Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
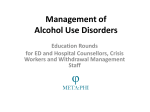
ED Management of Opioid Use Disorders Educational Rounds for ED Physicians META:PHI 2015 About META:PHI Mentoring, Education, and Clinical Tools for Addiction: Primary Care–Hospital Integration • Goals: – Promote evidence-based addiction medicine treatment – Implement care pathways between the ED, hospital, WMS, primary care, and rapid access addiction medicine clinics • Seven sites in Ontario are currently involved, with plans to expand the spread of the project in the future • Funding and support provided by the Adopting Research to Improve Care (ARTIC) program (Council of Academic Hospitals of Ontario & Health Quality Ontario) https://www.porticonetwork.ca/web/meta-phi META:PHI 2015 Baseline Survey The baseline survey is anonymous and entirely optional. You may skip any question that you do not wish to answer. We will not ask you for any personal information. Please tear off and keep the front page with contact information, should you have any questions about the survey or the META:PHI project. Please return the completed or incomplete survey face down to the facilitator when you leave the presentation. OVERVIEW META:PHI 2015 Management Goals for OUD Patients in the ED 1. Treat presenting problem (overdose, withdrawal, infection, pain etc.). 2. Initiate bup/nx treatment in the ED when appropriate 3. Prevent overdose through patient education and naloxone 4. Provide rapid access to an outpatient addiction medicine clinic for long-term medication-assisted treatment META:PHI 2015 IDENTIFYING AND DIAGNOSING AN OPIOID USE DISORDER META:PHI 2015 Identifying & Diagnosing an OUD (1) • Difficult to diagnose if patient doesn’t disclose use • Maintain high index of suspicion with risk factors: – Younger, male, psychiatric comorbidity, concurrent addiction to other drugs, on high prescribed opioid doses • Common presentations: – Overdose, withdrawal, drug seeking, infections from injection drug use, depression and suicidal ideation, trauma META:PHI 2015 Identifying & Diagnosing an OUD (2) Indications of an OUD 1. Check for physical signs: track marks, pinpoint pupils, slurred speech, nodding off (intoxication), restlessness (withdrawal) 2. Check pharmacy dispensing record for patients on Ontario Drug Benefits 3. Ask about opioid use and withdrawal symptoms META:PHI 2015 TREATING OPIOID OVERDOSE META:PHI 2015 Treating Opioid Overdose in the ED (1) • Provide naloxone drip and respiratory support • Monitor for at least six hours after respiratory support discontinued – Monitor patients for 10 hours if the patient has had a methadone overdose • Resume respiratory support and naloxone drip if signs of toxicity return during the six- to ten-hour interval • Most sensitive indicator of toxicity: Slurred speech or ‘nodding off’ while engaged in conversation over several minutes META:PHI 2015 Treating Opioid Overdose in the ED (2) • Initiate bup/nx if the patient experiences withdrawal (after naloxone is discontinued) • Do not prescribe opioids during ED/hospital stay • If the patient demands to leave while still intoxicated and you feel they are at high risk for overdose death or injury, inform them you will complete a Form I – Indicate on the Form I that the patient is suffering from an opioid use disorder, which puts them at imminent risk of self-harm META:PHI 2015 OPIOID WITHDRAWAL META:PHI 2015 Clinical Features of Opioid Withdrawal • Time course Symptoms start six hours after last use of IR opioid, peak at 2-3 days, and begin to resolve by 5-7 days (psychological symptoms, can last for weeks) • Physical symptoms Flu-like (myalgias, chills, nausea and vomiting, abdominal cramps, diarrhea, rhinorrhea, lacrimation, piloerection) • Psychological symptoms Insomnia, extreme anxiety/irritability, dysphoria, drug craving • Complications Exacerbation of psychiatric conditions, suicide, overdose if opioids taken after a period of abstinence, gastric or duodenal ulcer, acute exacerbation of cardiorespiratory illnesses, miscarriage or premature labour in pregnancy META:PHI 2015 Treatment of withdrawal 1. Buprenorphine/naloxone (bup/nx) 2. Clonidine META:PHI 2015 What is Buprenorphine/naloxone (bup/nx)? • Sublingual tablet, with long duration of action • Partial opioid agonist with a ceiling effect – Doses beyond 24 mg - 32 mg do not have any additional opioid effects – Therefore bup/nx is much less