Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
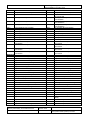
Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Screening, Testing and Immunisation for Blood Borne Viral Hepatitis in Primary Care Quality Improvement Toolkit Author: Primary Care Quality and Information Service Date: November 2009 Version: Final Version 1 Status: Final Intended Audience: Public (internet) / NHS Wales (Intranet) / NPHS (Intranet) This document is for use by general practices who are engaged in screening, testing and immunisation for Blood Borne Viral Hepatitis in Primary Care. The purpose of this quality improvement toolkit is to support practices to review and improve where necessary, the recording of information available when providing this service to their patients. The audit toolkit will provide the user with a summary of the evidence associated with screening, testing and immunisation for Blood Borne Viral Hepatitis in Primary Care. Also included is a practice review section designed to encourage a whole practice response to the audit findings and an evaluation of the quality and usefulness of the audit itself. Publication / distribution: Publication in NPHS document database (Primary Care Quality and Information) Link from NPHS e-bulletin Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 1 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Preface Quality Improvement Toolkits The Primary Care Quality and Information Service (PCQIS) has developed quality improvement toolkits to assist practices in collating and auditing information. These are produced with reference to evidence based practice and Welsh priorities. They should be seen as good practice. They cover areas that some or even all practices may not be recording at this stage. It is not expected that all the criteria within the audits will be achieved in year one. The PCQIS suggests that the toolkits be used to improve data quality and aid development within the practice. Improvements in practice will be optimised by multidisciplinary involvement in the audit and team discussion of the results. We recommend that action plans following audits are reviewed within 6 months and re-audit undertaken if possible in 6-12 months. You can access other quality improvement toolkits that support Enhanced Services and National Service Frameworks from the Public Health Wales (PHW) website: Intranet http://nww2.nphs.wales.nhs.uk/page.cfm?pid=33294 Internet http://www.wales.nhs.uk/sites3/page.cfm?orgid=719&pid=25575 Approved READ Codes (in Version 2 and Clinical Terms Version 3) have been developed to support practices wishing to build searches and extract the data from their clinical system. If you have any queries regarding this document please contact: Laura Beer, Team Lead – PCQIS Tel: 01792 607311 Email: [email protected] Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 2 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Contents Page Introduction 4 Aims 5 Background 5 Method 7 Data Collection 8 Evidence 9 References 13 Practice review 15 Evaluation form 16 Appendix A – Recommended tests 17 Appendix B – READ codes 18 Appendix C – Patient leaflets 21 Abbreviations Anti-HCV Anti-HBc Anti-HBS ICDS BBV HBV HCV IDUs MSM PHLS PHCT LFTs NICE Antibodies to hepatitis C virus Antibody hepatitis B core antigen Hepatitis B antibodies Infection and Communicable Disease Service Blood borne virus (e.g. HBV, HCV and HIV) Hepatitis B virus Hepatitis C virus Injecting drug users Men who have sex with men Public Health Laboratory Service Primary Health Care Team Liver Function Tests National Institute of Health and Clinical Excellence Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 3 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Definition of a user of drugs of dependence For the purpose of this toolkit, a user of any drugs of dependence is defined as a person who misuses substances such as heroin, crack cocaine, amphetamines, marijuana, opiates and benzodiazepines. Definitions of Screening and Testing For the purpose of this toolkit screening is the process of assessing the risk factors associated with the acquiring of a blood borne virus. Testing is the undertaking of a blood test or dry spot test to detect the presence or absence of a blood borne virus. However, it should be noted that many documents and clinical guidance use the terms interchangeably. Introduction In January 2008, the Welsh Assembly Government published ‘Working Together to Reduce Harm’, a 10 year strategy which aims to set out a clear national agenda to tackle and reduce the harms associated with substance misuse in Wales.1 The strategy describes the requirement of primary care in applying best practice, to prevent and control the hepatitis B virus (HBV) in injecting drug users (IDUs). Key Performance Indicator 18 states that “all clients who are IDUs to be offered information, counselling, screening, and where appropriate, immunisation against hepatitis B”.1 Published in March 2009, the Welsh Assembly Government Blood Borne Viral Hepatitis Action Plan for Wales consultation document 2 states that: Transmission of blood borne viruses (BBV) can be prevented, yet in Wales transmission is common amongst high risk groups. HBV infection is preventable with an effective vaccine With modern therapy, depending on the genotype of hepatitis C virus (HCV) infection, between 40% - 85% of patients with chronic HCV can be cleared of the virus. The treatment is cost effective and has been recommended by the National Institute of Health and Clinical Excellence (NICE) in a technology appraisal. 