Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
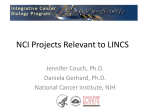
(CANCER RESEARCH 48, 5565-5569, October 1. 1988] Model for Breast Cancer Survival: Relative Prognostic Roles of Axillary Nodal Status, TNM Stage, Estrogen Receptor Concentration, and Tumor Necrosis' Lydia L. M. Shek and William Godolphin2 Department of Pathology; The University of British Columbia and Vancouver General Hospital, Vancouver, British Columbia, Canada V5Z 1M9 ABSTRACT The independent prognostic effects of certain clinical and pathological variables measured at the time of primary diagnosis were assessed with Cox multivariate regression analysis. The 859 patients with primarybreast cancer, on which the proportional hazards model was based, had a median follow-up of 60 months. Axillary nodal status (categorized as No, NI.J or N4+)was the most significant and independent factor in overall survival, but inclusion of TNM stage, estrogen receptor (ER) concentra tion and tumor necrosis significantly improved survival predictions. Pre dictions made with the model showed striking subset survival differences within stage: 5-year survival from 36% (N4+, log,(ER| = 0, marked necrosis) to 96% (No, logJER) = 6, no necrosis) in TNM I, and from 0 to 70% for the same categories in TNM IV. Results of the model were used to classify patients into four distinct risk groups according to a derived hazard index. An 8-fold variation in survival was seen with the highest (>3) to lowest index values (< I ). Each hazard index level included patients with varied combinations of the above factors, but could be considered to denote the same degree of risk of breast cancer mortality. A model with ER concentration, nodal status, and tumor necrosis was found to best predict survival after disease recurrence in 369 patients, thus confirming the enduring biological significance of these factors. INTRODUCTION Survival after primary breast cancer surgery has consistently been found to be longer for patients with earlier clinical stage, or absence of axillary nodal involvement, or ER3 positivity, or better differentiated tumors. Although these findings are repro ducible, the independence and relative importance of each pre dictor is often obscured when un ivariate statistical methods are used. Furthermore, univariate survival curves do not explain why some patients, classified as prognostically favorable by one of these factors, may experience early treatment failure or that a substantial proportion of patients with axillary métastasesat initial diagnosis remain recurrence free even 20 years later (1). Such observations beg for improvement in identification of subset prognostic factors. A more comprehensive approach to survival prediction is the formulation of risk models through multivariate regression techniques. The Cox proportional hazards model is popular because of its statistical sophistication and adaptability to cen sored survival data (2). This technique facilitates the selection of factors that independently influence survival from multiple prognostic variables, some of which may be highly correlated. The selection can be hierarchical, in terms of relative impor tance, through the use of stepwise regression. We undertook this study with objectives to derive a multivar iate Cox model that incorporates only factors having independ ent predictive value for risk of breast cancer mortality, to extend the model to identify low- and high-risk groups, and to dem onstrate the intrastudy consistency of this model. The strength of the analysis is in the large sample size (n = 1184) with a maximum follow-up of 10 years and availability of a relatively extensive set of prognostic variables within the data base. Many of these patients (n = 457) experienced a disease recurrence which permitted investigation of an additional model specifi cally related to postrecurrence prognosis. MATERIALS AND METHODS Patients. The present series consists of women diagnosed with pri mary breast cancer between 1975 and 1981 who were referred to the Cancer Control Agency of British Columbia. During that time about 6000 patients were referred to the Agency. The studied group were from a consecutive series of 1600 from which tumor was submitted for measurement of ER. They were further selected by these criteria: valid ER analysis on the primary tumor, known dates of diagnosis, and no previous, concomitant, or later malignancy regardless of site (including bilateral breast cancer) except nonmelanoma squamous cell and basal cell carcinomas of the skin. Postoperative follow-up of patients was regularly maintained by the Agency or private physicians who corresponded through a standard follow-up form. Patients were referred back to the Agency for evaluation and therapy planning when