likely to cause overdose than methadone or other potent opioids • Binds very tightly to receptor – Displaces other opioids (displacement of fentanyl is slower and less complete) – Can precipitate withdrawal when taken shortly after opioid use META:PHI 2015 Opioids replaced and blocked by buprenorphine (Image from naabt.org) Bup/nx for the Treatment of Withdrawal (1) • To avoid precipitating withdrawal, don’t give bup/nx until at least 12 hours have elapsed since last opioid use and patient has withdrawal symptoms • A score of 12 or more on the Clinical Opioid Withdrawal Scale (COWS) indicates that it is safe to administer bup/nx • If the patient is not in withdrawal but will likely be in 2-3 hours, keep in ED until safe to give bup/nx • If more than 2-3 hours before onset of withdrawal, discharge and give referral card for RAAM • Or send to WMS, with instructions to return to ED when in withdrawal META:PHI 2015 Clinical Opioid Withdrawal Scale Interval Date Time Resting heart rate (measure after lying or sitting for 1 minute) 0 HR 80 or below 1 HR 81-100 2 HR 101-120 4 HR greater than 120 Sweating (preceding 30 mins and not related to room temp /activity) 0 No report of chills/flushing 1 Subjective report of chills/flushing 2 Flushed or observable moistness on face 3 Beads of sweat on brow or face 4 Sweat streaming off face Restlessness (observe during assessment) 0 Able to sit still 1 Reports difficulty sitting still but able to do so 3 Frequent shifting or extraneous movements of legs/arm 5 Unable to sit still for more than a few seconds Pupil size 0 Pupils pinned or normal size for room light 1 Pupils possibly larger than normal for room light 2 Pupils moderately dilated 5 Pupils so dilated that only the rim of the iris is visible Bone or joint aches (not including existing joint aches) 0 Not present 1 Mild diffuse discomfort 2 Patient reports severe diffuse aching of joints/muscles 4 Patient is rubbing joints / muscles plus unable to sit still due to discomfort META:PHI 2015 0 30m 2h 4h Interval Date Time Runny nose or tearing (not related to URTI or allergies) 0 Not present 1 Nasal stuffiness or unusually moist eyes 2 Nose running or tearing 4 Nose constantly running or tears streaming down cheeks GI upset (over last 30 minutes) 0 No GI symptoms 1 Stomach cramps 2 Nausea or loose stool 3 Vomiting or diarrhoea 5 Multiple episodes of vomiting or diarrhoea Tremor 0 No tremor 1 Tremor can be felt, but not observed 2 Slight tremor observable 4 Gross tremor or muscle twitching Yawning (observe during assessment) 0 No yawning 1 Yawning once or twice during assessment 2 Yawning three or more times during assessment 4 Yawning several times/minute Anxiety or irritability 0 None 1 Patient reports increasing irritability or anxiousness 2 Patient obviously irritable or anxious 4 Patient so irritable or anxious that participation in the assessment is difficult Gooseflesh skin 0 Skin is smooth 3 Piloerection (goosebumps) of skin can be felt or hair standing up on arms 5 Prominent piloerection 5-12 Mild withdrawal 13-24 Moderate withdrawal 25-36 Moderately severe withdrawal > 36 Severe withdrawal META:PHI 2015 TOTAL INITIALS 0 30m 2h 4h Bup/nx for the Treatment of Withdrawal (2) • Initial dose: 4 mg SL (takes several minutes to dissolve) – Give only 2 mg SL if patient is elderly or on a high benzodiazepine dose, or if you’re unsure if the patient is in withdrawal • Reassess in 1-2 hours – If substantial improvement of withdrawal, give 2-4 mg SL to take-home for later in day, plus an outpatient script – If still in significant withdrawal, give another 4 mg SL in the ED and reassess again in 1-2 hours • Treatment complete when 4-12 mg have been dispensed and withdrawal symptoms are minimal META:PHI 2015 Outpatient Prescription • Prescribe the total amount given in ED as a single dose, dispensed daily under observation • LU 437 or 438 – 437 – high risk for methadone toxicity (elderly, on benzodiazepines, heavy drinker, non-daily opioid use or codeine use) – 438 – no methadone prescriber in community or waiting list 3+ months • Script should last until next RAAM clinic; advise patient to attend clinic (give referral card) for additional bup/nx treatment • Refer patient to WMS if: has transient housing, lack of social supports, and/or at high risk for relapse – Find out what pharmacy uses – put pharmacy name on script and fax – write note to WMS informing them of the bup/nx script and