3 Treatment for chronic HBV infection has been recommended by NICE in a technology appraisal.4 Less than 2000 people are currently being monitored or treated for hepatitis C by specialist services across Wales. Failure to improve uptake of treatment will lead to an increase in liver disease and the number of untimely deaths in Wales. The action plan states that an effective response must prevent transmission diagnose infection in people who have the virus in their blood treat disease in those with chronic infection and recommends that within Primary Care, Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 4 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care high quality shared care provision of substitute drug treatment is provided uptake of testing for blood borne viruses is improved - targeting those on their patient lists who are most at risk delivery of the antenatal screening programme for hepatitis B is supported hepatitis B vaccination is provided to all high risk groups in primary care contribution to the care pathway providing community based support to those affected is increased Currently within Wales and England only acute hepatitis B infection (HBV) is recorded so no estimates exist for chronic infection of HBV within Wales.2 The number of people infected with HBV and HCV increases each year because of continued high risk behaviour. 2 Aims The aim of this toolkit and audit is to address some of the issues for primary care raised in the above publications and help to increase the number of all high risk groups receiving screening, testing, and immunisation for blood borne viral hepatitis by: identifying all high risk groups in General Practice. raising awareness through offering information and counselling. offering testing and immunisation against hepatitis B, and offering referral for screening/testing for hepatitis C, to those in the relevant high risk groups. providing recommended READ codes to enable information relating to patients who are at high risk to be consistently recorded on GP practice systems. Background Hepatitis B Hepatitis B is a viral infection that is spread through the blood, and semen, saliva and vaginal fluid of an infected person and by perinatal transmission from mother to child. The incubation period ranges from 40-160 days and causes inflammation of the liver (hepatitis) which may lead to long term liver damage.5,20,7 In the UK, hepatitis B infection is usually acquired in adulthood, with sexual activity or injecting drug use being the most commonly reported routes of infection. Infection with hepatitis B, is however preventable using a widely available, safe and effective vaccine.6 Hepatitis B vaccine is a killed preparation of the purified major surface antigen of the virus manufactured by recombinant DNA technology, adsorbed onto aluminium hydroxide. It is highly effective and has an excellent safety record.20 The Immunisation Against Infectious Disease: The Green Book, states that HBV immunisation is recommended for the following individuals and groups:-7 All IDUs as a high priority (including those who inject intermittently) Those who are likely to “progress” to injecting, for example those who are currently smoking heroin and/or crack cocaine, and heavily dependent amphetamine users Non-injecting drug users who are living with current injectors Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 5 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Sexual partners of injecting users Children of injectors Men who have sex with men (MSM) Sex workers Those who change sexual partner frequently Close family contacts of a case or individuals with chronic HBV infection Families adopting children from countries with high or intermediate HBV prevalence Foster carers Individuals receiving regular blood or blood products and their carers Patients with chronic renal failure or chronic liver disease Individuals in residential accommodation for those with learning difficulties Travellers to areas of high or intermediate prevalence, Individuals at occupational risk.7 In 2005, the NPHS carried out a survey on General Practitioners who provided hepatitis B immunisation. It was found that 66.4% of GPs across Wales provided hepatitis B immunisation for IDUs.8 Hepatitis C Hepatitis C is transmitted through blood-to-blood contact. In the UK, sharing of needles and paraphernalia when injecting drugs is the most common way to acquire hepatitis C (only rarely is it passed on through other body fluids e.g. during sex). The HCV causes inflammation of the liver (hepatitis) and may also cause long term liver damage. In relation to other areas in the UK, Wales currently has lower levels of hepatitis B, hepatitis C and HIV in IDU populations. However, in the larger cities in Wales and particularly amongst homeless drug misusers, hepatitis C is common.1 Higher risk injecting practices e.g. multiple drug injecting, injecting heroin with crack/cocaine (speedballing) increase the risk of infection and associated harms.1 Evidence from NPHS is that in Wales there are an estimated 12,000 individuals, (0.4% of the population) with chronic hepatitis C.9 If left untreated, hepatitis C can cause serious liver disease in some patients, including cirrhosis and liver cancer. 