Medical Center, Cleveland, Ohio, USA Summary Combinations of proinflammatory and procoagulant reactions are the unifying principle for a variety of disorders affecting the cardiovascular system. Factor XII (FXII, Hageman factor) is a plasma protease that initiates the contact system. The biochemistry of the contact system in vitro is well understood; however, its in vivo functions are just beginning to emerge. The current review concentrates on activators and Correspondence to: Thomas Renné, MD, PhD Institute for Clinical Chemistry and Laboratory Medicine University Medical Center Hamburg D-20246 Hamburg, Germany Tel.: +49 40 7410 58984, Fax: +49 40 7410 57576 and Clinical Chemistry, Department of Molecular Medicine and Surgery Karolinska Institutet Karolinska University Hospital Solna (L1:00) SE-171 76 Stockholm, Sweden Tel.: +46 8 517 73390, Fax: +46 310376 E-mail: [email protected] Biochemistry of factor XII The contact system is a plasma-borne protease cascade that exerts procoagulant and proinflammatory activities. The system comprises the serine proteases factor XII (FXII), plasma prekallikrein (PPK), and factor XI (FXI), the non-enzymatic cofactor high-molecular-weight kininogen (HK) and C1 esterase inhibitor (C1INH). C1INH is the major inhibitor of activated FXII (FXIIa) and plasma kallikrein (PK), respectively (1–3). FXII is the principal initiator of the contact system reaction cascades (▶ Figure 1). Binding to negatively charged surfaces induces a conformational change in zymogen FXII, leading to the generation of small amounts of FXIIa. FXIIa cleaves PPK to generate active PK, which in turn reciprocally activates FXII. This amplification loop generates sufficient PK activity to liberate BK from HK by limited proteolysis (kallikrein-kinin system) (4). FXIIa also initiates other cascades such as the intrinsic pathway of coagulation via its substrate FXI. Furthermore, FXIIa has the capacity to drive the classic complement system pathway via activation of C1r and to a lesser degree the C1s subunit of C1, and the fibrinolytic system by PK-mediated urokinase or plasminogen activation or indirectly via BKtriggered tissue plasminogen activator (tPA) release (4, 5). FXII is primarily produced in the liver although some expression has been observed in other cells including endometrial stromal cells or leukocytes (6). FXII has an apparent molecular functions of the FXII-driven contact system in vivo. Elucidating its physiologic activities offers the exciting opportunity to develop strategies for the safe interference with both thrombotic and inflammatory diseases. Keywords Coagulation factors, contact phase, proteases Received: April 3, 2014 Accepted after minor revision: July 7, 2014 Epub ahead of print: September 4, 2014 http://dx.doi.org/10.1160/TH14-04-0311 Thromb Haemost 2014; 112: 868–875 weight of 80 kDa and circulates in plasma as a single chain zymogen with a concentration of 30–35 µg/ml (0.37 µM) with a halflife of 50 to 70 hours (7). The FXII gene is composed of 13 introns and 14 exons (8) that codes for a zymogen consisting of 596 amino acids. FXII is composed of a N-terminal fibronectin domain type II (Fib II, encoded by exon 3 and 4), an epidermal-growth-factorlike domain (EGF I, exon 5), a fibronectin domain type I (Fib I, exon 6), a second epidermal-growth-factor-like domain (EGF II, exon 7), a kringle domain (exon 8 and 9), a proline-rich region (a 55 amino acid long region, exon 9) and the catalytic domain (exon 10–14, ▶ Figure 2). The FXIIa form consists of a disulfide-linked heavy chain (Mw of 52 kDa) and a light chain (Mw of 28 kDa). The latter one mediates the enzymatic activity, whereas FXII binds to negatively charged surfaces via its heavy chain. The FXII surface-binding site is not precisely known and several regions appear to contribute including the distal N-terminal end (residues 1–28), the Fib II, the Fib I, the EGF II, the kringle domain and possibly the proline-rich region (7). FXII zymogen is activated by limited proteolysis involving cleavage of the peptide bond Arg353-Val354 resulting in a two-chain molecule, FXIIa (α-FXIIa). Two principal modes of FXII activation exist. The zymogen is activated through binding to negatively charged surfaces that induces a conformational change (auto-activation) (9, 10). Zinc ions (Zn2+) bind to FXIIa intermediate states and increase susceptibility for auto-activation by stabilising conformations in the Thrombosis and Haemostasis 112.5/2014 © Schattauer 2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. Figure 1: FXII-driven signalling cascades. FXII directly activates the intrinsic pathway of coagulation, the complement system and kallikrein-kinin system; FXII indirectly activates fibrinolysis via PK and BK. C1INH is the major inhibitor of FXIIa and PK. activation reaction. Cleavage of FXII is also mediated by other proteases such as PK (hetero-activation). FXIIa consists of a heavy chain and a light chain, connected by a single disulfide-bond between two Cysteine residues (Cys340-Cys367). Further cleavage of α-FXIIa at positions 334 and 343 results in β-FXIIa (Hageman factor fragment, HFf). Although retaining its proteolytic activity towards PPK, β-FXIIa is unable to bind to negatively charged surfaces and therefore has no effect on FXI activation and thrombosis. C1INH is the principle endogenous inhibitor of FXIIa and PK with > 90 % of FXIIa and > 50 % of PK, respectively, inhibited in plasma of healthy individuals (11). Other inhibitors