advising them that patient should attend next RAAM clinic META:PHI 2015 Sample bup/nx Prescription Patient Health card number Date of birth Pharmacy Address Fax number Date: Buprenorphine/naloxone 8/2 mg 1 tab SL OD February 12 – February 16, 2018 inclusive Dispense daily observed LU 437/438 Physician signature CPSO number META:PHI 2015 Bup/nx use in Methadone Patients • Bup/nx can trigger very severe withdrawal when given to methadone patients, even if 72 hours or more have elapsed since last methadone dose • Therefore, give bup/nx only under supervision of a methadone prescriber • If methadone patient requires admission and has no access to methadone, don’t use bup/nx; use oral controlled-release morphine titrated to relieve withdrawal symptoms META:PHI 2015 Bup/nx Versus Methadone Methadone Bup/nx Effectiveness as maintenance treatment Very effective Effective but less than methadone Overdose risk Very high Low Who can prescribe Need a special licence Any MD Rx of acute withdrawal Not safe or practical (takes weeks to reach optimal dose) Very effective Optimal dose reached within 1-3 days META:PHI 2015 CPSO Stance on Bup/Nx Prescribing & Training • Previously, the CPSO had a policy outlining expectations for physicians who wished to prescribe buprenorphine – This policy recommended advanced training and education in order to prescribe the medication • This has recently changed! • The CPSO has maintained that physicians do not need a methadone license to prescribe bup/nx and has removed its recommendation that physicians have specialized bup/nx prescribing training – Recommendation has been replaced with a reminder that ‘as with any drug the College expects that all physicians who wish to use buprenorphine will have the requisite knowledge about its intended impacts, side effects and role in addiction treatment’ META:PHI 2015 Clonidine Treatment of Withdrawal • Not as effective as bup/nx for symptom relief or treatment retention • Clonidine 0.1 mg PO qid PRN; increase to 0.2 mg if able to check BP prior to dose (hold if BP < 90/60) • Discharge home or WMS with prescription for 3-5 days • Additional meds for symptom relief: anti-emetics, e.g., gravol; trazodone for sleep; Naprosyn for myalgias • Warn patients that they are at high risk for overdose if they relapse to usual opioid dose • Refer to RAAM clinic (give referral card if available) META:PHI 2015 DISCHARGING PATIENTS WITH AN OPIOID USE DISORDER META:PHI 2015 Advice on Discharge • Advise patient that they have lost tolerance and that they could overdose again if they use their usual dose • Inform patient of overdose prevention strategies and provide with 1-2 vials of naloxone • Refer the patient to the RAAM clinic (give referral card) • If bup/nx prescribed during ED visit, give bridging script until patient can be seen at RAAM clinic • Inform patient’s family doctor, especially if the doctor has been prescribing opioids META:PHI 2015 Case Scenario – Karen Part 1 Karen is a 30 year old woman who was brought by her friends to the ED after an accidental overdose after injecting fentanyl purchased from a ‘friend’. She was given a naloxone drip and respiratory support. These were discontinued a half hour ago. Her O2 saturation is currently normal. The physician is requesting that Karen stay for several more hours of observation, but Karen is very angry and wants to go home. META:PHI 2015 Question • What medical intervention would you do in the ED prior to discharge? META:PHI 2015 Medical Intervention • Treat withdrawal with buprenorphine/naloxone in the ED • Start bup/nx when: – Patient is not on naloxone – Patient is in withdrawal – 12 hours have passed since last fentanyl dose META:PHI 2015 Case Scenario - Karen Part 2 Karen is feeling better after taking 8mg of bup/nx . After six hours of observation she shows no signs of opioid toxicity and is now ready for discharge. META:PHI 2015 Question • What would be your discharge plan for Karen? META:PHI 2015 Discharge Plan - Provide bridging prescription for bup/nx until patient can be seen at RAAM - Provide RAAM referral - Give advice on overdose prevention - Provide patient with naloxone kit META:PHI 2015 Who is at Risk for Opioid Overdose? • Opioid-addicted patients who inject, smoke, or snort opioids • Recently abstinent opioid-addicted patients – E.g., patients discharged from a treatment program, withdrawal management, prison, or hospital • Binge opioid users • Patients