Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
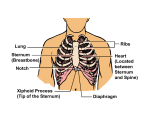
CODE BLUE MANAGEMENT ACLS CASES Part 4 Respiratory Arrest Management of respiratory arrest Giving supplementary oxygen Opening the airway Providing basic ventilation Using adjuncts suctioning Respiratory Arrest Critical concepts Avoid delivering excessive ventilations Increases intra thoracic pressure Decreases venous return to the heart ↓Carbon dioxide Causes gastric inflation Vomiting aspiration Respiratory Arrest Administering supplementary O2 Acute cardiac symptoms Respiratory distress Titrate to maintain ≥94% Respiratory Arrest Basic airway opening techniques Head tilt-chin lift Jaw thrust Respiratory Arrest Airway management OPA NPA Respiratory Arrest Providing basic ventilation Head tilt-chin lift Jaw thrust Mouth-to-mouth Mouth-to-nose Mouth-to-barrier Bag-mask Respiratory Arrest Suctioning Need suction force of -80 to -120 mmHg Soft vs. rigid catheters Catheter Use for Soft •Aspiration of thin secretions •Intra tracheal suctioning •Suctioning when NPA is in use Rigid Orophraynx Thick, particulate matter Respiratory Arrest Oropharyngeal suctioning Step 1 Action •Measure the catheter from tip of nose to earlobe •Gently insert into oropharynx beyond tongue 2 •Apply suction (occlude) while withdrawing with a rotating or twisting motion •If using a rigid device (Yankauer) place tip gently into oral cavity. Advance by pushing the tongue down to reach oropharynx Respiratory Arrest Endotracheal tube suctioning STEP ACTION 1 •Sterile technique 2 •Insert catheter (Do not occlude) 3 •Apply suction (occlude) while withdrawing with a rotating or twisting motion •DO NOT exceed 10 seconds •Precede and follow with 100% O2 Ventricular Fibrillation/Pulse less Ventricular Tachycardia Ventricular Fibrillation/Pulse less Ventricular Tachycardia What you will need Epinephrine Advanced airway Amiodarone Defibrillator Managing Ventricular Fibrillation/Pulse less Ventricular Tachycardia VF/VT (left side) Not recommend continued use of the AED when a manual defibrillator is available If you do not know the effective dose range, deliver the maximal energy Immediately after the shock, resume CPR Cont….. Safety during Defibrillation Be sure oxygen is not flowing across patient’s chest When shocking, the operator should face the patient, NOT the machine Cont…… Paddles vs Pads Reduces transthoracic impedance Equally effective Pads reduce arcing Allow for monitoring Recommended by the AHA Cont…… Rhythm Check After 2 minutes (5 cycles) Should not exceed 10 seconds Perform a pulse-check—preferably during rhythm analysis- only if an organized rhythm is present ASYSTOLE Give priority to Intravenous/Intraoseous access Search for underlying cause Do not stop CPR to administer drugs TCP not recommended Routine shock not recommended Asystole/PEA Asystole/PEA What you will need Epinephrine Defibrillator PEA Think of reversible causes (5 H & 5T’s) 5 H’s Hypovolemia Hypoxia Hydrogen ion (acidosis) excess Hypo/hyperkalemia Hypothermia Cont….. 5 T’s Toxins Tamponade, cardiac Thrombosis, coronary Thrombosis, pulmonary Tension pneumothorax Antiarrhytmics Amiodarone First-line antiarrhythmic agent in cardiac arrest Improves rate of ROSC ( return of spontaneous circulation) Lidocaine MgSO4 (Magnesium Sulphate) 1-2g (diluted in 10 mL D5W) bolus over 5 – 20 minutes For Torsade Cardiac Arrest Treatment Sequences Rhythm checks & shocks organized around 5 cycles (2 mins) Physiologic Monitoring During CPR AHA recommends using quantitative waveform capnography in intubated patients to monitor CPR quality End-Tidal CO2 Main determinant of PETCO2 during CPR is blood delivery to the lungs PETCO2 <10 mm Hg during CPR suggest ROSC unlikely. Improve chest compressions and vasopressor therapy If PETCO2 35-40, indicator of ROSC Cont….. Coronary Perfusion Pressure Measured by intra-arterial catheter <20 mm Hg, try to improve chest compressions and vasopressor therapy Monitoring CPR Quality Push hard (2 in) and fast ≥100/min Minimize interruptions Avoid excessive ventilation Rotate compressor every 2 minutes If no advanced airway, 30:2 Quantitative waveform capnography If PETCO2 <10 mmHg, attempt to improve CPR quality Intra-arterial pressure If diastolic <20 mmHg, attempt to improve CPR quality Routes of Access for Drugs IV Route Peripheral line preferred Central line access not necessary Drugs take 1-2 minutes to reach central circulation Give by bolus Follow with a 20mL bolus of IV fluid Elevate extremity for about 10-20 secs Routes of Access for Drugs Intraosseous route Preferred over the endotracheal route Endotracheal Route The optimal dose via this route is unknown Typical dose is 2-2 ½ times the IV route Dilute dose in 5 to 20 mL of H2O or saline Intraosseous route Adult Immediate Post-Cardiac Arrest Care Post-Cardiac Arrest Care Optimize ventilation and oxygenation Waveform capnography Use lowest FIO2 to maintain ≥94% (wean 100%) Begin ventilations at 10-12 bpm, titrate to PaCO2 of 40-45 mm Hg Avoid using ties that pass circumferentially around neck obstructs venous return from brain Post-Cardiac Arrest Care Foundational Facts: Recue breaths for CPR with an advanced airway During CPR, compression to ventilation ratio is 30:2 Once advanced airway is in place, compressions no longer interrupted Ventilating via advanced airway give 1 breath every 6 to 8 secs. (8-10 bpm) Post-Cardiac Arrest Care Most common and easily reversible causes of PEA Hypovolemia Hypoxia Assess, assess, assess for their presence Cardioversion Synchronized vs. unsynchronized Synchronized Unstable SVT Unstable atrial fibrillation Unstable atrial flutter Monomorphic tachycardia with pulses Cardioversion Energy doses for cardioversion Initial: 200 J (monophasic) 120-200 J (Biphasic) Atrial Flutter & SVT (50 to 100 J)