Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
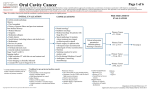
This practice algorithm has been specifically developed for MD Anderson using a multidisciplinary approach and taking into consideration circumstances particular to MD Anderson, including the following: MD Anderson’s specific patient population; MD Anderson’s services and structure; and MD Anderson’s clinical information. Moreover, this algorithm is not intended to replace the independent medical or professional judgment of physicians or other health care providers. This algorithm should not be used to treat pregnant women. NOTE: Consider clinical trials as treatment options for eligible patients. TREATMENT INITIAL EVALUATION Pathology consistent with small cell lung cancer ● History and physical ● Chest X-ray ● Laboratory studies to include: hematological and full chemistry panels ● CT chest and upper abdomen ● Pet and MRI or CT of the brain ● STAGE FURTHER WORKUP Solitary pulmonary nodule without lymphadenopathy? Brain imaging ● Bone scan or plain bone films if symptoms present that might require immediate radiotherapy ● Extensive Stage 2 1 Any test positive? Pulmonary function tests3 Yes No Positive Inoperable No Pulmonary function tests3, if clinically indicated Good performance status (Zubrod 0, 1 or 2)? No Are symptomatic brain metastases or cord compression present? No Limited disease: disease confined to the ipsilateral hemithorax within a single radiation port Extensive disease: disease beyond ipsilateral hemitorax or malignant pleural effudion or obvious metastatic disease 3 Pulmonary function tests include: spirometry pre-and-post-bronchodilators, xenon if clinically indicated, Exercise oxygen consumption testing if clinically indicated 4 Endobronchial ultrasound ● ● Yes No Platinum and etoposide For 4 cycles followed by Optional radiotherapy Radiotherapy and steroids, then Platinum and etoposide for 6 cycles Platinum and etoposide for 6 cycles Lymph nodes and/or margins positive Radiotherapy (45 Gy twice a day or 60-70 Gy daily or twice a day) concurrent with platinum and etoposide for 4 cycles Yes Yes Resection Mediastinoscopy or EBUS4 Yes ● Brain Limited Stage 1 imaging ● Bone scan ● Bone marrow aspiration and biopsy if LDH elevated or abnormal CBC Is patient potentially operable? Operable Negative Partial or complete response? Lymph nodes and margins negative Adjuvant platinum and etoposide for 4 cycles Prophylactic cranial irradiation (PCI). Use total dose of: 25 Gy in 10 fractions Surveillance (see page 2) Yes Consider: ● Prophylactic cranial irradiation (PCI) of 25 Gy in 10 fractions, and ● Chest radiotherapy of 45 Gy in 15 fractions 2 Copyright 2015 The University of Texas MD Anderson Cancer Center No Department of Clinical Effectiveness V8 Department of Clinical Approved by The Executive Committee of the Medical Staff Effectiveness on 03/31/2015V8 Approved by The Executive Committee of the Medical Staff on 03/31/2015 This practice algorithm has been specifically developed for MD Anderson using a multidisciplinary approach and taking into consideration circumstances particular to MD Anderson, including the following: MD Anderson’s specific patient population; MD Anderson’s services and structure; and MD Anderson’s clinical information. Moreover, this algorithm is not intended to replace the independent medical or professional judgment of physicians or other health care providers. This algorithm should not be used to treat pregnant women. NOTE: Consider clinical trials as treatment options for eligible patients. SALVAGE / PALLIATION SURVEILLANCE Reinduction therapy with platinum and etoposide ● Palliative symptom management including localized radiotherapy ● Greater than 3 months from completion of treatment History, physical, chest X-ray and scans of involved sites every 2 – 3 months for 2 years, then every 6 months for 3 years, then yearly Yes Time of relapse? Relapse? No Continue surveillance Copyright 2015 The University of Texas MD Anderson Cancer Center Less than or equal to 3 months from completion of treatment Salvage chemotherapy (see principles of chemotherapy) ● Palliative symptom management including localized radiotherapy ● Department of Clinical Effectiveness V8 Department of Clinical Approved by The Executive Committee of the Medical Staff Effectiveness on 03/31/2015V8 Approved by The Executive Committee of the Medical Staff on 03/31/2015 This practice algorithm has been specifically developed for MD Anderson using a multidisciplinary approach and taking into consideration circumstances