Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
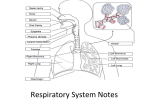
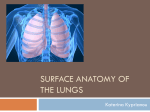
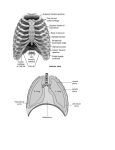
Dr.Naresh Kumar Junior Resident Dept. of Pulmonary Medicine AnAtomy of pleurA… Definition and layers of Pleura Embryology Histology Surface marking Recesses of pleura Blood supply Lymphatic drainage Nerve supply Definition and layers of Pleura • Pleura : • Serous membrane that covers the lung parenchyma, mediastinum, diaphragm and the rib cage. • It comprise visceral and parietal layer. Visceral pleura – Covers the lung parenchyma, not only at its point of contact with chest wall, diaphragm and the mediastinum but also in the interlobar fissures. – It apposed to lungs and cannot be dissected from the surface. • Endo pleura : Most superficial layer Composed of a continuos layer of mesothelial cells External elastic layer (chief layer) Consist of thin layer of dense collagen and elastic tissue Responsible for pleural mechanical stability Vascular layer (interstitial layer) Consist of connective tissue containing lymphatic and blood vessels. Continuos with the interstitial tissue of the interlobular septa and directly overlies the lobular-limiting membrane. Parietal pleura – It lines the thoracic wall. – Covers the inner surface of rib cage, mediastinum and diaphragm. – It extends into the root of neck to line the undersurface of suprapleural membrane at thoracic outlet According to intrathoracic surface it lines :- Cervical pleura Costal pleura Diaphragmatic pleura Mediastinal pleura • Cervical pleura : – “pleural capula” or dome of pleura. – It extends from the superior thoracic aperture into the root of neck, forming a cup shaped pleural dome over the apex of lung. – The cervical pleura at higher levels in infants and young children because of the shortness of their necks, thus more prone to injury. – The small areas of pleura exposed in the costo vertebral angles inferiomedial to the 12th ribs are posterior to the superior poles of kidneys. More prone to injure during surgical procedure in posterior abdominal wall. • Costal pleura : – It covers the internal surface of : • • • Ribs Intercostal spaces Back of sternum Costal cartilages Sides of vertebral bodies • Mediastinal pleura : – It covers the lateral aspects of the mediastinum. – It is attached to blood vessels and bronchi that constitute the lung root. • Diaphragmatic pleura : – Covers the superior or thoracic surface of diaphragm on each side of mediastium. – In quite respiration the costal and the diaphragmatic pleura are in apposition to each other. – They separate in deep inspiration. Pleural cuff The two layers, parietal and visceral, continuous with one another by means of a cuff of pleura. This cuff surrounds the structures entering and leaving the lung at the hilum of each lung. Pleural cuff hangs down as loose fold called the pulmonary ligament. Fold contains a thin layer of loose areolar tissue with a few lymphatics. It provides a dead space into which the pulmonary veins can expand during increased venous return. Embryology of pleura • Pleural cavity : – Derived from the coelomic cavity (body cavity) – Coelomic cavity divided into pericardium, pleural cavities and the peritoneal cavity through the development of three sets of portions : • • • Septum transversum : serves as an early partial diaphragm. Pleuro pericardial membranes : divide pericardial and pleural cavities. Pleuro peritoneal membranes : unite with the septum transversum to complete the partition between each pleural and peritoneal cavity. – Pleural cavity is fully lined by mesothelial membrane, the pleura. Visceral pleura : Primordial lung buds grows and bulge into right and left pleural cavities, carry along lining mesothelium which becomes visceral pleura. Parietal pleura : Lining mesothelial of pleural cavity becomes parietal pleura. Histology • Grossly, normal pleura is a smooth, glistening, semitransparent membrane. • Light microscopy, pleural consist of five layers : – Mesothalial layer – Connective tissue layer – Superficial elastic layer – Loose subpleural connective tissue layer (rich in vessels, nerves and lymphatics) In pleural fibrosis connective tissue is arranged in a coarse, basket weave pattern and contains only a few capillaries. – Deep fibroelastic layer (in continuity with the parenchymal structures of lung, diaphragm or the thorax) Mesothelial layer • Single cell layer • Different shaped cells – flattend or cuboidal or • • • • • columnar 6-12mm thickness Microvillae present to decrease friction Stomata present between the mesothelial cells that communicate directly with lymphatic lucanes. Capable of transformation into macrophages. In a rheumatoid pleuritis, normal mesothelial cell covering absent, instead there is pseudostratified layer of epitheloid cells that focally forms multinucleated giant cells . Surface