of the contact system proteases include α1-antitrypsin, α2-antiplasmin, α2-macroglobulin and antithrombin (6, 12–14). FXII in coagulation Figure 2: Domain structure of FXII forms. The heavy chain, which harbours the putative surface-binding region of FXII, consists of the five domains Fib II, EGF I, Fib I, EGF II, kringle domain and the proline-rich region. The light chain bears the enzymatic site of the serine protease. The two chains are connected by a single disulfide-bond (Cys340 and Cys367). Cleavage of the peptide bond Arg353-Val354 (arrow 1) results in two-chain activated FXII (α-FXIIa). The catalytic triad of FXIIa consists of His393, Asp442 and Ser544. Further proteolysis of the peptide bonds Arg343-Leu344 and Arg334-Asn335 (arrows 2 and 3) by PK, results in activated FXII-fragment (β-FXIIa). Congenital deficiency in FXII (Hageman trait) is an autosomal recessive trait, initially described in 1955 in the index patient Mr. John Hageman (15). Similarly to other contact system proteins (PPK and HK), deficiency in FXII severely prolongs the activated partial thromboplastin time (aPTT), a diagnostic coagulation assay that relies on contact system activation. However, in sharp contrast to deficiency in tissue factor, factors VII, VIII (Haemophilia A) or IX (Haemophilia B), individuals with severe deficiencies in the contact FXII, PPK or HK do not suffer from spontaneous or injury-related excessive bleeding (1). PPK-, HK-, and FXII-deficient patients safely undergo surgical procedures without blood product support and have a completely normal haemostatic capac- © Schattauer 2014 Thrombosis and Haemostasis 112.5/2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. 869 Coagulation proteases and CVD Björkqvist et al. Factor XII Coagulation proteases and CVD 870 Björkqvist et al. Factor XII ity. FXI deficiency predisposes individuals to stress-related bleeding such as that seen with trauma or surgical procedures that involve tissues with high fibrinolytic activity (oropharyngeal, genitourinary). However, independent laboratories have shown that the antigen level of plasma FXI does not correlate with increased bleeding risk suggesting a more complex role of FXI in regulating haemostasis (7). The intact haemostasis in contact systemdeficient individuals led to the premise that this pathway is dispensable during bleeding and that fibrin formation at sites of injury is exclusively dependent on the extrinsic pathway. However, previous data have challenged this concept. We generated the first FXII-deficient mice (16) and reported that they are protected from thrombosis both in venous and arterial beds in various experimental models (17). Subsequent studies have shown that FXIIdeficient mice are also protected from cerebral ischaemia in an experimental stroke model of transient (18) but not permanent (19) occlusion of the middle cerebral artery (MCAO model). Defects in the FXII-driven intrinsic coagulation pathway also provide thromboprotection in rabbits and baboon models (20). Despite evidence that FXII deficient/inhibited animals are largely protected from vessel occlusive thrombosis, the contribution of FXII in human thrombotic disease remains to be analysed. There are anecdotal reports suggesting that FXII deficiency may actually predispose to thrombosis, dating back to the death of the index FXII deficient patient who succumbed to an episode of post-operative pulmonary embolism. However, larger studies have convincingly shown that thrombosis in FXII-deficient patients is related to other risk factors, independent of the noted FXII deficiency (21, 22). FXII is highly preserved among mice and humans and the FXII homologs share 71 % identity on the protein level. There is experimental evidence that FXIIa triggers similar pathways among the species. Infusion of human FXII into FXII-/- mice restores their prolonged aPTT (17) and homologous human proteins restore defective thrombus formation in FXII-/-, FXI-/- and PK-/- mice (17, 23, 24), further corroborating the close similarity of the contact system among species. Furthermore, deficiency in the major substrate of activated FXII, FXI, largely reduces the risk of ischaemic stroke (25) and venous thrombosis (26) in human subjects. Vice versa elevated FXI levels are associated with increased risk of myocardial infarction in men (27). Basal BK levels are depressed in FXII-deficient mice and deficiency in the contact system proteins might be beneficial in human inflammatory disease states (28). Multiple mutations are known to cause loss of FXII activity and deficiency in the clotting factor. Some mutations either reduce FXII plasma levels by interference with synthesis or secretion. Other mutations interfere with the enzymatic activity of FXIIa. These latter mutations are either located in the serine protease catalytic triad His393-Asp442–Ser544 or in close proximity to these residues (29). FXII (Washington DC) has a Cys571-to-Ser571 substitution that leads to complete loss of procoagulant activity in vitro (30). Another example is FXII Locarno, which is a secreted but dysfunctional protein due to an Arg353 substitution. The mutation alters the FXIIa/PK recognition site in FXII and abolished zymogen activation by limited proteolysis (31). FXII in hereditary angioedema Hereditary angioedema [HAE (MIM #106100)] is a rare lifethreatening inherited oedema disorder that is characterised by recurrent episodes of acute swelling, involving the skin, oropharyngeal, laryngeal, or