recurrent disease was suspected or evident. Confirmation of recurrence was obtained by histopathological diagnosis of malignancy consistent with the primary tumor or through radiolog ical scans. The medical records were reviewed up to the end of 1985. The end point was death due to breast cancer as ascertained from death certificates or autopsy reports. There were 486 deaths; 96 were not due to breast cancer. Censored data include patients alive, with or without evidence of disease, and dead from other causes (when the primary cause of death as stated on death certificates or autopsy reports was not breast cancer). Patients were considered lost to follow-up if there was cessation of letter correspondence with the patients and if their physicians had no contact with them for a long period of time. The status of "lost to follow-up" was subsequently assigned when patient contact was unsuccessful, even after information was sought from known relatives, city or telephone directories, or vital statistics. In this study approximately 3% of all patients not known to be dead at the date of last contact were considered lost to follow-up; these data were also censored. Variables. The following patient and tumor characteristics were tested in the Cox analysis. Clinical TNM stage was assigned according to Union Internationale Contre le Cancer criteria, based on complete information on size of breast lump with or without fixation to underlying pectoralis muscle or chest wall, palpability of axillary lymph nodes, and presence or absence of distant spread as verified by metastatic work-up. The number of axillary node métastasesfor patients who had an axillary dissection was taken from the original pathology report and was categorized as none (No), 1 to 3 nodes positive (Ni-j), and 4 or more nodes positive (N4+). It was not possible to determine the mini Received 1/29/88; revised 5/27/88; accepted 7/1/88. mum number of nodes examined in each case; this information was not The costs of publication of this article were defrayed in part by the payment always recorded in a standard manner. However, the classification of of page charges. This article must therefore be hereby marked advertisement in negative nodes was made with confidence and an axillary dissection of accordance with 18 U.S.C. Section 1734 solely to indicate this fact. ' This research was supported by grants from the British Columbia Health an average of 10 nodes was the usual practice among local surgeons. Care Research Foundation and the British Columbia Cancer Foundation. Microscopic examination of available nodal sections was routine. 2To whom requests for reprints should be addressed. Tumors were analyzed for ER in a single laboratory by an established 3The abbreviations used are: ER, estrogen receptor; N0, 0 axillary nodes with radioactive ligand binding method described in detail elsewhere (3-5). cancer; NI_J, 1-3 axillary nodes with cancer; N«», 4 or more axillary nodes with Receptor concentration was uniformly expressed as fmol of bound cancer. 5565 Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1988 American Association for Cancer Research. SURVIVAL MODEL FOR BREAST CANCER estradici per mg of cytosol protein, corrected for serum protein accord Statistical Analyses. The proportional hazards model was specified ing to the recommendation of the European Organization for Research by Cox (7) in the form: on Treatment of Cancer (6). The lowest signal distinguishable from H(t, x) = //»(r)exp (ß,x, (A) noise or background was about 1 fmol/mg; such results were designated <1. to model the effects of the ßs upon the death (hazard) rate (//); where The following histológica! features were assessed by the same pa t is the time from diagnosis, A is a vector of prognostic variables thologist on a section of the tumor specimen adjacent to that sent for (covariates) x¡• • • A,,and //¡>(f) is an unknown base-line hazard function ER assay: (a) histológica! type of the dominant growth pattern; (¿>) when all covariates are equal to zero. The ßs are unknown regression degree of differentiation (well, moderate, or poor) in relation to the coefficients estimated by maximizing the partial likelihood function extent of tubule formation, nuclear pleomorphism, and mit otic activity; based on conditional probability of failure. A positive coefficient de (c) degree of confluent tumor necrosis (absent, minimal, or marked). notes an increased risk of death with increased value of covariate; a Tumor size as recorded in the pathology report was the largest negative coefficient denotes the opposite effect. diameter of the tumor. Stepwise-up regression of all covariates selects first the single co Age and menopausa! status were determined at the time of diagnosis. variate which produces the