particular to MD Anderson, including the following: MD Anderson’s specific patient population; MD Anderson’s services and structure; and MD Anderson’s clinical information. Moreover, this algorithm is not intended to replace the independent medical or professional judgment of physicians or other health care providers. This algorithm should not be used to treat pregnant women. NOTE: Consider clinical trials as treatment options for eligible patients. PRINCIPLES OF CHEMOTHERAPY First-Line Chemotherapy Acceptable regimens for Limited Stage disease include: ● Cisplatin: 60 mg/m2 day 1 plus Etoposide: 120 mg/m2 days 1, 2, 3 every 21 days for 4 cycles; cycles 1 and 2 should be given concurrent with chest XRT. ● Carboplatin: AUC 6 day 1 plus Etoposide: 100 mg/m2 days 1, 2, 3 every 21 days for 4 cycles is an acceptable alternative regimen in patients unable to receive cisplatin; cycles 1 and 2 should be given concurrent with chest XRT. ● Acceptable regimens for Extensive Stage disease include: ● Cisplatin: 60 mg/m2 day 1 plus Etoposide: 100 mg/m2 days 1, 2, 3 every 21 days for 6 cycles ● Carboplatin: AUC 6 day 1 plus Etoposide: 100 mg/m2 days 1, 2, 3 every 21 days for 6 cycles ● Irinotecan: 60 mg/m2 on days 1, 8, 15 plus Cisplatin: 60 mg/m2 on day 1, each cycle 28 days ● Second-Line Chemotherapy If relapse occurs greater than 3 months after completion of first-line therapy, re-treat with original regimen ● If relapse occurs less than 3 months after completion of first-line therapy, acceptable second-line chemotherapy option include topotecan, irinotecan, VAC (vincristine plus doxorubicin plus cyclophosphamide) or oral etoposide ● Copyright 2015 The University of Texas MD Anderson Cancer Center Department of Clinical Effectiveness V8 Department of Clinical Approved by The Executive Committee of the Medical Staff Effectiveness on 03/31/2015V8 Approved by The Executive Committee of the Medical Staff on 03/31/2015 This practice algorithm has been specifically developed for MD Anderson using a multidisciplinary approach and taking into consideration circumstances particular to MD Anderson, including the following: MD Anderson’s specific patient population; MD Anderson’s services and structure; and MD Anderson’s clinical information. Moreover, this algorithm is not intended to replace the independent medical or professional judgment of physicians or other health care providers. This algorithm should not be used to treat pregnant women. NOTE: Consider clinical trials as treatment options for eligible patients. PRINCIPLES OF RADIATION THERAPY Radiotherapy For Limited Stage Disease ● Radiotherapy should be given 1.5 Gy bid (with at least 6 hours between fractions), to a total dose of 45 Gy. In circumstances where bid fractionation is not feasible, an acceptable alternate schedule is 1.8 – 2.0 Gy/day to a dose of 60 – 70 Gy. ● XRT should be administered concurrent with chemotherapy, ideally beginning during cycle 1 of chemotherapy. ● XRT should be delivered to original tumor volume unless there is marked risk of radiation pneumonitis; then decrease field as tumor shrinks. ● Appropriate schedule for prophylactic cranial irradiation (PCI) 25 Gy in 10 fractions. ● In patients receiving radiation therapy or chemoradiation with curative intent, treatment interruptions or dose reductions for temporary and manageable toxicities, such as esophagitis and myelosuppression, should be avoided. Careful patient monitoring and aggressive supportive care are preferable to treatment breaks in potentially curable patients. Patients should be evaluated at least once per every 5 fractions to monitor weight changes and toxicity. ● 45 Gy in 30 Fractions over 3 weeks would not be recommended with concurrent chemotherapy on day 1, if the DVH shows V20 more than 35% of TL. If the GTV is too large to meet Dose Volume constraints, give one cycle of chemo or go daily fraction of radiation and cone down of the GTV after resimulation after 2-3 weeks treatment. This will apply for the patients who have FEV1 or DCLO less than 30% of predicted value. ● Elective nodal RT is not recommended. Copyright 2015 The University of Texas MD Anderson Cancer Center Department of Clinical Effectiveness V8 Department of Clinical Approved by The Executive Committee of the Medical Staff Effectiveness on 03/31/2015V8 Approved by The Executive Committee of the Medical Staff on 03/31/2015 This practice algorithm has been specifically developed for MD Anderson using a multidisciplinary approach and taking into consideration circumstances particular to MD Anderson, including the