92% of reports of hepatitis C infection to the PHLS, in which risk factors were reported, related to either current or previous drug use.10 Contaminated blood or blood products accounted for a further 2.5% of reported infections. Other people may have become infected with hepatitis C through non-sterile medical or dental procedures; non-sterile tattooing, body-piercing or other skin-incision procedures; other forms of blood-to-blood contact. There is around a 6% risk of transmission from mother to child before or during birth if the mother has chronic hepatitis C and detectable viraemia.9 There is no vaccine to protect against hepatitis C. The NPHS, state that as the virus may be transmitted by contact with blood from an infected person, certain people may be at a higher risk of acquiring hepatitis C. These include people who: 10,21,22 Have unexplained abnormal liver function tests (e.g. elevated ALT), or unexplained jaundice Have ever injected drugs, even if it was only once or twice, or many years ago Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 6 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Have had a blood transfusion (before September 1991) or blood products (before 1986 in the UK) Are children of a mother with hepatitis C. (The test result may be difficult to interpret in children under 18 months, due to the presence of material antibodies and specialist virological advice will be needed) Are regular sexual partners of someone with hepatitis C. Have had medical or dental procedures abroad, in countries where infection control may be poor Have been accidentally exposed to blood where there is risk of hepatitis C infection Have had an ear piercing, a body piercing, tattoo, acupuncture or electrolysis with unsterile equipment (although not stated in the website those with prison tattoos). Have previously been diagnosed with non-A, non-B hepatitis and not subsequently tested for hepatitis C. Are drug users, whether smoking or injecting drugs, who have ever shared any drug paraphernalia. Have received medical treatment or blood products in a country where hepatitis is common Were born in a country where hepatitis c is common. Come into contact with blood products i.e. healthcare workers, prison officers Method It is recommended that Practices complete the Data Collection Sheet provided. This sets out the criteria taken from evidence based sources. Practices should agree a data collection period prospectively and members of the Primary Healthcare Team (PHCT) should be involved in the identification of patients. Practices should use the audit results as the basis of a discussion by the PHCT. The Practice review form can be used to reflect on findings and changes needed to ensure quality improvement. It is suggested that Practices re-audit annually to ensure that any changes implemented are having a positive effect on patient care. Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 7 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Data Collection Sheet Screening, Testing, Immunisation for blood borne viral hepatitis amongst high risk groups in primary care Number A Number of patients in at risk groups for hepatitis B Some READ Codes for patients in the “Risk Groups” can be found in Appendix B (page 18), however, NHS Connecting for Health have been contacted to request new READ Codes on the italic bulleted lists on pages 5,6,7. New READ codes are released quarterly, updates are available on the Connecting For Health website http://www.connectingforhealth.nhs.uk/systemsandservices/data/readcodes/changestocurrentrelease B Number of patients in A offered a test for hepatitis B (Please note the evidence on page 9 – opportunistic immunisation of those unlikely to re-attend is recommended and lack of certainty of immunisation status should not act as a barrier to immunisation) READ V2 65W5. Requires a course of hepatitis B 65WC. Hepatitis B immunisation recommended CTV3 65W5. Requires a course of hepatitis B XaMe9 Hepatitis B immunisation recommended C Number of patients in at risk groups for hepatitis C. Some READ Codes for patients in the “Risk Groups” can be found in Appendix B (page 18), however, NHS Connecting for Health have been contacted to request new READ Codes on the italic bulleted lists on pages 5,6,7. New READ codes are released quarterly, updates are available on the Connecting For Health website http://www.connectingforhealth.nhs.uk/systemsandservices/data/readcodes/changestocurrentrelease D Number of patients in C offered a test for hepatitis C (Please see note under B above) E Of those in A - Number who have received 1 dose of hepatitis B immunisation READ V2 14b0. History of one hepatitis B immunisation 65F1. 1st hepatitis B immunisation 65MD. First combined hepatitis A & B vacc. CTV3 XaN0g History of one hepatitis B immunisation. 65F1. 1 st hepatitis B immunisation 65MD. First combined hepatitis A & B vacc. F Of those in A - Number who have received 2 doses of hepatitis B immunisation READ V2 65F2. 2nd hepatitis B immunisation 65ME. Second combined hepatitis A & B vacc. CTV3 65F2. 2nd hepatitis B immunisation 65ME. Second combined hepatitis A & B vacc G Of those in A - Number who have received 3 doses of hepatitis B immunisation READ V2 65F3. 3rd hepatitis B immunisation 65MF. Third combined hepatitis A & B vacc. Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 CTV3 65F3. 