maximum likelihood, then adds the next Patients were excluded from the regression analysis if any of the above information was not available, resulting in 859 patients to be covariate which improves the likelihood of the preceding variable, and proceeds in the same manner until further covariates cannot be added studied. There was a significantly larger proportion of patients with at a chosen significance level (e.g., 0.05). advanced TNM stage in the excluded group (Table 1). These patients ER data were used as the sole continuous variable after logarithmic were most often excluded because an axillary dissection had not been transformation. Categorical variables (Acategories) were dummy coded done and hence pathological nodal status was unknown. into k —1 strata (8). For example, with TNM I as a referent stratum, The above variables were evaluated concomitantly with the effect of SI is a dummy variable that assumes the value 1 for TNM II, 0 systemic treatment type given after relapse in a model of postrecurrence otherwise; S2 is another dummy variable that has a value of 1 for TNM survival. Adjuvant systemic treatments were not considered in either model of overall or postrecurrence survival since preliminary un ¡variate III, 0 otherwise; S3 is the final dummy variable with a value of 1 for TNM IV and 0 otherwise. Both differentiation (0 = well or moderate, analyses had shown they had little significant impact on survival. The 1 = poor) and necrosis (0 = absent or minimal, 1 = marked) were coded major postrecurrence systemic treatment types for the 369 patients on as binary variables since preliminary analysis indicated no significant which this model was based were: (a) cytotoxic chemotherapy if the difference in survival between the combined subgroups. patient had no or low ER, regardless of menopausa! status; (b) endo The Cox proportional hazards models were generated with EPILOG crine therapy by ovarian ablation in ER-positive premenopausal pa (9). The predicted survival functions based on different covariate pat tients and tamoxifen for ER-positive or ER-unknown postmenopausal terns were obtained with the program RISK (10). Program P:2L of patients; (c) both endocrine and cytotoxic chemotherapies given se BMDP (11) was used to check the proportionality assumption of the quentially. model with stratification of covariates. Table 1 Distribution of patients by characteristic at time of primary diagnosis One or more data points considered for the stepwise regression analysis were missing from the excluded group. The distribution of ER status is given in this table: however, all statistical analyses were performed with the actual concentralion infr»rmatir»nStudied erouDVariableER P"0.77 66 10456 34<0.00120 IIIIIIVNodesNoN,-JN*.Menopausal 11563517655448617833 402218 Four riclr COvariatCS nf iTinrtillitv were shown to be predictive of the Overall anH i»Qr»h f»r»nvpvi»H r»rr»onnctir' withthe from the others (Table 2). Nodal status associated themodel greatest likelihood value and hence was selected into next;thefirst. TNM stage entered the regression equation incremental coefficients reflect the detrimental effects of increased stage at presentation. The negative coefficient oflogf[ER] increasingER indicates the reduced risk associated with concentration. The final variable selected was tumor necro sis. Marked confluent necrosis was associated with a greaterrisk necrosis.Table of mortality than minimal or no grouDn199 status ER positive (>10 fmol/mg) fmol/mg)TNMI ER negative (<10 RESULTS 0.994332250.7733670.3910 2 Final proportionalhazards step of stepwise regression analysis by the Cox survivalOnly models for overall and postrecurrence status:PremenopausalPostmenopausalAge included.The cases with complete information on all studied variables were regressioncoefficient significance of the covariate level is indicated by a standardized 2.0corresponds (estimated ßdivided by its standard error); a value greater than (yr)<40 at diagnosis roughly (32).Variable to P < 0.05 for a standard normal deviate P"Overall 0« 0/SE 40-4950-5960-69a70Tumor 187238243100610249750109760851418062752%6832315511342342430701022282812712987138810221736Excluded 58718677183942453224325185413836% 182226240.5466341.0088120.5685960.09246016unique 859)Nodel survival model (n = statusN,-3 0.01N,* 0.47 2.65 differentiationWell 0.0001TNM 1.17 6.74 moderatePoorTumor or stageII 0.02III 0.41 2.31 necrosisAbsent/minimalMarkedHistological 0.0001IV 1.14 5.12 0.0001Log, 2.06 6.89 0.0001Necrosis [ER] -0.21 5.56 typeInfiltrative 0.001Postrecurrence 0.64 3.57 369)Log, survival model (n = ductalInfiltrative <0.0001Nodal [ER] -0.23 6.08 lobularOthersTumor statusN,_j (cm)<22-5>5n582277266474952436528820625560491 size 0.005N.,» 0.52 2.83 <0.0001Necrosis 0.86 4.80 0.02" + 0.43 2.37 Estimated regression coefficient for each level of the covariate. " xj for proportions. Global x2 statistic that tests that all /3s = 0. 