Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
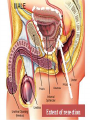
URO ONCOLOGY DONE BY: SHATHA MUQBIL SHAMS KADHIM ANATOMY: The bladder is an extraperitoneal muscular urine reservoir that lies behind the pubis symphysis in the pelvis . The ureters, which transport urine from kidney to bladder, approach the bladder obliquely and posterosuperiorly, entering at the trigone (the area between the interureteric ridge and the bladder neck). The bladder neck serves as an internal sphincter. In males, the seminal vesicles, vas deferens, ureters, and rectum border the inferoposterior aspect of the bladder. Anteriorly there is space filled with fibroadipose tissue and the prevesical fascia. The dome and posterior surface of the bladder are covered by parietal peritoneum, which reflects superiorly to the seminal vesicles and is continuous with the anterior rectal peritoneum. In females, the posterior peritoneal reflection is continuous with the uterus and vagina. ANATOMY: BLADDER CANCER: Almost all bladder cancers originate in the urothelium, which is a 3- to 7-cell mucosal layer within the muscular bladder. Squamous cell carcinoma of the bladder can involve multiple sites; however, the lateral wall and trigone are more commonly involved. 90% of bladder cancers are TCC. In developing countries—particularly in the Middle East and Africa—the majority are SCCs, and most of these are secondary to Schistosoma haematobium infection BLADDER CANCER: The incidence of bladder cancer increases with age, with the median age at diagnosis being 65 years; & rarely diagnosed before age 40 years. Bladder cancer is about 3 times more common in men than in women. The incidence of bladder cancer is twice as high in white men as in black men in the United States. However, blacks have a worse prognosis than whites. Causes: • Tobacco smoking is the main known contributor; & associated with over half of cases in men and one-third among women. • occupational exposure in the workplace to carcinogens such as benzidine & naphthylamine, Occupations at risk are bus drivers, rubber workers, motor mechanics, leather (including shoe) workers, machine setters, and mechanics. Hairdressers are thought to be at risk as well because of their frequent exposure to permanent hair dyes. •It has been suggested that mutations at HRAS, KRAS2, RB1, and FGFR3 may be associated in some cases. CLINICAL PRESENTATION: BY HISTORY: • painless gross hematuria (8090%) MALAGNANCY UNTIL PROVED OTHERWISED • Irritative bladder symptoms : dysuria, urgency, or frequency of urination (20-30%) may be related to more advanced muscleinvasive disease, carcinoma in situ (CIS) is the more likely cause •pelvic or bony pain, lowerextremity edema from iliac vessel compression, or flank pain from ureteral obstruction THIS INDICATE A MORE ADVANCED DISEASE BY EXAMINATION: typically nothing significant during a physical examination. In rare cases, a mass is palpable during abdominal, pelvic, rectal, or bimanual examination. A bimanual examination may be considered part of the staging of such lesions Attention to the anterior vaginal wall in women and the prostate in men may reveal findings that suggest local extension of bladder cancer. Assessment of fixation of the bladder to the surrounding pelvic sidewall is also important when planning definitive management for locally advanced tumors that may not be surgically resectable. DIAGNOSIS: Approach Considerations Urine studies include the following: •Urinalysis with microscopy to detect hematuria or infection •Urine culture to rule out infection, if suspected •Voided urinary cytology: is extremely valuable and is often the test used for diagnosis. IT is most helpful in diagnosing high-grade tumors and carcinoma in situ (CIS). Low-grade, noninvasive tumors may be missed by routine cytologic analysis . •Urinary tumor marker testing may help in the early detection and prediction of urothelial carcinoma. however, no urinary assay has been shown to effectively replace urine cytology and cystoscopy. DIAGNOSIS: Imiging: •Computed tomography (CT) scans of the abdomen and pelvis with contrast are recommended. • magnetic resonance imaging (MRI) and renal ultrasonography. •Few US centers still perform intravenous pyelography (IVP) for upper tract imaging. The bladder urothelium is not well visualized with routine imaging studies, including CT scanning and MRI. Small tumors are easily missed on images produced by these modalities. Irregular areas on images, which may appear to represent mucosal abnormalities, are often artifacts of incomplete bladder filling; delayed images following contrast administration can better visualize actual filling defects. CIS is not visible on images from any current radiographic study DIAGNOSIS: Cystoscopy: Is gold standard for detecting bladder cancer, but it is invasive and relatively expensive. Moreover, visibility can be reduced by bleeding, and flat urothelial lesions such as CIS may be difficult to distinguish from normal bladder tissue. Use of adjunctive endoscopic techniques may improve the accuracy of cystoscopy. DIAGNOSIS: DIAGNOSIS: TREATMENT: Tis Complete TURT + Intravesical BCG Ta (Single) Complete TURT Ta (Multiple) Complete TURT + Intraveiscal chemotherapy T1 Complete TURT + Intravesical Chemotherapy T2 – T4 Any 1) Radical Cystectomy 2) Neoadjuvant Chemotherapy + Radical Cystectomy 3) Radical Cystectomy + Adjuvant Chemotherapy T , N+ , M+ Systemic Chemotherapy followed by selective surgery TREATMENT: BCG Mitomycin-C Thiotepa Instilled directly into the Bladder via a Urinary Catheter to avoid morbidity of systemic administration. I. II. III. Adjunctive : at time of TURT to prevent implantation Prophylactic : after complete TURT to delay recurrence or progression Therapeutic : after Incomplete TURT to cure residual tumor. To improve efficacy : 1. 2. 3. 4. Avoid Air instillation Increase contact time Increase drug conc. By decreasing fluid intake Changing patient’s position during therapy TREATMENT: Is the initial treatment for most bladder cancers . Patient should be checked every 3 months after the operation for recurrence. TREATMENT: The Gold Standard for Muscle-Invasive CA. Includes removal of : In Male : Bladder ( &its surrounding fat and peritoneal attachment) Prostate Seminal Vesicles In Female : Bladder ( &its surrounding fat and peritoneal attachment ) Ovaries Uterus Cervix Anterior Vaginal Vault.