marking Recesses of pleura There are two folds or recesses of parietal pleura which acts as reserve space for the lung to expand during deep inspiration. Costomediastinal recesses Costodiaphragmatic recesses Costomediastinal recesses Are situated along the anterior margins of pleura. They are slit like spaces between the costal and the mediastinal parietal pleura. Seperated by a capillary layer of pleural fluid. During inspiration and expiration, the anterior borders of the lungs slide in and out of the recesses. Costodiaphragmatic recesses • Are slit like spaces between the costal and • • • • • diaphragmatic parietal pleura. Separated only by a capillary layer of pleural fluid. During inspiration, the lower margins of the lung descend into the recesses. During expiration, the lower margins of the lung ascend so that the costal and the diaphragmatic pleura come together again. First part of pleural cavity to be filled up by pleural effusion. It has capacity upto 300 ml. Blood supply • Arterial supply : – Parietal pleura : • • • Costal pleura : small branches of intercostal arteries Mediastinal pleura : supplied by pericardio phrenic artery Diaphragmatic pleura : supplied by superior phrenic and musculophrenic artery. – Visceral pleura : • • Bronchial artery : supplies visceral pleura facing the mediastinum, pleura covering the interlobular surface and part of the diaphragmatic surface. Pulmonary artery : supplies remaining portion. Venous drainage : Parietal pleura Through the intercostal veins which empty into inferior venacava or brachio-cephalic trunk. Visceral pleura Through pulmonary veins. Applied anatomy : Aspiration of any fluid from the pleural cavity is called parencentesis thoracis. It is usually done in the 6th intercostal space in the midaxillary line. The needle is passed through the lower part of the space to avoid injury to the neurovascular bundle. Nerve supply • Parietal pleura : – Sensitive to pain, temperature, touch and pressure. Costal pleura : innervated by segmental intercostal nerves. Peripheral part of diaphragmatic pleura : innervated by lower 6 intercostal nerves. pain is percieved in adjacent chest wall. Central portion of diaphragmatic pleura and mediastinal pleura : innervated by phrenic nerve. Pain is percieved in ipsilateral shoulder. • Visceral pleura : – Insensitive to common sensation such as pain and touch. – Sensitive to stretch. – Innervated by autonomic nerves from the spinal segments T4 and T5. • Presence of pleuritic chest pain indicates inflammation or irritation of parietal pleura. Applied anatomy : Intrapleural anaesthesia :it is infusion of small volume of local anaesthetic agent into the intrapleural space through catheter. It diminish the pain sensation from the area by action on intercostal nerves, indicated in thoracotomy and insertion of chest drainage Lymphatic drainage • Parietal pleura : – Costal pleura : • • Ventrally : towards nodes along the internal thoracic artery. Dorsally : towards the intercostal lymph nodes. – Medistinal pleura : • Drain to tracheobronchial and mediastinal nodes. – Diaphragmatic pleura : • Drain to parasternal, middle phrenic and posterior mediastinal nodes. • Lymphatic vessels in parietal pleura are in communication with the pleural space by means of stoma. • Stoma : – 2-6 mm in diameter – Round or slit like opening – Found mostly on the mediastinal pleura and on the intercostal surfaces. – More stoma in the area where the mesothelial cells are cuboidal rather then flat. • Lacunas : – Lymphatic vessels in parietal pleura have many branches, some submesothelial branches have dilated lymphatic space called lacunas. • Stomas are found only over lacunas. • Significance : Stomas with their associated lacunas and lymphatic vessels are main pathway for elimination of particulate matter from pleural space. This transport system may provide a mechanism for migration of malignant cell to distant organs in patients with positive pleural lavage cytology. • Visceral pleura : – They have abundant lymphatic vessels. – Lymphatics form a plexus of inter communicating vessels that run over the surface of lung towards the hilum. – It also penetrate the lungs to join the bronchial lymph vessels. – Lymphatic vessel in visceral pleura have one way valves, directing flow towards the hilum of lung. – No stomas are seen in visceral pleura. Physiology of pleura Pleural pressure Pleural fluid Pleural effusion Therapeutic application of pleural space Clinical condition associated with pleura Pleural pressure It is pressure within the pleural space. It is pressure at the outer surface of the lung and heart, and inner surface of thoracic cavity. With the chest closed and the patient relaxed, the respiratory system is at its functional residual capacity (FRC), which is approximately 35% of the total lung capacity. Thus, at FRC, the opposing elastic forces of the chest wall and lung produce