5566 Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1988 American Association for Cancer Research. SURVIVAL MODEL FOR BREAST CANCER Fig. 1 depicts the fitted statistical model which predicts the probability of 5-year survival of an individual breast cancer patient with a particular combination of the above four param eters. The model permits prediction for any discrete time after diagnosis. We chose the 5-year mark for illustration because the 95% confidence intervals of estimates at this time were relatively small, 5-year survival is of clinical interest and allows comparison with other reports. A counterbalance of the effects of these covariates on survival can be seen. For example, a particular patient with TNM I, N4+, ER = 400 fmol/mg and no tumor necrosis is predicted to have similar survival to another with TNM I who has N0, but ER = 1 fmol/mg and no tumor necrosis. Thus "high risk" according to nodal status or TNM stage can be attenuated by the presence of high ER concentration. The proportional ben efit of high ER generally increases with increasing risk due to other factors (Fig. 2). A hazard index was calculated for each patient by log-linear substitution of the obtained coefficients and covariate values. For example a patient with NI_J, TNM II, log,.|I-'.K| = 3, and no necrosis would have a hazard index equal to: exp [0.47 + 0.41 + (-0.21)(3) + 0] = 1.28 Partition levels were set for even cut points after preliminary examination of the data and four risk groups were formed. The Kaplan-Meier plots of the observed survival represent the four risk groups formed from the 859 patients grouped according to a given range of hazard index (Fig. 3); the differences between TNM II 100 r r B TNM III TNM IV "A /VV» ïïf !!• iff"/'//,"//ii; Õ« 80 j Õ.40 I il 20 Fig. 1. Predicted 5-year overall survival by simultaneous effects of nodal status, TNM stage, ER concentration, and tumor necrosis. The pairs of Lines A, B, and C designate patients with axillary' nodal status No, NT .. and N4.. respectively. The upper of each pair designates absent or minimal tumor necrosis and the lower designates marked tumor necrosis. Four ER concentrations (1, 7. ISO, and 400 fmol/mg), the break points on each line from lowest to highest, were arbitrarily chosen to represent a wide range. For example: patients with TNM I, N, . (group B), marked tumor necrosis (the lower solid line of group B), and ER s l (lowest point on this line) would be expected to have a 5-year survival of about 60%, which is a little less than those patients with TNM III, N4» (group C), minimal tumor necrosis (the upper dashed line of group C), and ER = 400 (highest point on this line). 100 80 5«60 ~ô > .1 40 Predicted1 20 123456789 1 l l l l l 1•• Years Fig. 3. General model Tit: observed survival versus predicted survival as a function of hazard index level. Each of the predicted curves represents the mean hazard value for that category; for example, the upper curve represents a hazard index of 0.62, which is the mean for the "<l" subgroup. The curves were discontinued when fewer than 10 patients remained at risk in the observed survival group. them were highly significant (P < 0.0001). The following 5year survival was observed in each subgroup: (a) hazard index <1 (n = 366): 91%; (*) hazard index = 1.00-1.99 (n = 256): 79%; (c) hazard index = 2.00-2.99 (n = 97): 65%; (d) hazard index>3(/i= 140): 43%. The goodness of fit of the model was tested graphically by comparison of the observed survival curves defined by hazard indices with predicted survival curves (Fig. 3). The latter curves are Kaplan-Meier plots of the expected survival, as predicted from the model, of any patient with a hazard index that is the mean value of the corresponding range. If the derived model is an accurate reflection of true survival experience of a large group of breast cancer patients, then these predicted survival curves (assuming the mean of a given range is its most repre sentative value) should be reasonably close to the observed curves. The most desirable test of this model would, of course, be a prospective analysis of an independent group. The basic proportionality assumption of the Cox model states that the relationship between the underlying hazard function and the covariates is multiplicative as shown in Equation A. This was supported by nearly constant differences of the log (—logsurvival) curves between strata of a covariate, specified at the mean of the other covariates (data not shown) (12, 13). Furthermore, interaction terms composed of the cross-products among all terms in the model were tested when the main factors (nodal status, TNM