on very high prescribed doses (eg > 400 mg MED) • Patients who use opioids and also take benzodiazepines or drink heavily META:PHI 2015 Advice to Patients on Preventing Overdose (1) • If you relapse after being abstinent for a few days or longer, you have lost tolerance and could die if you take your usual dose. • To avoid overdose: – do not inject – take a much smaller opioid dose than usual. – Take a ‘test dose’ unless you got the drug directly from a doctor’s prescription. – Don’t mix opioids with alcohol/benzos. – Always have a friend with you if you inject or snort opioids. META:PHI 2015 Advice to Patients on Preventing Overdose (2) • If one of your friends appears drowsy, has slurred speech, or is “nodding off” after taking opioids: Shake/talk to them to keep them awake. If they can’t be woken up, call 911 and start chest compressions. Don’t let your friend ‘sleep it off,’ even if someone watches them overnight. META:PHI 2015 Advice to Patients on Preventing Overdose (3) • The best way to avoid an overdose is to get treatment for your addiction. Please attend the next rapid access addiction medicine clinic. Give referral card and tell them when and where the clinic is. Tell them that they don’t need an appointment; they can just show up during clinic hours. Carry naloxone META:PHI 2015 Distribute Take-Home Naloxone to Patients at High Risk of Overdose • Not on methadone or bup/nx, on these medications but started in the past two weeks, or on these medications but continuing to use substances • On high dose opioids for chronic pain • Treated for overdose (or reports a past overdose) • Injects, crushes, smokes or snorts potent opioids (fentanyl, morphine, hydromorphone, oxycodone) • Buys methadone or other opioids from the street • Recently discharged from an abstinence-based treatment program, WMS, hospital, or prison • Uses opioids with benzos and/or alcohol META:PHI 2015 Contents of Naloxone Kit – One to two naloxone vials – Two syringes – Alcohol wipes – ID card explaining why patient is carrying medication and syringes META:PHI 2015 Administering Naloxone Instruct patient on naloxone use: - Shake the overdose victim, call their name - If they cannot be fully woken up, call 911 - Inject a full naloxone vial into an arm or leg muscle - Start chest compressions - Inject another vial if they don’t wake up in 3-4 minutes META:PHI 2015 Outpatient Psychiatry Referral • Refer patient to outpatient psychiatry if patient: Has major symptoms of anxiety, depression, etc. Is not at imminent risk of self-harm META:PHI 2015 MANAGEMENT OF COMMON PRESENTING PROBLEMS OF OPIOID USERS META:PHI 2015 Infections: Outpatient Treatment • Use oral antibiotics that cover staph and strep – Avoid PIC lines if possible • Ask about injection drug use and look for indicators • Offer bup/nx treatment and refer to RAAM clinic (using ED referral card) • If patient agrees to bup/nx treatment but is not in withdrawal, refer to WMS with instructions to send back to ED upon onset of withdrawal • Offer advice on overdose prevention and give naloxone if indicated META:PHI 2015 Infections: Inpatient Treatment • Ask for telephone or in-person consult from RAAM physician • Start bup/nx treatment ASAP • Avoid PIC line if possible • Refer to RAAM clinic on discharge META:PHI 2015 Musculoskeletal Injuries and Trauma • Most minor injuries (muscle strains, contusions, etc.) do not require opioids • Combination of acetaminophen and NSAIDs is at least as effective as opioids and much safer META:PHI 2015 Opioid Prescribing for Minor Injuries *Protocol for ALL patients (not just opioid users) • When opioids are indicated: Use IR low-dose opioids rather than high-dose CR formulations Codeine preparations are effective for acute pain Prescribe for no more than 3-5 days Do not prescribe fentanyl for acute pain Do not prescribe benzodiazepines along with opioids Warn patients not to drink heavily or take sedating drugs when taking opioids Warn patients not to drive for two to three hours after taking the opioid, for at least the first week META:PHI 2015 Patients Admitted with Trauma • Suspect opioid addiction if: Patient requests higher doses than normally required for their degree of injury Patient requests a specific opioid Patient demands dose immediately, uses all PRNs Patient has risk factors for addiction Patient was on a high opioid dose prior to admission META:PHI 2015 Inpatient trauma patient and OUD • If addiction is suspected yet opioids required: Avoid PCA pumps and high doses of short-acting parenteral opioids Total daily dose will probably be higher than usual Breakthrough doses should be 10-30% of total daily dose Contact patient’s family doctor for further information Ask for phone or in-person consult from RAAM physician Initiate bup/nx or methadone therapy if indicated Or refer to RAAM clinic on discharge META:PHI 2015 Chronic Non-Cancer Pain: Requests for Opioid Refills in the ED (1) • If you do not suspect an OUD: Ask the patient the date and dose of last script Contact the patient’s pharmacy If history is consistent and sounds legitimate, and you chose to write a script: write a note to the pharmacist: “Do not dispense if you receive an alert from NMS [Narcotic Monitoring System].” Inform the patient that this is a one-time-only prescription, and document this in the chart META:PHI 2015 Chronic Non-Cancer Pain: Requests for Opioid Refills in the ED (2) Prescribe no more than 3-5 days Send a record of the visit to the family physician Prescribe a reasonable daily dose that you are comfortable with No more than 120-200 mg MED regardless of patient’s usual dose Prescribe no more than one patch of fentanyl even if patient is prescribed more than that • If OUD is suspected: Don’t prescribe opioids META:PHI 2015 Morphine Equivalent Doses Opioid Equivalent oral dose Morphine 30 mg Hydromorphone 5 mg Oxycodone 20 mg Codeine 200 mg Fentanyl 25 ucg = 60-100 mg morphine META:PHI 2015 Drug Seeking by Patients with OUD • Patients with OUD sometimes use the ED as a source of opioids • Can be difficult to diagnose • Clinical features: Make aggressive demands for a specific opioid Not satisfied with non-opioid treatments Often return to the same ED with the same presenting complaint Often on high prescribed doses yet runs out early Has risk factors for addiction META:PHI 2015 Management of Suspected Drug Seeking • Contact the patient’s pharmacy • Do not prescribe opioids • Tell patient you suspect they may have an OUD, and prescribing opioids will increase their risk of overdose while worsening their pain and distress • Inform patient that addiction is a treatable condition • If the patient is in withdrawal, prescribe bup/nx • If patient is not yet in withdrawal, refer to WMS with instructions to return to the ED when in withdrawal • Refer them to the RAAM clinic META:PHI 2015 Case Scenario – Christie Part 1 Christie is a 35 year old woman with neck pain from a motor vehicle accident years ago. She is on Hydromorph Contin 12 mg tid and hydromorphone 8 mg 1-2 tabs qid PRN for breakthrough. She reports that her prescription ended and her family doctor is not available to refill the prescription. She says she has not had medication in two days and that she is in severe pain. META:PHI 2015 Question • How would you manage Christie’s request? – What further information would you want to gather? META:PHI 2015 Management Plan • Check patient’s chart to see if she has presented with similar requests previously • Call pharmacy and verify amount and date of last prescription • Call physician in case they are available to speak META:PHI 2015 Case Scenario – Christie Part 2 You call the pharmacy and they inform you that Christie received a prescription for 240 hydromorphone tabs and 90 Hydromorph Contin tabs 2 weeks ago. You calculate that she has run out 2 weeks early. You review the hospital chart and note that she has made four similar requests for hydromorphone in the last six months. META:PHI 2015 Question • What is your diagnosis • What is your management plan? META:PHI 2015 Management Plan Tell patient you suspect she is addicted to hydromorphone and she needs treatment. Tell patient you will not prescribe her hydromorphone or Hydromorph Contin but can offer bup/nx instead META:PHI 2015 Case Scenario – Christie Part 3 Christie is reluctant to try bup/nx, citing fears around: worsening pain if she stops her prescription opioids, switching from one addictive substance to another, and being unable to attend the pharmacy everyday. She wants to leave with her regular prescription. META:PHI 2015 Question • What would be your discharge plan for Christie? META:PHI 2015 Discharge Plan a) Do not prescribe hydromorphone as this is harming the patient b) Provide bup/nx in the ED (patient has been off hydromorphone for two days) c) Give a prescription for a few days until patient can be seen