gastrointestinal mucosa (32). The mechanisms of increased vascular permeability in HAE and excessive formation of the proinflammatory peptide hormone BK is a consistent finding in acute episodes in HAE patients (33). HAE develops in individuals who are quantitatively or qualitatively deficient in C1INH (HAE type I and II, respectively) (32). Ablation of Serping1 gene expression (that codes for C1INH) results in excessive BK production and increased vascular permeability in mice (34) and humans (35). In addition to these two classical HAE types, a third variant exists that mostly affects women, HAE type III (HAEIII). HAEIII patients have normal levels of fully functional C1INH but suffer from angioedema nonetheless (36). Using genome-wide linkage analyses, HAEIII was shown to be associated with a single missense mutation (c.1032CrA) in the F12 gene (37). Independent studies involving other families found HAEIII to be associated with a different mutation affecting the same nucleotide in F12, c.1032CrG (38). Both point mutations translate into amino acid exchanges Thr309Lys and Thr309Arg (identical to position Thr328 if numbering includes the signal peptide), respectively. F12-linked HAEIII is of autosomal dominant inheritance and a mixture of wild-type and Thr309-mutated FXII circulates in plasma of HAEIII patients (37). The position Thr309 is located in the C-terminal proline-rich portion of the FXII heavy chain that mediates FXII surface-induced activation (39) and is associated with increased FXIIa activity in HAEIII patient plasma samples (37). Recently, a F12 gene deletion of 72 base pairs (coding amino acids 305–321) was identified in two unrelated HAEIII families (40). Additionally, in a 37-year-old woman and her daughter with recurrent C1INH-independent angioedema a duplication of 18 base pairs in the F12 gene was found (41). The duplication codes for six additional amino acids in FXII (positions 298–303). The molecular mechanism of oedema formation in patients carrying HAEIIIassociated FXII mutations is unknown and may involve altered FXII activation or processing, reduced binding of C1INH (42), modulation of zymogen cleavage by FXIIa/PK, or other mechanisms. Activation of FXII in angioedema Formation of the vasoactive and proinflammatory peptide hormone BK can in vitro be initiated by a variety of polyanionic surfaces such as kaolin, glass, ellagic acid, certain polymers including nucleotides (DNA and RNA), sulfatides, polyphosphates (polyP), misfolded proteins and some types of collagen or glycosaminoglycans (43). BK binding to its cognate B2 receptor (B2R) activates various intracellular signalling pathways that dilate vessels, induce chaemotaxis of neutrophils and increase vascular permeability and fluid efflux (44). HAE patients experience recurrent attacks of swelling, but the stimuli that trigger these periodic episodes of ex- Thrombosis and Haemostasis 112.5/2014 © Schattauer 2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. Björkqvist et al. Factor XII Targeting FXII Currently available anticoagulants used for the acute treatment and prevention of thrombotic diseases target enzymes of the coagulation cascade that are critical for fibrin generation. As a result, bleeding is the primary complication of anticoagulation therapy (68). In contrast, the selective importance of FXII in thrombus formation while being dispensable for haemostasis, suggests that inhibition of this plasma protease is a safe thromboprotective strategy. In murine models pharmacologic targeting of FXII with H-D-Pro-Phe-Arg-chloromethylketone (PCK) that irreversibly inhibits the amidolytic activity of FXIIa and PK-mediated activation of FXII, provided similar protection from ischaemic stroke as congenital FXII deficiency without an increase in therapy-associated bleeding (18). Pretreatment with PCK markedly reduced cerebral infarction in the transient MCAO model. Furthermore, PCK protected mice from platelet polyP-induced oedema formation (69). The recombinant FXIIa inhibitor rHA-infestin-4 that also inhibits plasmin and modestly factor Xa (70) is based on the fourth domain of the nonclassic Kazal-type serine protease inhibitor from the midgut of the insect Triatoma infestans fused to human albumin (71). Intravenous infusion of the inhibitor prior to the challenge protects mice from FeCl3-induced arterial thrombus formation, ischaemic stroke (transient MCAO model) (71), silent brain ischaemia (72) and from lethal pulmonary embolism (69) and salvages rabbits and rats from arterial thrombosis (70, 71). Similarly, the recombinant inhibitor Ir-CPI, a Kunitz-type protein from the salivary gland of Ixodes ricinus inhibits FXIIa, PK, and FXIa and provides protection from venous and arterial thrombus formation in mice (73). The specific FXIIa inhibitor Corn trypsin inhibitor (CTI) attenuated the prothrombotic properties of catheters in rabbits (74). Other protein inhibitors, such as cabbage seed protease inhibitor (75), pumpkin seed inhibitor CMTI-V (76) and Ecotin (77) block FXIIa in plasma, but also inhibit other coagulation proteases including thrombin, FXa, FXIa, PK and plasmin. The monoclonal anti-FXI antibody 14E11 interferes with FXI activation by FXIIa and provides protection against acute ischaemic stroke (78), arterial occlusion induced by FeCl3 in mice, and reduced platelet-rich thrombus growth in baboons (24). Similarly, the monoclonal anti-FXII zymogen antibody 15H8 reduced fibrin formation and platelet accumulation in a