3rd hepatitis B immunisation 65MF. Third combined hepatitis A & B vacc. Date October 2009 8 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS % Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Evidence to support the screening, testing immunisation for blood borne viral hepatitis amongst high risk groups within primary care Hepatitis B Promoting immunisation uptake A pragmatic approach to an immunisation schedule is recommended. This involves providing current users of any drugs of dependence with both the means and opportunity to significantly reduce the risks associated with injecting. Drug misusers whether injecting or not, should be encouraged to access relevant advice and information or counselling which includes strategies for avoiding exposure to blood-borne virus infection and contamination.11 Strategies to help identify other groups at risk of hepatitis B should also be taken. This would include highlighting the risks for those travelling to high risk areas, occupational risk etc. Prominent display of posters and use of leaflets promoting hepatitis B immunisation may be helpful. Promotion of immunisation is dependent on motivated knowledgeable staff.12 Testing for hepatitis B Testing for HBV serves the dual purpose of identifying those who are currently infected, and those who are immune by natural infection (and by eliminating those who are still susceptible and should be immunised).15 Diagnostic tests for HBV are recommended in anyone presenting with suspected acute hepatitis and in those with symptoms or signs of chronic liver disease, or abnormal LFTs consistent with acute or chronic hepatitis. 13 However, poor patient attendance for testing is often reported as a major barrier to immunisation. To address this, current expert advice is to focus on protection through immunisation rather than testing.12 Immunisation should be offered and administered opportunistically perhaps at the time when the 'at risk' individual makes initial contact with the practice. Delaying immunisation can do harm because a drug misuser may become infected before the next visit or may not return.21 Lack of certainty of immunisation status should not act as a barrier to immunisation and reliance on recall of history of immunisation is not advised. 12 Keeping records Information on hepatitis B vaccine uptake and completion is however useful and may assist in assessing the quality of a service and help teams to plan achievable improvements. A full record of immunisations given should be kept on the GP practice system, using recommended READ codes. Evidence recommends that recording systems between GPs and specialist clinics including those in prisons are developed and strengthened to ensure that where possible the full course of hepatitis B vaccine is administered to all relevant patients. 11, 12, 14 Sexual and Other Contacts The partners and children of drug misusers are also at risk of hepatitis B infection, but their need for immunisation is often overlooked. Hepatitis B can be transmitted through sexual contact and non-sexual intimate contact.12 Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 9 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Sexual partners, close household contacts, and children of users of any drugs of dependence are at risk of hepatitis B infection and it is recommended that these should be immunised. Children infected with hepatitis B have a higher risk of chronic infection than adults.7, 12 Organising immunisation for families may not be straightforward. Families may not be registered in the same practice as the drug misuser. Some drug misusers may be reluctant to disclose the risk to their partners. Health care workers need to work with drug misusers to advise them of the risks and promote the routine offering of immunisation to partners and children.12 Testing to identify those with current or past infection should be undertaken at the same time as immunisation and should not delay immunisation.12 Hepatitis B Immunisation Schedule There are 3 recommended schedules for hepatitis B immunisation. Conventional – immunisation given at zero, one and six months can be used for pre-exposure prophylaxis where rapid protection is not required and there is a high likelihood of compliance.7 Accelerated - An accelerated schedule is recommended for pre-exposure prophylaxis for adults and children in at risk groups. Immunisation is given at zero, one and two months with a fourth dose after 12 months. This schedule is recognised as the most appropriate for users of any drugs of dependence.7 Higher completion rates for three doses at zero, one and two months have been reported. Improved compliance is likely to offset the slightly reduced immunogenicity when compared with the zero, one and six months schedule, and similar response rates can be achieved by opportunistic use of a fourth dose after 12 months.7 Rapid - A primary immunisation schedule is also licensed for adults (Engerix B only), three doses given at zero, seven and twenty one days with a fourth dose 12 months after the first. This schedule is licensed for use in circumstances where adults over 18 years of age are at immediate risk and where a more rapid induction of protection is required. In teenagers under 18 years of age, response to vaccine is as good as or better than in older adults. Although not licensed for this group, this schedule can be used in those aged 16 – 18 where it is important to provide rapid protection and to maximise compliance.7 Even incomplete immunisation schedules offer some protection. ensure that there is a robust system for re-call.12 In addition services need to Immunisation Schedules for hepatitis B using monovalent vaccine or combined A+B vaccine. 