a negative pressure between the visceral and the parietal pleura, which is called the pleural pressure. Significance : Because the lung, the heart, and the thoracic cavity are all distensible, and because the volume of a distensible object depends on the pressure difference between the inside and the outside of the object and its compliance, pleural pressure plays an important role in determining the volume of these structures. Pleural liquid pressure pressure measured using fluid-filled catheters 1.0 cm H2O/cm vertical height. It represents the pressure that influenced the absorption of fluid. Pleural surface pressure pressure measured using surface balloons or suction cups. 0.3 cm H2O/cm vertical height. It represents the balance between the outward pull of the thoracic cavity and the inward pull of the lung. Measurement Direct methods measured by inserting needles, trocars, catheters, or balloons into the pleural space. Highly risk of producing a pneumothorax or of introducing infection into the pleural space. Indirect methods measured by a balloon positioned in the esophagus. esophagus is a compliant structure situated between the two pleural spaces, esophageal pressure measurements provide a close approximation of the pleural pressure. Precaution to be taken – volume of air within the balloon must be small, so that the balloon is not stretched and the esophageal walls are not displaced; balloon must be short and balloon must be placed in the lower part of the esophagus. Gradients Pleural pressure is not uniform throughout the pleural space. pleural pressure being lowest or most negative in the superior portion and highest or least negative in the inferior portion. factors responsible for gradient gravity, mismatching of the shapes of the chest wall and lung, weight of the lungs The magnitude of the pleural pressure gradient appears to be approximately 0.30 cm H2O/cm vertical distance. Significance of gradient : alveolar pressure is constant throughout the lungs, thus, higher pressure gradient at the apex of the lung is thought to be responsible for the formation of pleural blebs at the apex of the lung. It also play a role in difference in ventilation at apex and base of lung. Pleural fluid Fluid present between the parietal and visceral pleura, the pleural space is called pleural fluid. Fluid act as lubricant and allows the visceral pleura covering the lung to slide along the parietal pleura lining the thoracic cavity during respiratory movements. Volume : Mean amount of fluid in right pleural space in normal individual is 8.4 +/- 4.3 ml. Normally the volume of fluid in right and left pleural space is equal. Thickness : Pleural space slightly more narrow near the top(18.5mm) than at bottom(20.3mm). pleural space width in the most dependent recess such as costodiaphragmatic recess reaches 1 to 2 mm. Cells : Mean WBC count – 1,716 cells/mm3 Mean RBC count – 700 cells/mm3 Macrophages – 75 % Lymphocytes – 25 % Mesothilial, neutrophils, eosinophils ( < 2 % each ) Eosinophil > 10 % -- drug reaction, asbestosis, parasitic infection, churg-strauss syndrome. Physiochemical factors : • Protein – pleural fluid is similar to that of serum except that low molecular weight protien such as albumin present in relatively greater quantities in plural fluid. • Ions : Bicarbonates : increase by 20-25% to that in plasma. Sodium : reduce by 3-5% to that in plasma Chloride : reduce by 6-9% to that in plasma Potassium : nearly identical to that in plasma • Glucose : similar to that in plasma • Less than 60 mg/dl – parapneumonic effusion, malignancy, TB, RA, parasitic infection, churg-strauss syndrome. • Pco2 : same as the plasma Pco2 • pH : due to elevated pleural fluid bicarbonate the pleural fluid is alkaline with respect to plasma pH. • Apperance : normally light yellow and clear Appearance Underlying disaese Pale yellow Transduates Turbid Inflammatory exudates Pus Empyema Haemorrhagic Trauma, malignancy Milky fluid Chylotorax Brown Amoebic liver abcess Black Fungal infection Yellow to green Rheumatoid pleurisy Pleural Fluid Formation Sources pleural capillaries, interstitial spaces of the lung, intrathoracic lymphatics, intrathoracic blood vessels, peritoneal cavity. Pleural Capillaries The movement of fluid between the pleural capillaries and the pleural space governed by Starling's law of transcapillary exchange. [Q]f - liquid movement Lp - filtration coefficient/unit area or hydraulic water conductivity of the membrane A - surface area of the membrane Pcap and pcap - hydrostatic and oncotic pressures of capillary Ppl and ppl - hydrostatic and oncotic pressures of pleural space sd - solute reflection coefficient for protein, Parietal Pleura gradient for fluid formation is normally present. Hydrostatic pressure hydrostatic pressure of capillaries in parietal pleura is 30 cm of H2O Pleural pressure is -5 cm of H2O Net hydrostatic pressure = 30 – (-5) = 