collagen-coated vascular graft in baboons (79) consistent with earlier data of FXII null mice in collagen/epinephrine-triggered pulmonary embolism models (17). The antibody 15H8 directed to zymogen FXII interferes with platelet accumulation in a collagen-coated arterio-venous shunt in baboons. The antibody binding characteristics, its epitope and mechanisms of inhibition are not currently known and interference with the zymogen form bears the risk of an antigen sink. In contrast, recombinant fully human antibody 3F7 binds with high affinity (KD=6.2 ± 0.2 and 4.0 ± 0.1 nM for human and rabbit FXIIa, respectively) into the enzymatic pocket of FXIIa and specifically inhibits FXIIa activity and FXIIa-driven coagulation in human, mouse and rabbit plasma (80). Recently, the clinical applicability of FXIIa inhibition was established in a clinical © Schattauer 2014 Thrombosis and Haemostasis 112.5/2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. Coagulation proteases and CVD cessive vascular leakage are poorly defined (32, 45). In allergic disease, BK is generated and contributes to increased vascular permeability (46). In vitro, heparin liberates BK by triggering contact system activation (33). Using oedema models in genetically modified mice we have shown that heparin activates BK formation in vivo (47). IgE/antigen-activated mast cell-released heparin readily initiates FXII activation. Interference with this pathway either by blocking FXIIa or B2R largely blunts aberrant mast cell-mediated oedema in mice. Clinical data support a role of heparin-triggered BK formation in patients (48). Elevated plasma concentrations of BK directly trigger coughing, a classic side effect of angiotensin converting enzyme (ACE) inhibitors. ACE inhibitors block the major BK degrading enzyme and increase BK plasma concentrations (44). Vice versa, the risk and severity of mast cell-triggered oedema is increased in patients with low ACE activity (49). Heparin appears to have a dual role in FXII activity. It provides the negatively charged surface upon which FXII binds and becomes activated. However, heparin also interacts with antithrombin III (ATIII) (50), through a unique 3-O-sulfated glucosamine unit within the heparin backbone (51). Experimental data show that ATIII-heparin complexes inhibit FXIIa with similar activity as free ATIII (52). Indeed, theoretical models predict a threshold of complete FXII activation or inactivation that is determined by the kinetic balance between the catalytic rate of auto-activation and the rate of FXIIa inhibition (53) that warrant further investigation. During anaphylactic shock the aPTT is markedly prolonged in patient plasma (54, 55). Consistently, plasma of IgE/antigenchallenged mice is unclottable due to a systemic heparin concentration of > 4 µg/ml, that is sufficient to initiate BK formation (47). Initially, small amounts of locally secreted heparin may generate BK activity on the mast cell surface. Mast cells express B2R (56) and BK stimulation induces mast cell degranulation (57). Due to this amplification loop an initial BK activity might be multiplied by liberated mast cell-heparin that triggers the contact system. Heparin specifically triggers FXII-mediated BK formation. Under these conditions no proteolytic-activation of FXI is detectable. Similarly, both the non-natural polysaccharide dextran sulphate (58, 59) and misfolded protein aggregates initiate BK formation in a FXII-dependent manner (60). However, these agents do not induce coagulant activity. FXI and PPK have highly homologous structures and are both bound via HK to cell surfaces (2, 3, 61-63), mechanisms for cell-type specific activation of the kallikrein-kinin system and/or the intrinsic clotting pathway may exist. The mechanisms involve distinct FXII-activation, different forms of FXIIa (64), effects of the activators on downstream inhibitors (65) and other yet unknown regulators. Supporting the concept of selective activation of FXII-driven pathways, HAE patients suffer from recurrent BK-mediated swelling but oedema attacks are not associated with an increased pro-thrombotic risk (66). Similar to HAE type I and II patients, oedema in HAEIII patients is triggered by allergen exposure (67) supporting a role of heparin in initiating BK-mediated oedema in humans. 871 Coagulation proteases and CVD 872 Björkqvist et al. Factor XII setting, when rabbits were adapted to a cardiopulmonary bypass system (ECMO system) used for infant therapy. 3F7 provided thromboprotection as efficient as heparin, however, in contrast to heparin, 3F7 treatment did not impair the haemostatic capacity of treated animals (80). An alternative method to interfere with FXII action is the use of antisense oligonucleotides (ASOs) (81). Repetitive subcutaneous ASO injection for several weeks depressed expression of FXII in mice and rabbits. Consistent to the gene-ablated mouse data, depletion of FXII by ASO reduced arterial and venous thrombosis in mice (81). ASO attenuates catheter-induced thrombosis in rabbits (82), confirming 3F7-mediated inhibition of occlusive clot formation in polymer-tubing shunts (80). Furthermore, inhibition of FXII by ASO reversed C1INH deficiency-induced increased vascular permeability in mice (83). The major drawback of ASO is the slow onset of action that may hamper its use as an anticoagulant in invasive procedures or any other medical setting that requires acute intervention. Taken together, targeting FXII using different technologies