15 Immunisation Schedule 0, 7, 21 days, 12 months Advantages - Rapid immunity, - Short duration, - High antibody titres at 12 and 13 months - Better uptake Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 10 Disadvantages - Less information on HIV or other immune-compromised patients - Low antibody titres in 1st year (but current evidence suggests that protection is still adequate in the immune-competent) - Not licensed for under 18s Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales 0, 1, 2, 12 months 0, 1, 6 months Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care - Shorter time to early immunity than the 0, 1, 6 course - High antibody titres at 12 and 13 months - Higher antibody titres at 7 months than the other two regimens although this may not be clinically important - Long established regimen - Most researched in HIV - Antibody titres lower than the 0, 1, 6 regimen in the first year - Poor uptake of the 6 month dose in the clinical setting Pre and /or post-immunisation testing for hepatitis B antibodies (anti-HBs), is not generally recommended (please see ‘Testing for hepatitis B’ on page 9 of this toolkit). It is however essential in certain occupational groups, and babies who are born to hepatitis B positive mothers would require both anti-HBs and HBsAg. Practices should follow the guidance issued by Public Health Wales23 and the Green Book 7 for advice on scheduling for babies and children and the use of combined HAV/HBV vaccines. When previous history is not available, individuals should be assumed to be unimmunised and a full course of immunisation planned.7, 16 For those babies and children (up to the age of 18 years) who are administered hepatitis B immunisation, notification must be sent to the Child Health Department via an unscheduled form as soon after the vaccine is given as possible so the central recording system has a full, accurate record of the vaccines given. 23 Hepatitis C Screening for hepatitis C Screening for HCV infection is the offer of a test in people not complaining of symptoms associated with HCV or requesting a test of HCV status. Screening for HCV is currently undertaken in a range of groups and settings, and supported by several consensus statements internationally and NHS Policy with respect to screening in IDUs.17 Health Technology Assessment 2002; Vol 6: No 31 states that “while selective screening may be more cost-effective and affordable than universal screening, we believe that it remains open to question whether seeking people other than IDUs for screening represents a cost effective use of NHS resources”.17 Health Technology Assessment 2006; Vol 10: No 32 concluded that case-finding for hepatitis C is likely to be considered cost-effective by NHS commissioners. Improvements in the effectiveness of treatments to slow or halt disease progression are likely to improve the cost-effectiveness of case finding. Case finding is likely to be most cost-effective if targeted at people whose HCV disease is more advanced. 3 Drug Misuse There are estimated to be around 8,000 current IDUs in Wales – around 0.4% of the adult population in Wales.1 The health service cost in Wales of problem drug use has been estimated at £17.6 million per year.18 Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 11 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care The prevalence of blood borne virus infection amongst drug injectors To address the epidemiology of blood borne viral transmission in Wales, a large multi-centre incidence study was carried out between 2004 and 2006. This study, the largest of its kind in Wales, has produced up to date evidence of the prevalence and incidence of HCV, HBV amongst IDUs in Wales. The study found prevalence rates of antibodies to hepatitis C virus (anti-HCV) 26% and antibody hepatitis B core antigen (anti-HBc) - 9%. 7% had markers of exposure to both HCV and HBV. There were marked regional differences in prevalence for example, in Cardiff anti-HCV prevalence was 35% and anti-HBc was 18%, whilst in Merthyr Tydfil respective prevalences were 10% and 0%.14 Incidence rates of 6 per “100 person years” 14 for hepatitis C were found. This means that in a year, between 3 and 9 in every 100 injectors will become infected with hepatitis C. Incidence rates of 2 per “100 person years” for hepatitis B were found. This means that within the injecting drug user population, in a year between 1 and 4 will become infected with hepatitis B. These figures are not static and may rise due to the year on year increase in those infected and potentially passing on the virus to others.14 Initial analysis of incidence data suggests that the incidence of HCV is at least as great amongst recent initiates to injecting as amongst long term injectors.14 The prevalence of infection was greatest among those who had long injecting careers, however, an anti-HCV prevalence of 5% was found in those, usually young people, who had been injecting for one year or less.14 Only one quarter of those individuals who tested anti-HCV positive were already aware of their status, the remaining three quarters (over 135 individuals) were unaware of their status.14 Of serious concern was the lack of awareness of hepatitis C and hepatitis B transmission routes and the implications for health among this population despite contact with substance misuse services.14 Needle Exchange Services Needle exchange provision is fundamental in the prevention of blood borne viral transmission in Wales. Work undertaken by the Infection and Communicable Disease Service (ICDS) states that the provision of clean needles and syringes across Wales is varied and at times problematic. Furthermore, barriers exist in the ability of individual injectors to access services. A greater understanding of both these barriers and of current provision is needed.14 The services provided must include needle exchange, harm minimisation advice, blood-borne virus testing and immunisation for hepatitis