in the rapid access clinic d) Emphasize to the patient that stopping hydromorphone and starting bup/nx will improve her pain, mood and function e) Tell patient to discuss ‘carries’ and going to the pharmacy every day with the RAAM physician META:PHI 2015 Depression and Suicidal Ideation • Regardless of whether patient sees psychiatry or is admitted: Inform patient that opioid addiction treatment will likely rapidly improve their mood and functioning Initiate bup/nx treatment if patient goes into withdrawal in the ED or in hospital If patient agrees to bup/nx treatment but is not in withdrawal, send to WMS with instructions to send back to ED with onset of withdrawal On discharge, refer patient to RAAM clinic (give referral card) and community addiction treatment with a bridging script for bup/nx if started in the ED META:PHI 2015 Urgent Psychiatry Referral • Refer patient to psychiatry if patient: Has recently attempted suicide Refuses bup/nx treatment or remains severely depressed despite bup/nx treatment Has major risk factors for suicide (e.g., recent loss, has feasible suicide plan) META:PHI 2015 MANAGING PAIN IN ED PATIENTS ON METHADONE OR BUP/NX META:PHI 2015 Addressing Misconceptions about Pain Patients on Methadone or Bup/nx • Stable doses of methadone or bup/nx do not relieve acute pain Patients have developed tolerance to analgesic effects of methadone or bup/nx Often require higher opioid doses to overcome tolerance • Treating acute pain will not trigger a relapse • Patients on methadone or bup/nx who are in acute pain are rarely drug-seeking META:PHI 2015 Protocol for Acute Pain Management • Maintain patient on their usual dose of methadone or bup/nx • Prescribe standard non-opioid analgesia • Prescribe opioids if the patient’s pain condition warrants it • Start with usual dose for that pain condition • Titrate rapidly if that dose is inadequate META:PHI 2015 Discharge for Patients on Methadone or Bup/nx • Prescribe opioids as you would for other patients (generally no more than 3-5 days) • Have patient follow up with their methadone or bup/nx prescriber and family physician • Fax prescription to patient’s bup/nx or methadone pharmacy with the request “Dispense with bup/nx or methadone” META:PHI 2015 PATIENTS ADMITTED TO HOSPITAL ON METHADONE META:PHI 2015 On Admission • Only doctors with an exemption from the CPSO to prescribe methadone can write methadone orders for hospital inpatients • Hospitals should identify methadone prescribers on staff who can write these orders – Methadone is usually not initiated in hospital whereas bup/nx can be safely initiated META:PHI 2015 Protocol for Admitted Methadone Patients • Cancel patient’s methadone at outpatient pharmacy • Ask pharmacy for dates methadone was dispensed in the past week • Lower dose if 72 hours or more have elapsed since last dose • If pharmacy or prescriber cannot be reached, give small amount of methadone (e.g., 15 mg) • If patient about to be admitted and methadone not available: Prescribe oral controlled release morphine qid; initial daily dose should probably not exceed 45 mg qid (180 mg) Do not co-prescribe benzodiazepines Titrate daily to relieve withdrawal symptoms; hold if drowsy META:PHI 2015 Risk Factors for Methadone Toxicity in Hospitalized Patients • Prescribing benzodiazepines or atypical antipsychotics • Prescribing medications that inhibit methadone metabolism (e.g., quinolone antibiotics) • Hepatic failure • Renal failure • Respiratory impairment META:PHI 2015 Avoiding Methadone Toxicity • Avoid or use low doses of benzodiazepines and atypical antipsychotics • Closely monitor patient daily for signs of toxicity • Observe patient for slurred speech or ‘nodding off’ while engaged in conversation over several minutes • Monitor QT interval – High serum methadone concentration can cause QT prolongation META:PHI 2015 Management of Toxicity • If signs of toxicity, hold methadone until clear, then resume at a much lower dose • Discontinue sedating drugs • If rapidly developing hepatic, renal, or respiratory failure, reduce dose even if no obvious signs of toxicity META:PHI 2015 ICU Patients on Methadone • Intubated, obtunded patients will still go through severe withdrawal if their methadone is abruptly discontinued • Provide regular doses of hydromorphone, titrated to relieve agitation • When patient is awake and alert, methadone can be resumed (at a lower dose, via G tube) META:PHI 2015