shows safe thromboprotection in mice, rabbits and baboons and interferes with oedema formation in mice. The FXII activator polyphosphate Although FXII is activated in vitro by a variety of non-physiologic polyanions, the in vivo activator of FXII remained an enigma for decades. FXII activation by contact to the inorganic polyanionic mineral kaolin (a silicate), is commonly used to trigger aPTT, however an inorganic silicate does not exist under physiologic conditions in humans. FXII activation has been linked to procoagulant platelets in plasma and multiple studies have shown that activated platelets promote coagulation in a FXII-dependent manner (58, 84–87). Consistently, platelet-derived microparticles induce thrombin generation independently of tissue factor via activation of FXII (88). Taken together the ex vivo data show that procoagulant platelets initiate FXII-mediated fibrin formation. The critical role of FXII in thrombus formation has led to the search for naturally occurring platelet-derived FXII activators. Initially, extracellular RNA was identified as a FXII activator and targeting the phosphodiester bonds in the polymer backbone with RNAse provided thromboprotection in mouse models (89). Polyphosphates (polyP) comprise an inorganic polymer that shares a similar polyanion structure as RNA. Synthetic polyP of 70 phosphate units initiate coagulation in a FXII-dependent manner in plasma (90). Soluble platelet polyP are composed of 60–100 linear linked phosphate subunits and are released from platelet dense granules upon PAR-receptor stimulation (91). Using experiments in plasma, thrombosis and oedema models in genetically altered mice, along with a human disease model, we have identified platelet polyP as an activator of FXII and have shown that polyPdriven FXII activation has critical functions in platelet-driven thrombosis and inflammation in vivo (69). Independent laboratories have confirmed that platelet polyP initiate coagulation in a FXII-dependent manner in vitro (90, 92–95) and thrombus formation in vivo (96). Platelet polyP are unstable and the polyP/ FXII pathway operates independently of tissue factor-driven coagulation (97). Ex vivo, the ability of polyP to activate FXII is dependent on the chain length (95). Polymers of < 45 residues do not sustain FXII activation (69) and FXII-activating capacity increases with the polyP chain length. However, the FXII activating property of polyP may not be solely dependent on chain length in vivo. Long chain polyP are insoluble (98) and do not naturally occur in humans under physiologic conditions in circulation or the extracellular compartment. In contrast, platelet-derived polyP are soluble, present in plasma and can reach high local local concentrations in an entrapped environment which activate FXII in the context of a platelet rich thrombus. Indeed, inherited deficiency in platelet polyP results in defective thrombus formation in mice (96) and prolonged clotting in platelet rich plasma that is restored to normal levels by addition of platelet size synthetic polyP (69). In addition to activation of coagulation via FXII, polyP accelerates generation of factor V activation. PolyP also accelerate FXI acti- Figure 3: Platelet polyphosphate activities. Activated platelets release polyP from their dense granules. The polymer activates FXII and induces clot formation via the intrinsic pathway of coagulation and oedema formation via the kallikreinkinin system. Furthermore, polyP accelerate factor V (FV) activation (FVa), factor XI (FXI) activation by thrombin and enhance fibrin clot structure. PolyP bind to histone H4 (H4) that in turn activates platelets. Thrombosis and Haemostasis 112.5/2014 © Schattauer 2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. vation by thrombin, and enhance the stability of the fibrin clot (90, 92–95). Targeting polyP activity provides protection from thrombosis (69, 99) and vascular leakage (100) in animal models (▶ Figure 3). Extracellular histone H4 contributes to organ failure and sepsisassociated death (101). Histones activate platelets, interact with platelet-secreted polyP thus, amplifying thrombus formation (93). The binding of platelet-size polyP to the inflammatory mediators histone H4 and high mobility group box 1 (HMGB1) potentiates proinflammatory activities in vitro and in vivo (102). Conclusions FXII influences thrombosis risk without altering haemostasis. It also plays a role in inflammation, sepsis and HAE. Recently identified in vivo activators of FXII include mast cell-derived heparin, misfolded protein aggregates, nucleotides and platelet polyP. While heparin and misfolded protein aggregates selectively activate the kallikrein-kinin system and increase vascular leakage, platelet-derived polyP has a precise role in coagulation amplification and oedema formation. Anti-FXIIa antibodies have a long half-life in the circulation and have been shown to provide safe anticoagulation in a clinically relevant extracorporeal circulation bypass model. These properties have renewed interest in FXII as a therapeutic strategy to treat aberrant vascular leakage and thrombosis disorders. Acknowledgements This work was supported in part by grants from the Hjärt Lungfonden (20110500), Stockholms läns landsting (ALF, 2110471), Cancerfonden (100615), Vetenskapsrådet (K2013–65X-21462–04–5), German Research Society (SFB841/TP B8; SFB877/TP A11), and a European Research Council grant (ERCStG-2012–311575_F-12) to TR. Conflicts of interest None declared. References 1. Renne T, et al. In vivo roles of factor XII. Blood 2012; 120: 4296–4303. 