35 cm of H2O Oncotic pressure : Oncotic pressure in plasma = 34 cm of H2O Oncotic pressure in pleural space = 5 cm of H2O Net oncotic pressure = 34-5 = 29 cm of H2O Net gradient = 35-29 = 6 cm of H2O This gradient favours the movement of fluid from capillaries in parietal pleura to the pleural space. Visceral pleura Pressure in the visceral pleural capillaries is approximately 6 cm of H2O less than that in the parietal pleural capillaries. Filtration coefficient for the visceral pleura is less than that of parietal pleura, because the capillaries in the visceral pleura are much further from the pleural space than those in parietal pleura. Thus, net gradient for fluid movements across the visceral pleura is close to zero. Interstitial It acts as a source of pleural fluid formation in CHF Pulmonary edema Lung transplantation Pulmonary embolisation Movement of fluid from interstitial to pleural space is closely related with pulmonary venous pressure than with the systemic venous pressure. Peritoneal cavity Act as a source of pleural fluid formation in Hepatic hydrothorax Meig’s syndrome Peritoneal dialysis Pressure in the pleural cavity is less than that of peritoneal cavity Thoracic duct/Blood vessel Thoracic duct injury : lymph will accumulate in pleural space producing chylothorax. Rate of fluid accumulation can be more than 1000ml/day Blood vessel injury : Trauma of the blood vessels leading to blood accumulation in pleural space cause hemothorax. Pleural fluid absorption Lymphatic clearance : Pleural space is in communication with lymphatic vessels in the parietal pleura by stomas in parietal pleura. Stomas are not present in visceral pleura Proteins, cells and all other particulate matter are removed from the pleural space by this lymphatics in parietal pleura. More fluid formation across the parietal pleura over the ribs compared with intercostal spaces. Pleural fluid absorption more over intercostal spaces than over ribs. More fluid formation over the caudal ribs than over the cranial ribs. Increase in breathing frequency results in more fluid formation. Pleural effusion Pleural effusion is excess fluid that accumulates between the two pleural layers, the fluid-filled space that surrounds the lungs. It occurs when the rate of pleural fluid formation exceeds the rate of pleural fluid absorption. Normal rate of pleural fluid formation – 0.01 ml/kg/hr Normal rate of pleural fluid absorption – 0.01 ml/kg/hr but it can exceed upto 0.20 ml/kg/hr Causes… Increased pleural fluid formation Increased interstitial fluid in the lung (most common) Left ventricular failure, pneumonia, and pulmonary embolus Increased intravascular pressure in pleura Right or left ventricular failure, superior vena caval syndrome Increased permeability of the capillaries in the pleura Pleural inflammation Increased levels of vascular endothelial growth factor Increased pleural fluid protein level Decreased pleural pressure Lung atelectasis or increased elastic recoil of the lung Increased fluid in peritoneal cavity Ascites or peritoneal dialysis Disruption of the thoracic duct Disruption of blood vessels in the thorax Decreased pleural fluid absorption Obstruction of the lymphatics draining the parietal pleura Elevation of systemic vascular pressures Superior vena caval syndrome or right ventricular failure Disruption of the aquaporin system in the pleura Transudative vs exudative Transudative – CHF Cirrhosis Pulmonary embolism Nephrotic syndrome Peritoneal dialysis Myxedema SVC syndrome Exudative : Infections Connective tissue disease Cancer Pancreatitis Chylothorax Drug reaction Exudative effusion Light’s criteria [satisfying anyone criterion means it is exudative] Pleural total protein/serum total protein > 0.5 Pleural LDH/serum LDH > 0.6 Pleura LDH > 2/3 of the upper limits of normal for serum LDH For patients with high suspicion for transudative, but meets light’s criteria – Serum albumin – pleural albumin < 1.2 gm/dl confirm the effusion is exudative. Therapeutic uses of pleural space Intrapleural gene transfer : Easy accessibility Large surface area Ability to provide high concentration of secreted gene products to chest structure Low risk of vector induced inflammation Treatment of accidental hypothermia Clinical conditions associated with pleura • Pleuritis or pleurisy : This is the inflammation of the • • • • pleura. Acute pleuritis is marked by sharp, stabbing pain, especially on exertion. Pneumothorax : Presence of air in the pleural cavity. Entry of air into the pleural cavity, resulting from a penetrating wound of the parietal pleura or rupture of a lung results in partial collapse of the lung. Hemothorax : Presence of blood in the pleural cavity. It results more often from injury to a major intercostal vessel than laceration of lung. Hydropneumo thorax : prence of both fluid and air in the pleural cavity. Empyema : presence of pus in pleural cavity.