B. Access to these must be easy and convenient and include better provision via outreach services.19 Working Together to Reduce Harm states that commissioners should engage with providers to ensure additional venues are available for the provision of sterile injecting equipment, such as mobile facilities, and the need to expand outreach teams, including those aimed at rough sleepers.1 Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 12 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care References 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 WAG. Working Together to Reduce Harm. The Substance Misuse Strategy for Wales 2008-2018. WAG January 2008. WAG. Proposed Blood Borne Viral hepatitis Action Plan for Wales 2009-2014. WAG March 2009. Castelnuovo E, Thompson-Coon J, Pitt M et al. The cost-effectiveness of testing for hepatitis C in former injecting drug users. Health Technology Assessment 2006; Volume 10: No. 32. Accessed 05/03/2009. National Institute for Health and Clinical Excellence. Adefovir dipivoxil and peginterferon alfa-2a for the treatment of chronic hepatitis B. London: NIHCE; (2006b) http://www.nice.org.uk/nicemedia/pdf/TA096guidance.pdf. Accessed 29/03/2009. NPHS. Hepatitis B. Available from Health Protection web page. http://howis.wales.nhs.uk/sites3/home.cfm?orgid=457 . Accessed 29/03/2009 (intranet only) Health Protection Agency, Health Protection Scotland, National Public Health Service for Wales, CDSC Northern Ireland and CRDHB. Shooting Up: Infections among injecting drug users in the United Kingdom 2006. London: Health Protection Agency, 2007 Salisbury D, Ramsay M, Noakes K. Immunisation against infectious disease. The Green Book. Chapter 18 Hepatitis B. London: The Stationery Office; 2006. NPHS. Report 9 – Primary Care Services for blood borne viral hepatitis prevention, treatment and care. October 2006. NPHS. Secondary and Tertiary Service Provision for Chronic Hepatitis C across Wales. October 2006. NPHS. Hepatitis C web pages. (intranet only) http://howis.wales.nhs.uk/sites3/page.cfm?orgId=719&pid=20099 Accessed 21/04/2009. National Treatment Agency for Substance Misuse. Drug Misuse and dependence UK guidelines on clinical management. 2007. http://www.nta.nhs.uk/areas/Clinical_guidance/clinical_guidelines/docs/clinical_guidelines_ 2007.pdf. Accessed 20/11/2008. Substance Misuse Management in General Practice (SMMGP) and the Royal College of General Practitioners (RCGP). Guidance for hepatitis A and B immunisation of drug users in primary care and criteria for audit. 1st Edition 2005. Screening Guidelines Steering Committee commissioned by Clinical Effectiveness Group. Sexually Transmitted Infections: UK National Screening and Testing Guidelines. August 2006 NPHS. Report A - Blood Borne Viral Hepatitis Action for Wales Research Programme – Developing the evidence base. Findings, Implications and Recommendations. October 2006. British Association of Sexual Health and HIV. United Kingdom National Guideline on the Management of the Viral Hepatitides A, B, C 2008. http://www.bashh.org.uk Accessed 13/02/2009 World Health Organisation (WHO) web site. http://www.who.int/csr/disease/hepatitis/en/index.htm Accessed 05/03/2009. Health Technology Assessment 2002; Volume 6: No. 31. Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice. Coles E and Pates R for Welsh Assembly Government. The Economic and Social Costs of Class A drug and alcohol abuse in Wales. Cardiff: Welsh Assembly Government (unpublished). National Treatment Agency for Substance Misuse. Treating Drug Misuse Problems: Evidence of Effectiveness. London: National Treatment Agency for Substance Misuse, 2006 Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 13 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales 20 21 22 23 Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care NPHS for Wales. Immunisation and Vaccination web pages. http://howis.wales.nhs.uk/sites3/home.cfm?orgid=474 Accessed March 2009. Heptonstall J. Strategies to ensure delivery of hepatitis B vaccine to injecting drug users. Communicable Disease and Public Health, 1999. 2(3): p.154-6. http://www.nhs.uk/hepatitisc/hcp/testing-for-hepatitis-c/Pages/who-to-test.aspx The British Liver Trust http://www.britishlivertrust.org.uk/home/the-liver/liverdisease/hepatitis-c-updated.aspx Accessed 16th June 2009 Public Health Wales formerly NPHS for Wales. Childhood Immunisation (COVER) data April-June 2009 http://howis.wales.nhs.uk/sites3/page.cfm?orgid=474&pid=21302 Accessed Sept 2009 Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 14 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Practice Review A. What lessons did the practice discover from carrying out this audit? B. What changes, if any have the practice agreed to implement as a result of this audit? C. What support would enable the practice to enhance the service it provides to patients? This audit was compiled by; Name(s) ___________________________________________________________ Signature(s) ___________________________________________________________ Practice (name and address) ________________________________________________________________________ Date ___________________________________________________________________ Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 15 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Quality improvement toolkit – evaluation form The Primary Care Quality and Information Service would like to ensure that the information and suggested tools help practices to monitor and audit their practice data, therefore please could you take a moment and provide your comments on the blood borne viral hepatitis quality improvement toolkit. 