2. Herwald H, et al. Mapping of the discontinuous kininogen binding site of prekallikrein. A distal binding segment is located in the heavy chain domain A4. J Biol Chem 1996; 271: 13061–13067. 3. Renne T, et al. Mapping of the discontinuous H-kininogen binding site of plasma prekallikrein. Evidence for a critical role of apple domain-2. J Biol Chem 1999; 274: 25777–25784. 4. Muller F, Renne T. Novel roles for factor XII-driven plasma contact activation system. Curr Opin Hematol 2008; 15: 516–521. 5. Bjorkqvist J, et al. Plasma kallikrein: the bradykinin-producing enzyme. Thromb Haemost 2013; 110: 399–407. 6. Stavrou E, Schmaier AH. Factor XII: what does it contribute to our understanding of the physiology and pathophysiology of haemostasis & thrombosis. Thromb Res 2010; 125: 210–215. 7. Renne T. The Factor XII-Driven plasma Contact System. In: Textbook of Haemostasis and Thrombosis – Basic principles and clinical practice. 6th ed. Lippincott Williams & Wilkins 2013; pp. 242–53. 8. Cool DE, MacGillivray RT. Characterization of the human blood coagulation factor XII gene. Intron/exon gene organization and analysis of the 5’-flanking region. J Biol Chem 1987; 262: 13662–13673. 9. Cochrane CG, et al. Activation of Hageman factor in solid and fluid phases. A critical role of kallikrein. J Exp Med 1973; 138: 1564–1583. 10. Samuel M, et al. Human factor XII (Hageman factor) autoactivation by dextran sulfate. Circular dichroism, fluorescence, and ultraviolet difference spectroscopic studies. J Biol Chem 1992; 267: 19691–19697. 11. Pixley RA, et al. The regulation of human factor XIIa by plasma proteinase inhibitors. J Biol Chem 1985; 260: 1723–1729. 12. Siegerink B, et al. Intrinsic coagulation activation and the risk of arterial thrombosis in young women: results from the Risk of Arterial Thrombosis in relation to Oral contraceptives (RATIO) case-control study. Circulation 2010; 122: 1854–1861. 13. de Agostini A, et al. Inactivation of factor XII active fragment in normal plasma. Predominant role of C-1-inhibitor. J Clin Invest 1984; 73: 1542–1549. 14. Maas C, Renne T. Regulatory mechanisms of the plasma contact system. Thromb Res 2012;129 (Suppl 2): 73–76. 15. Ratnoff OD, Margolius A, Jr. Hageman trait: an asymptomatic disorder of blood coagulation. Trans Assoc Am Physicians 1955; 68: 149–154. 16. Pauer HU, et al. Targeted deletion of murine coagulation factor XII gene-a model for contact phase activation in vivo. Thromb Haemost 2004; 92: 503–508. 17. Renne T, et al. Defective thrombus formation in mice lacking coagulation factor XII. J Exp Med 2005; 202: 271–281. 18. Kleinschnitz C, et al. Targeting coagulation factor XII provides protection from pathological thrombosis in cerebral ischaemia without interfering with haemostasis. J Exp Med 2006; 203: 513–518. 19. Pham M, et al. Enhanced cortical reperfusion protects coagulation factor XIIdeficient mice from ischaemic stroke as revealed by high-field MRI. Neuroimage 2010; 49: 2907–2914. 20. Muller F, et al. Factor XI and XII as antithrombotic targets. Curr Opin Hematol 2011; 18: 349–355. 21. Johnson CY, et al. The factor XII –4C>T variant and risk of common thrombotic disorders: A HuGE review and meta-analysis of evidence from observational studies. Am J Epidemiol 2011; 173: 136–144. 22. Girolami A, et al. Rebuttal: factor XII levels, factor XII 46 C>T polymorphism and venous thrombosis: a word of caution is needed. Thromb Haemost 2004; 92: 892–893; author reply 894–895. 23. Bird JE, et al. Effects of plasma kallikrein deficiency on haemostasis and thrombosis in mice: murine ortholog of the Fletcher trait. Thromb Haemost 2012; 107: 1141–1150. 24. Cheng Q, et al. A role for factor XIIa-mediated factor XI activation in thrombus formation in vivo. Blood 2010; 116: 3981–3989. 25. Salomon O, et al. Reduced incidence of ischaemic stroke in patients with severe factor XI deficiency. Blood 2008; 111: 4113–4117. 26. Salomon O, et al. Patients with severe factor XI deficiency have a reduced incidence of deep-vein thrombosis. Thromb Haemost 2011; 105: 269–273. 27. Doggen CJ, et al. Levels of intrinsic coagulation factors and the risk of myocardial infarction among men: Opposite and synergistic effects of factors XI and XII. Blood 2006; 108: 4045–4051. 28. Iwaki T, Castellino FJ. Plasma levels of bradykinin are suppressed in factor XIIdeficient mice. Thromb Haemost 2006; 95: 1003–1010. 29. Schloesser M, et al. Mutations in the human factor XII gene. Blood 1997; 90: 3967–3977. 30. Miyata T, et al. Coagulation factor XII (Hageman factor) Washington D. C.: inactive factor XIIa results from Cys-571----Ser substitution. Proc Natl Acad Sci USA 1989; 86: 8319–8322. 31. Hovinga JK, et al. Coagulation factor XII Locarno: the functional defect is caused by the amino acid substitution Arg 353-->Pro leading to loss of a kallikrein cleavage site. Blood 1994; 84: 1173–1181. 32. Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J Med 2008; 359: 1027–1036. 33. Bjorkqvist J, et al. Hereditary angioedema: a bradykinin-mediated swelling disorder. Thromb Haemost 2013; 109: 368–374. 34. Han ED, et al. Increased vascular permeability in C1 inhibitor-deficient mice mediated by the bradykinin type 2 receptor. J Clin Invest 2002; 109: 1057–1063. 35. Cugno M, et al. Bradykinin and the pathophysiology of angioedema. Int Immunopharmacol 2003; 3: 311–317. © Schattauer 2014 Thrombosis and Haemostasis 112.5/2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. 