stage, ER, and necrosis) were in the model. None of the interaction terms contributed significantly to the prediction, indicating that the effect of one covariate does not depend on the value of another. A model consisting of only three covariates was found to best explain variation in survival after first recurrence (Table 2). These covariates, in order of decreasing importance, were ER concentration in the primary tumor, pathological nodal status at the time of primary diagnosis, and tumor necrosis (Fig. 4). DISCUSSION TNM I TNM TNM TNM IV Fig. 2. Relative gain in predicted 5-year survival as a consequence of high ER concentration (400 fmol/mg) compared to negative ER (l fmol/mg), in cases with no necrosis. A multivariate approach was used in this study to identify relevant and independent factors measurable at diagnosis that could be used to model risk of breast cancer mortality. Four such factors emerged as the best combination; in descending order of importance they were: number of involved axillary nodes, TNM stage, ER concentration, and extent of tumor 5567 Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1988 American Association for Cancer Research. SURVIVAL MODEL FOR BREAST CANCER lOOr N0 N13 80 60 40 20 Fig. 4. Predicted 5-year postrecurrence survival by simultaneous effects of ER concentration, nodal status, and tumor necrosis. The upper of each pair designates absent or minimal tumor necrosis and the lower designates marked tumor necro sis. Four ER concentrations (1, 7, ISO, and 400 fmol/mg), the break points on each line from lowest to highest, were arbitrarily chosen to represent a wide range. necrosis. The incorporation of these factors in the final model obviated the prognostic information provided by other covariates we studied, since the effect of other factors has already been explained by one or more of the chosen covariates. The Cox proportional hazards model has been used by others to correlate predictive factors and survival with breast cancer. The prognostic usefulness of ER status in addition to tumor stage, axillary node metastasis, and histopathological grade has been reported (14). Russo et al. (15) showed improved survival predictions when nodal status, tumor size, and grade and ER status were combined. Haybittle et al. (16) found that the inclusion of tumor grade or ER status in a similar model was mutually exclusive, such that omission of either factor in the analysis permitted the inclusion of the other. Our prediction model was based on a large number of patients with long followup, and we studied the quantitative effects of ER together with its strong correlates such as tumor differentiation and tumor necrosis. We observed that the effect of tumor differentiation was overwhelmed when examined in this context. There is firm agreement among studies pointing to axillary nodal involvement as the single most important predictor (17). In many treatment protocols métastasesin axillary nodes war rant the institution of systemic adjuvant therapy. However, considerable prognostic heterogeneity within nodal categories may result in overtreatment when the sole criterion for adjuvant therapy is the presence of lymph node métastases(18). Adjuvant therapy is clearly indicated in patients who are considered high risk, but there is a need to agree upon the definition of high risk (19). It is evident from this study that high risk is a composite of characteristics. Despite the inherent unreliability of clinical assessment of regional lymph node involvement (20) TNM stage was found to be independently important in con veying the severity of this risk. There is general consensus on the clinical importance of ER status of the primary tumor, and we have shown that there is a quantitative relationship with prognosis (21). Survival predictions based on this model suggest that the more ER present in the primary tumor, the greater the prog nostic improvement in patients with dire features of advanced stage disease. Therefore a high-risk patient, by the criterion of advanced TNM stage or node positivity, may be considered to have reduced her risk by virtue of high ER concentration in the tumor. It is possible that there is an ER threshold beyond which there is a weaker or no influence on survival. However, when patients were grouped according to ER in the high range, i.e., >250 fmol/mg, there was clear survival advantage to the higher ER levels. Thus if such a threshold does exist it would occur in the very high positive range. The positive influence of high ER concentration was also expressed as a reduced risk of death after disease recurrence. This favorable effect was not dependent on the mode of systemic therapy (22), but appears to be an independent manifestation of the generally better differentiation (23) and slower growth rate of these tumors (24). Although not commonly emphasized, the aggressive nature of tumors with marked necrosis was reported by Fisher et al. (25) some time ago. They found that the presence of necrosis influenced treatment failure independent of pathological nodal status, tumor size, and histológica! grade. We found that tumor necrosis was the only histopathological feature of the primary tumor with enduring biological influence beyond recurrence. A hazard index is a convenient measure of the summed risk estimate for a patient with a particular set of predictors. The concept of one covariate compensating for the hazardous effect of the others may be illustrated with this index. Each of the four hazard categories in Fig. 4 is defined by a range of hazard index values. Patients who have different patterns of the four covariates may have the same hazard index and hence be considered to have the same degree of risk. We believe that the four factors identified in this study represent different aspects of the complex interactions between host and tumor and reflect biologically significant characteris tics of breast cancer, although the underlying precise mecha nisms remain speculative. The presenting TNM stage indicates the anatomical progression of the disease, as well as signals a permissive environment that allows full expression of tumor invasive properties. The host may also provide facilitative con ditions for tumor expression of metastatic properties, such as changes in cell surface chemistry associated with loss of cell adhesiveness (26), increased tumor cell mot ¡lily,and production of active proteolytic enzymes that render basement membranes defective (27). These are some features of biologically aggressive tumors that predispose to involvement of axillary nodes. They do not appear to be a function of time (28). Greater malignancy of ER- tumors is consistent with their increased secretion of autocrine and paracrine growth factors such as insulin-like growth factor, transforming growth factors (a and ß),and a competence factor (29). In addition, there is a link among growth factors, steroid hormones, and their receptors and on cogene products (30). Vascular insufficiency, as one result of rapid tumor growth rate, is a possible cause of tumor necrosis. This hypothesis is consistent with the significant associations found between tumor necrosis and ploidy or the mean fraction of cells engaged in DNA synthesis (24). The ascertainment of pathological nodal involvement, TNM stage, ER concentration, and tumor necrosis is feasible at primary diagnosis. Assessment of just these four parameters appears to enable fairly accurate prediction of the long-term outlook for individual patients. This in turn allows the clinician to recognize the heterogeneous prognoses of patients at any presentation stage of disease, and may help in the selection of specific therapies, design of overall treatment strategies (31), and more uniform stratification for trials. 5568 Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1988 American Association for Cancer Research. SURVIVAL MODEL FOR BREAST CANCER REFERENCES 1. r cui iman. I. S., Cuzick. J.. Millis. R. R., and Hayward, J. L. Which patients are cured of breast cancer? Br. Med. J., 289: 1108-1111, 1984. 2. Breslow, N. E. Analysis of survival data under the proportional hazards model. Int. Stat. Rev., 43:45-58. 1975. 3. Elwood, J. M., and Godolphin, W. Oestrogen receptors in breast tumors: associations with age. menopausal status and epidemiológica! and clinical features in 735 patients. Br. J. Cancer, 42/635-644. 1980. 4. Jacobson, B. E. Investigation of estrogen receptor protein in human mammar)' carcinoma for the establishment of a routine clinical assay. Can. J. Med. Technol., 43: 17-33, 1981. 5. Godolphin, W., and Jacobson, B. E. Quality control of estrogen receptor assays. J. Immunoassay, /: 363-374. 1980. 6. EORTC Breast Co-operative Group. Revision of the standards for the as sessment of hormone receptors in human breast cancer; report of the second EORTC workshop, held on 16-17 March, 1979. in the Netherlands Cancer Institute. Eur. J. Cancer, 16: 1513-1515, 1980. 7. Cox, D. R. Regression models and life-tables. J. R. Stat. Soc., B34:187-202, 1972. 8. Lee, E. T. Statistical Methods for Survival Data Analysis. Belmont, NY: Lifetime Learning Publications, 1980. 9. Epilog Version 3. Pasadena, CA: Epicenter Software, 1986. 10. Thomas, D. C. Program "Risk" User's Manual. Montreal: McGill University. 11. 12. 13. 14. 15. 16. 17. 18. 