1) Did you find the introduction, aims and methodology to be clear and easy to understand? YES NO If No, please comment _____________________________________________ 2) Did you find the organisational checklist to be clear and easy to understand? YES NO If No, please comment _____________________________________________ 3) Did you find the patient audit data proforma easy to use? YES NO If No, please comment _____________________________________________ 4) Did you find the practice review template helpful? YES NO N/A If No, please comment _____________________________________________ 5) Did you find the hints and tips section useful? YES NO N/A If No, please comment _____________________________________________ 6) Did you find the information within the appendices helpful? YES NO If No, please comment _____________________________________________ 7) Do you have any suggestions on how we should improve our quality improvement Toolkits? Please send to: Laura Beer, PCQIT NPHS 36 Orchard Street Swansea SA1 5AQ / or email [email protected] Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 16 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Appendix A Recommended Tests This figure is based on a flow chart produced by DoH and adapted by WAG1, and outlines the key stages in diagnosis and referral to specialist hepatitis treatment services and is relevant to all those responsible for diagnosis and referral. Diagnosis and referral pathways for blood borne viral hepatitis Client / Patient with identified risk factors behavioural or clinical Pre test discussion Sample 1 – Dried blood spot or venepuncture blood test Negative antibody test result Positive antibody test result Retest within 12 weeks (window period) Sample 2 – Further confirmatory venepuncture antibody tests Negative result – viral load not detected Positive result and viral load detected Further antibody tests Post test discussion. No treatment required. May need further tests in future Post test discussion. Genotype testing and liver function tests. Referral to specialist hepatitis services If outside window period – post test discussion In the case of chronic --------------- infection, notification to local Health Protection Team 1. Welsh Assembly Government. Proposed Blood Borne Viral Hepatitis Action Plan for Wales 2009-2014. http://new.wales.gov.uk/consultations/healthsocialcare/blood/?lang=en&status=closed Accessed November 2009. Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 17 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Appendix B READ Codes Note: “Risk Groups” - NHS Connecting for Health have been contacted to request new READ Codes on the italic bulleted lists on pages 5,6,7. New READ codes are released quarterly, updates are available on the Connecting For Health website http://www.connectingforhealth.nhs.uk/systemsandservices/data/readcodes/changestocurrentrelease Read V2 Code CTV3 Code Read V2 Description CTV3 Description RISK GROUPS 65PL. Hepatitis B contact 65PM. Hepatitis C contact 13N5. Multiple sexual partners 13N9. Sexual contact with high risk partner 1P70. Number of sexual partners in past year Xa1pO XaLGb Ua1ZB XaLHk Ub0oP 133N. Approved foster parent XaF0D L1765 L1765 13c.. Viral hepatitis complicating pregnancy, childbirth and the puerperium Drug user Ub0mt Hepatitis B contact Hepatitis C contact Multiple sexual partners Sexual contact with high risk partner Number of sexual partners in past year – requested new term Approved foster parent – new term requested Viral hepatitis complicating pregnancy, childbirth and the puerperium Drug user 13c0. 13c1. 13c2. 13c3. Injecting drug user Intravenous drug user Never injecting drug user Intramuscular drug user Ub00U Ub0nA XaJgi Ub0n9 Injecting drug user Intravenous drug user Never injecting drug user Intramuscular drug user Ub0n4 XaKSC XaKcY Intranasal drug user Current drug user Previously injecting drug user Ua1O4 XaLTv 6828. XaLND XaKuU XaIyP 8CE.. XaLoH XaBib 677Q. XaLTu XaJh4 XaLDh XaLNE XaNPZ Pre-screening counselling Hepatitis B screening counselling Hepatitis B screening Hepatitis B screening declined Health education - safe sex Health education - sexual health Self-help advice leaflet given Safer sex leaflet given Drugs – health education Hepatitis C screening counselling Hepatitis C screening counselling Hepatitis C screening Hepatitis C screening offered Hepatitis C screening declined Hepatitis C screening not offered XaLIH XaKiz XaKiz Hepatitis B immunisation declined Hepatitis B immunisation refused No consent for hepatitis B 13c4. Intranasal drug user 13c7. Current drug user 13cJ. Previously injecting drug user PRE SCREENING COUNSELLING 677J. Pre-screening counselling 677R. Hepatitis B screening counselling 6828. Hepatitis B screening 8I3u. Hepatitis B screening declined 679S. Health education. - safe sex 679K. Health education - sexual health 8CE.. Self-help advice leaflet given 8CEC. Safer sex leaflet given 679A. Health ed. – drugs of addiction 677Q. Hepatitis C screening counselling 6829. 9Op1. 