873 Coagulation proteases and CVD Björkqvist et al. Factor XII Coagulation proteases and CVD 874 Björkqvist et al. Factor XII 36. Bork K, et al. Hereditary angioedema with normal C1-inhibitor activity in women. Lancet 2000; 356: 213–217. 37. Cichon S, et al. Increased activity of coagulation factor XII (Hageman factor) causes hereditary angioedema type III. Am J Hum Genet 2006; 79: 1098–1104. 38. Dewald G, Bork K. Missense mutations in the coagulation factor XII (Hageman factor) gene in hereditary angioedema with normal C1 inhibitor. Biochem Biophys Res Commun 2006; 343: 1286–1289. 39. Citarella F, et al. Structure/function analysis of human factor XII using recombinant deletion mutants. Evidence for an additional region involved in the binding to negatively charged surfaces. Eur J Biochem 1996; 238: 240–249. 40. Bork K, et al. A novel mutation in the coagulation factor 12 gene in subjects with hereditary angioedema and normal C1-inhibitor. Clin Immunol 2011; 141: 31–35. 41. Kiss N, et al. Novel duplication in the F12 gene in a patient with recurrent angioedema. Clin Immunol 2013; 149: 142–145. 42. Moreno AS, et al. Structural and Molecular Changes Caused By Mutations Thr328Lys and Thr328Arg In FXII Associated With Hereditary Angioedema With Normal C1 Inhibitor. J Allergy Clin Immunol 2014; 133: 39. 43. Maas C, et al. The plasma contact system 2.0. Semin Thromb Haemost 2011; 37: 375–381. 44. Leeb-Lundberg LM, et al. International union of pharmacology. XLV. Classification of the kinin receptor family: from molecular mechanisms to pathophysiological consequences. Pharmacol Rev 2005; 57: 27–77. 45. Davis AE, 3rd. Hereditary angioedema: a current state-of-the-art review, III: mechanisms of hereditary angioedema. Ann Allergy Asthma Immunol 2008; 100 (Suppl 2): 7–12. 46. Kaplan AP. Kinins, airway obstruction, and anaphylaxis. Chem Immunol Allergy 2010; 95: 67–84. 47. Oschatz C, et al. Mast cells increase vascular permeability by heparin-initiated bradykinin formation in vivo. Immunity 2011; 34: 258–268. 48. MacLaughlin EJ, et al. Anaphylactoid reaction to enoxaparin in a patient with deep venous thrombosis. Pharmacotherapy 2002; 22: 1511–1515. 49. Summers CW, et al. Factors predicting anaphylaxis to peanuts and tree nuts in patients referred to a specialist center. J Allergy Clin Immunol 2008; 121: 632–638 e2. 50. Colman RW, et al. Effect of heparin on the inhibition of the contact system enzymes. Ann NY Acad Sci 1989; 556: 95–103. 51. Capila I, Linhardt RJ. Heparin-protein interactions. Angew Chem Int Ed Engl 2002; 41: 391–412. 52. Pixley RA, et al. Effect of heparin on the inactivation rate of human activated factor XII by antithrombin III. Blood 1985; 66: 198–203. 53. Beltrami E, Jesty J. Mathematical analysis of activation thresholds in enzymecatalyzed positive feedbacks: application to the feedbacks of blood coagulation. Proc Natl Acad Sci USA 1995; 92: 8744–8748. 54. Lombardini C, et al. „Heparinization“ and hyperfibrinogenolysis by wasp sting. Am J Emerg Med 2009; 27: 1176 e1–3. 55. Mazzi G, et al. Primary hyperfibrinogenolysis in a patient with anaphylactic shock. Haematologica 1994; 79: 283–285. 56. Dlamini Z, Bhoola KD. Upregulation of tissue kallikrein, kinin B1 receptor, and kinin B2 receptor in mast and giant cells infiltrating oesophageal squamous cell carcinoma. J Clin Pathol 2005; 58: 915–922. 57. Ishizaka T, et al. Release of histamine and arachidonate from mouse mast cells induced by glycosylation-enhancing factor and bradykinin. J Immunol 1985; 134: 1880–1887. 58. Johne J, et al. Platelets promote coagulation factor XII-mediated proteolytic cascade systems in plasma. Biol Chem 2006; 387: 173–178. 59. Bjorkqvist J, et al. Zinc-dependent contact system activation induces vascular leakage and hypotension in rodents. Biol Chem 2013; 394: 1195–1204. 60. Maas C, et al. Misfolded proteins activate factor XII in humans, leading to kallikrein formation without initiating coagulation. J Clin Invest 2008; 118: 3208–3218. 61. Renne T, et al. Characterization of the H-kininogen-binding site on factor XI: a comparison of factor XI and plasma prekallikrein. J Biol Chem 2002; 277: 4892–4899. 62. Renne T, Muller-Esterl W. Cell surface-associated chondroitin sulfate proteoglycans bind contact phase factor H-kininogen. FEBS Lett 2001; 500: 36–40. 63. Renne T, et al. Local bradykinin formation is controlled by glycosaminoglycans. J Immunol 2005; 175: 3377–3385. 64. Schmaier AH. The elusive physiologic role of Factor XII. J Clin Invest 2008; 118: 3006–3009. 65. Kishimoto TK, et al. Contaminated heparin associated with adverse clinical events and activation of the contact system. N Engl J Med 2008; 358: 2457–2467. 66. Nzeako UC, et al. Hereditary angioedema: a broad review for clinicians. Arch Intern Med 2001; 161: 2417–2429. 67. Bork K, et al. Hereditary angioedema caused by missense mutations in the factor XII gene: clinical features, trigger factors, and therapy. J Allergy Clin Immunol 2009; 124: 129–134. 68. Eikelboom JW, Weitz JI. New anticoagulants. Circulation 2010; 121: 1523–1532. 69. Muller F, et al. Platelet polyphosphates are proinflammatory and procoagulant mediators in vivo. Cell 2009; 139: 1143–1156. 70. Xu Y, et al. Factor XIIa inhibition by Infestin-4: in vitro mode of action and in vivo antithrombotic benefit. Thromb Haemost 2013; 111: 694–704. 71. Hagedorn I, et al. Factor XIIa inhibitor recombinant human albumin Infestin-4 abolishes occlusive arterial thrombus formation without affecting bleeding. Circulation 2010; 121: 1510–1517. 