following: MD Anderson’s specific patient population; MD Anderson’s services and structure; and MD Anderson’s clinical information. Moreover, this algorithm is not intended to replace the independent medical or professional judgment of physicians or other health care providers. This algorithm should not be used to treat pregnant women. NOTE: Consider clinical trials as treatment options for eligible patients. SUGGESTED READINGS Auperin A, Arriagada R, Pignon JP et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. N Engl J Med 1999;341:476 – 484 (Editoral: Carney DN. Prophylactic cranial irradiation and small-cell lung cancer. N Engl J Med 1999; 341:524 – 526). Chute JP, Chen T, Feigal E, et al. Twenty years of phase III trials for patients with extensive small cell lung cancer: perceptible progress. J Clin Oncol 1999;17:1794 – 1801. Komaki R, Swann RS, Ettinger DS, et al. Phase I study of thoracic radiation dose escalation with concurrent chemotherapy for patients with limited small-cell lung cancer: Report of Radiation Therapy Oncology Group (RTOG) protocol 97-12. Int J Radiat Oncol Biol Phys. 2005;62:342-50. Murray N, Coy P, Pater JL, et al: Importance of timing for thoracic irradiation in the combined modality treatment of limited-stage small-cell lung cancer. The National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 1993;11:336-44. Pechoux CL, Dunant A, Senan S, Wolfson A, Quoix E, Finn CF, Ciuleanu T, Arriagada R, Jones R, Wanders R, Lerouge D, Laplanche, A. Standard-dose versus higher-dose prophylactic cranial. Lancet 2009;10:467-74, 4/2009. Pignon JP, Arriagada R, Ihde DC, et al. A meta-analysis of thoracic radiotherapy for small-cell lung cancer. N Engl J Med 1992; 327:1618-1624. Slotman B, Tinteren H, Praag J, Knegjens J, Sharouni S, Hatton M, Keijser A, Faivre-Finn C, Senan S. Use of thoracic radiotherapy for extensive state small-cell lung cancer: a phase 3 randomised controlled trial. Lancet 2014; 10.1016/S0140-6736(14)61085-0. Spira A and Ettinger DS. Multidisciplinary management of lung cancer. N Engl J Med 2004;350:379 – 392. Tucker MA, Murray N, Shaw EG, et al. Second primary cancers related to smoking and treatment of small cell lung cancer. J Natl Cancer Inst 1997;89:1782 – 1788 (Editorial: Glisson BS, Hong WK. Survival after treatment of small cell lung cancer: an endless uphill battle. J Natl Cancer Inst 1997;89:1745 – 1747). Turrisi AT, Kim K, Blum R, et al. Twice daily compared with once daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N Engl J Med 1999;340:265 – 271. Copyright 2015 The University of Texas MD Anderson Cancer Center Department of Clinical Effectiveness V8 Department of Clinical Approved by The Executive Committee of the Medical Staff Effectiveness on 03/31/2015V8 Approved by The Executive Committee of the Medical Staff on 03/31/2015 This practice algorithm has been specifically developed for MD Anderson using a multidisciplinary approach and taking into consideration circumstances particular to MD Anderson, including the following: MD Anderson’s specific patient population; MD Anderson’s services and structure; and MD Anderson’s clinical information. Moreover, this algorithm is not intended to replace the independent medical or professional judgment of physicians or other health care providers. This algorithm should not be used to treat pregnant women. NOTE: Consider clinical trials as treatment options for eligible patients. DEVELOPMENT CREDITS This practice guideline is based on majority expert opinion of the Thoracic Oncology Center Faculty at the University of Texas, M D Anderson Cancer Center. It was developed using a multidisciplinary approach that included input from the following medical, radiation and surgical oncologists: Lauren A. Byers, MD George R Blumenschein, Jr, MD Joe Y Chang, MD, PhD Ŧ Frank V. Fossella, MDŦ Daniel Gomez, MD Bonnie S Glisson, MD John V Heymach, MD, PhD Wayne Hofstetter, MD Melenda Jeter, MD, MPH Merrill S Kies, MD Ritsuko Komaki, M.D. Jonathan M Kurie, MD Zhongxing Liao, MD Charles Lu, MD, SM Reza Mehran, MD Vassiliki A Papadimitrakopoulou, MD Makala B Pace, RPH Katherine M Pisters, MD David Rice, MD Jack A Roth, MD Stephen Swisher, MD Anne Tsao, MD Ara Vaporciyan, MD Garrett Walsh, MD James Welsh, MD William N William Jr, MD Ŧ Core Development Team Copyright 2015 The University of Texas MD Anderson Cancer Center Department of Clinical Effectiveness V8 Department of Clinical Approved by The Executive Committee of the Medical Staff Effectiveness on 03/31/2015V8 Approved by The Executive Committee of the Medical Staff on 03/31/2015