8I3v. 682A. Hepatitis C screening Hepatitis C screening offered Hepatitis C screening declined Hepatitis C screening not offered IMMUNISATIONS 8I3r. Hepatitis B immunisation declined 68Nm. Hepatitis B immunisation refused 68Nm. No consent for hepatitis B immunisation Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 18 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care immunisation Requires a course of hepatitis B Hepatitis B immunisation recommended History of one hepatitis B immunisation History of two hepatitis B immunisations History of three hepatitis B immunisations 1st hepatitis B immunisation 2nd hepatitis B immunisation 3rd hepatitis B immunisation Booster hepatitis B immunisation 4th hepatitis B immunisation 5th hepatitis B immunisation Sixth hepatitis B immunisation Third combined hepatitis A and B vaccination First combined hepatitis A and B vaccination Second combined hepatitis A and B vaccination Booster combined hepatitis A and B vaccination 65W5. 65WC. Requires a course of hepatitis B Hepatitis B immunisation recommended 65W5. XaMe9 14b0. History of one hepatitis B immunisation XaN0g 14b1. History of two hepatitis B immunisations XaN0h 14b2. History of three hepatitis B immunisations XaN20 65F1. 65F2. 65F3. 65F4. 65F6. 5F7. 665FM 65MF. 1st hepatitis B immunisation 2nd hepatitis B immunisation 3rd hepatitis B immunisation Boost hepatitis B immunisation 4th hepatitis B immunisation 5th hepatitis B immunisation Sixth hepatitis B immunisation Third combined hepatitis A and B vaccination First combined hepatitis A and B vaccination 65F1. 65F2. 65F3. 65F4. 65F6. 65F7. XaKXg 65MF. Second combined hepatitis A and B vaccination Booster combined hepatitis A and B vaccination 65ME. RESULTS 43X6. 43dC. 43dB. 43d8. 43B.. 43dA. 43d9. 43B8. 43d8. 43dB. A703. Hepatitis C antibody level Hepatitis B e antibody level Hepatitis B core antibody level Hepatitis B surface antibody level Hepatitis B immunity test Hepatitis B core IgM level Hepatitis B surface antigen level Hepatitis B core antigen test Hepatitis B surface antibody level Hepatitis B core antibody level Viral (serum) hepatitis B XaIM5 XaFuV XaFuU XaFuR XE2ww Hepatitis C antibody level Hepatitis B e antibody level Hepatitis B core antibody level Hepatitis B surface antibody level Hepatitis B immune XaFuS XaEOm XaFuR XaFuU A703.% Hepatitis B surface antigen level Hepatitis B core antigen test Hepatitis B surface antibody level Hepatitis B core antibody level Viral serum hepatitis B A707.% Chronic viral hepatitis 43B6. 6773. 6772. 677B. 65X.. Hepatitis B non-immune Investigation result counselling Disease counselling Advice about treatment given Contact tracing 44D6. 43X2. 43dD. Liver function test Hepatitis C antibody test Hepatitis C recombinant immunoblot assay 43B6. 6773. 6772. 677B. Ua1RW XaAgt X77WP XaEOG XaFuX Hepatitis C viral load not detected Hepatitis C viral load detected Hepatitis B non-immune Investigation result counselling Disease counselling Advice about treatment given Contact tracing Referral to contact tracing nurse Liver function tests Hepatitis C antibody test Hepatitis C recombinant immunoblot assay New term requested New term requested Hepatitis C sustained negative viral load New term requested 65MD. 65ME. 65MG. Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 65MD. 65MG. Date October 2009 19 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Acute Hepatitis C Active Hepatitis C (up to 12 months) Chronic Hepatitis C (after 12 months) Past history of HCV successfully eradicated HCV spontaneous clearance Hepatitis re-infection REFERRAL 8H15. Referral to drugs therapist 8Hk5. Referred to hepatology service 8HA5. Follow-up refused 8H48. Gastroenterological referral 8HVN. Private referral to Gastroenterologist 8Hk5. Referred to hepatology service TREATMENT FOR HBV/HCV 9N42. Did not attend - no reason 9N41. Did not attend - reason given 9kX.. Hepatitis status 6 months post treatment enhanced services administration FOLLOW UP 9G1.. Infectious disease notification 65V.. Notification of disease 9kT.. Hepatitis C screening negative - enhanced services administration 9kV.. Hepatitis C screening positive - enhanced services administration 9kR.. Chronic hepatitis annual review - enhanced services administration Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 New term requested New term requested New term requested New term requested New term requested New term requested XaMzM XaLrh 8HA5. 8H48. 8HVN. XaLrh Referral to drugs worker Referred to hepatology service Follow-up refused Referral to gastroenterology service Private referral to gastroenterologist Referred to hepatology service XE2NM 9N41. XaPE9 Did not attend - no reason Did not attend - reason given Hepatitis status 6 months post treatment - enhanced services administration XE2Mn 65V.. XaPLZ Infectious disease notification Notification of disease Hepatitis C screening negative enhanced services administration Hepatitis C screening positive enhanced services administration Chronic hepatitis annual review enhanced services administration XaPLl XaPLW Date October 2009 20 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS Public Health Wales Screening, Testing & Immunisation for Blood Borne Viral hepatitis in Primary Care Appendix C Patient Leaflets Patient information leaflets on Hepatitis are available from the following: National Public Health Service for Wales has Information for pregnant women who are hepatitis B positive available at: http://howis.wales.nhs.uk/sites3/page.cfm?orgid=474&pid=21234 The British Liver Trust have a variety of booklets on Hepatitis A,B,C, available on request from the British Liver Trust, 2 Southampton Road, Ringwood, BH24 1HY. Tel 0800 652 7330 or web www.britishlivertrust.org.uk Patient UK have information leaflets on Hepatitis A,B,C, and Immunisation for Hepatitis A, B available from http://www.patient.co.uk Author Primary Care Quality & Information Service Blood Borne Viral Hepatitis Version 1 Date October 2009 21 Status; Final Version 1 Intended audience: Public (Internet)/ NHS (intranet PHW (Intranet) / PCQIS