72. Chen JW, et al. Selective factor XIIa inhibition attenuates silent brain ischaemia: application of molecular imaging targeting coagulation pathway. JACC Cardiovasc Imaging 2012; 5: 1127–1138. 73. Decrem Y, et al. Ir-CPI, a coagulation contact phase inhibitor from the tick Ixodes ricinus, inhibits thrombus formation without impairing haemostasis. J Exp Med 2009; 206: 2381–2395. 74. Yau JW, et al. Corn trypsin inhibitor coating attenuates the prothrombotic properties of catheters in vitro and in vivo. Acta Biomater 2012; 8: 4092–4100. 75. Carter TH, et al. Cabbage seed protease inhibitor: a slow, tight-binding inhibitor of trypsin with activity toward thrombin, activated Stuart factor (factor Xa), activated Hageman factor (factor XIIa), and plasmin. Blood 1990; 75: 108–115. 76. Hojima Y, et al. Pumpkin seed inhibitor of human factor XIIa (activated Hageman factor) and bovine trypsin. Biochemistry 1982; 21: 3741–3746. 77. Ulmer JS, et al. Ecotin is a potent inhibitor of the contact system proteases factor XIIa and plasma kallikrein. FEBS Lett 1995; 365: 159–163. 78. Leung PY, et al. Inhibition of Factor XII-Mediated Activation of Factor XI Provides Protection Against Experimental Acute Ischaemic Stroke in Mice. Transl Stroke Res 2012; 3: 381–389. 79. Matafonov A, et al. Factor XII inhibition reduces thrombus formation in a primate thrombosis model. Blood 2014; 123: 1739–1746. 80. Larsson M, et al. A Factor XIIa Inhibitory Antibody Provides Thromboprotection in Extracorporeal Circulation Without Increasing Bleeding Risk. Sci Transl Med 2014; 6: 222ra17. 81. Revenko AS, et al. Selective depletion of plasma prekallikrein or coagulation factor XII inhibits thrombosis in mice without increased risk of bleeding. Blood 2011; 118: 5302–5311. 82. Yau JW, et al. Selective depletion of factor XI or factor XII with antisense oligonucleotides attenuates catheter thrombosis in rabbits. Blood 2014; 123: 2102–2107. 83. Bhattacharjee G, et al. Inhibition of vascular permeability by antisense-mediated inhibition of plasma kallikrein and coagulation factor 12. Nucleic Acid Ther 2013; 23: 175–187. 84. Back J, et al. Activated human platelets induce factor XIIa-mediated contact activation. Biochem Biophys Res Commun 2010; 391: 11–17. 85. Walsh PN, Griffin JH. Contributions of human platelets to the proteolytic activation of blood coagulation factors XII and XI. Blood 1981; 57: 106–118. 86. Walsh PN. The role of platelets in the contact phase of blood coagulation. Br J Haematol 1972; 22: 237–254. 87. Castaldi PA, et al. Availability of platelet Factor 3 and activation of factor XII in thrombasthenia. Nature 1965; 207: 422–424. 88. Van Der Meijden PE, et al. Platelet- and erythrocyte-derived microparticles trigger thrombin generation via factor XIIa. J Thromb Haemost 2012; 10: 1355–1362. 89. Kannemeier C, et al. Extracellular RNA constitutes a natural procoagulant cofactor in blood coagulation. Proc Natl Acad Sci USA 2007; 104: 6388–6393. 90. Smith SA, et al. Polyphosphate modulates blood coagulation and fibrinolysis. Proc Natl Acad Sci USA 2006; 103: 903–908. 91. Rao NN, et al. Inorganic polyphosphate: essential for growth and survival. Annu Rev Biochem 2009; 78: 605–647. 92. Choi SH, et al. Polyphosphate is a cofactor for the activation of factor XI by thrombin. Blood 2011; 118: 6963–6970. Thrombosis and Haemostasis 112.5/2014 © Schattauer 2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. 93. Semeraro F, et al. Extracellular histones promote thrombin generation through platelet-dependent mechanisms: involvement of platelet TLR2 and TLR4. Blood 2011; 118: 1952–1961. 94. Mutch NJ, et al. Polyphosphate modifies the fibrin network and down-regulates fibrinolysis by attenuating binding of tPA and plasminogen to fibrin. Blood 2010; 115: 3980–3988. 95. Smith SA, et al. Polyphosphate exerts differential effects on blood clotting, depending on polymer size. Blood 2010; 116: 4353–4359. 96. Ghosh S, et al. Inositol hexakisphosphate kinase 1 maintains haemostasis in mice by regulating platelet polyphosphate levels. Blood 2013; 122: 1478–1486. 97. Nickel KF, et al. Time-dependent degradation and tissue factor addition mask the ability of platelet polyphosphates in activating factor XII-mediated coagulation. Blood 2013; 122: 3847–3849. 98. Kulaev IS, et al. The Peculiarities of Polyphosphate Metabolism in Different Organism. In: Textbook of The Biochemistry of inorganic polyphosphate. 2nd ed. John Wiley & Son 2004; pp. 177–181. 99. Smith SA, et al. Inhibition of polyphosphate as a novel strategy for preventing thrombosis and inflammation. Blood 2012; 120: 5103–5110. 100. Bae JS, et al. Polyphosphate elicits pro-inflammatory responses that are counteracted by activated protein C in both cellular and animal models. J Thromb Haemost 2012; 10: 1145–1151. 101. Xu J, et al. Extracellular histones are major mediators of death in sepsis. Nat Med 2009; 15: 1318–1321. 102. Dinarvand P, et al. Polyphosphate amplifies proinflammatory responses of nuclear proteins through interaction with receptor for advanced glycation end products and P2Y1 purinergic receptor. Blood 2014; 123: 935–945. © Schattauer 2014 Thrombosis and Haemostasis 112.5/2014 Downloaded from www.thrombosis-online.com on 2017-06-11 | IP: 88.99.165.207 For personal or educational use only. No other uses without permission. All rights reserved. 875 Coagulation proteases and CVD Björkqvist et al. Factor XII