1980. Dixon, W. J. (chief ed.). BMDP Statistical Software. Berkeley, CA: Univer sity of California Press, 1983. Kay, R. Proportional hazard regression models and the analysis of censored survival data. Appi. Statist., 26: 227-237, 1977. Kalbfleisch, J. D., and Prentice, R. L. The Statistical Analysis of Failure Time Data. New York: John Wiley & Sons. Inc.. 1980. Pari. F. F., Schmidt. B. P.. Dupont. W. D., and Wagner, R. K. Prognostic significance of estrogen receptor status in breast cancer in relation to tumor stage, axillary node metastasis, and histopathologic grading. Cancer (Phila.), 54:2237-2242, 1984. Russo, J., Frederick, J., Ownby, H. E., Fine, G., Hussain, M., Krickstein, H. I., Robbins, T. O.. and Rosenberg. B. Predictors of recurrence and survival of patients with breast cancer. Am. J. Clin. Pathol.. 88: 123-131, 1987. Haybittle. J. L., Blarney. R. W., Elston. C. W.. Johnson, J., Doyle, P. J., Campbell, F. C., Nicholson, R. I., and Griffiths, K. A prognostic index in primary breast cancer. Br. J. Cancer, 45: 361-366, 1982. Fisher, E. R., Sass. R., Fisher, B., and Collaborating NSABP Investigators. Pathologic findings from the National Surgical Adjuvant Project for Breast Cancers (protocol no. 4). X. Discriminants for tenth year treatment failure. Cancer (Phila.), 53: 712-723, 1984. van der Linden. H. C., Baak, J. P. A., Lindeman, J., Hermans, J., and Meyer, C. J. L. M. Morphometry and breast cancer. II. Characterisation of breast 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. cancer cells with high malignant potential in patients with spread to lymph nodes: preliminary results. J. Clin. Pathol.. 39: 603-609. 1986. Cascinelli, N.. Greco, M., Bufalino, R., Clemente, C., Galluzzo. D., Delle Donne, V., De Lellis, R., Sacchini, V., and Veronesi. U. Prognosis of breast cancer with axillary node métastasesafter surgical treatment only. Eur. J. Cancer Clin. Oncol.. 23: 795-799, 1987. Coppin, C. M. L., and Swenerton, K. D. Prognostic factors and predictors of response in breast cancer. Rev. Endocr. Relat. Cancer, 15: 23-29, 1983. Godolphin, W., Elwood, J. M.. and Spinelli. J. J. Estrogen receptor quantitation and staging as complementary' prognostic indicators in breast cancer: a study of 583 patients. Int. J. Cancer, 28: 677-683, 1981. Shek, L. L. M., Godolphin, W., and Spinelli, J. J. Oestrogen receptors, nodes and stage as predictors of post-recurrence survival in 457 breast cancer patients. Br. J. Cancer. Ji: 825-829, 1987. Fisher, E. R., Osborne, C. K., McGuire, W. L., Redmond, C., Knight, W. A., Fisher, B., Bannayan, G., Walder, A., Gregory, E. J., Jacobsen, A., Queen, D. M., Bennett, D. E., and Ford, H. C. Correlation of primary breast cancer histopathology and estrogen receptor content. Breast Cancer Res. Treat../: 37-42, 1981. McDivitt, R. W., Stone, K. R., Craig, R. B., Palmer, J. O., Meyer, J. S., and Bauer, W. C. A proposed classification of breast cancer based on kinetic information derived from a comparison of risk factors in 168 primary operable breast cancers. Cancer (Phila.), 57: 269-276, 1986. Fisher, E. R., Palekar, A. S., Gregorio, R. M., Redmond, C., and Fisher, B. Pathological findings from the National Surgical Adjuvant Breast Project (protocol no. 4), IV. Significance of tumor necrosis. Hum. Pathol., 9: 523530, 1978. Kim, L1.Possible avenues for the control of metastatic behaviour in breast cancer. In: V. P. Hollander (ed.). Hormonally Responsive Tumors, pp. 288317. Orlando, FL: Academic Press, Inc., 1985. Liotta. L. A. Tumor invasion and métastases:role of the basement membrane. Am. J. Pathol.. 117: 339-348, 1984. Bonadonna, G., and Valagussa. P. Chemotherapy of breast cancer: current views and results. Int. J. Radial. Oncol. Biol. Phys., 9: 279-297, 1983. Lippman, M. E., Dickson, R. B., Kasid, A., Gelmann, E.. Davidson, N., McManaway, M., Huff, K., Bronzert, D., Bates, S.. Swain, S., and Knabbe, C. Autocrine and paracrine growth regulation of human breast cancer. J. Steroid Biochem., 24: 147-154, 1986. Saez, S. Steroids, growth factors and oncogenes in breast cancer. In: F. Cavalli (ed.). Endocrine Therapy of Breast Cancer: Concepts and Strategies. Berlin: Springer-Verlag, I986. McGuire, W. L., Clark, G. M.. Fisher, E. R., and Henderson. J. C. Predicting recurrence and survival in breast cancer. Breast Cancer Res. Treat., 9: 2738, 1987. Byar, D. P. Analysis of survival data—Cox and Weibull models with covariates. In: V. Mike and K. E. Stanley (eds.). Statistics in Medical Research, pp. 365-401. New York: John Wiley & Sons. Inc., 1982. 5569 Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1988 American Association for Cancer Research. Model for Breast Cancer Survival: Relative Prognostic Roles of Axillary Nodal Status, TNM Stage, Estrogen Receptor Concentration, and Tumor Necrosis Lydia L. M. Shek and William Godolphin Cancer Res 1988;48:5565-5569. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/48/19/5565 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1988 American Association for Cancer Research.