Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Normal Anatomy and Imaging
Stations
Medical Univ. of
South Carolina
Digestive Disease Center
Dr. Ian Penman
and Dr. David Williams
Normal Anatomy and
Imaging Stations
• Ultrasonography is a dynamic process and it
is difficult to capture all the relevant
information from a study on a few still
images. Slides 1- 33, however, demonstrate
examples of normal anatomy and the
important landmarks to identify while
performing endosongraphy.
Mediastinum
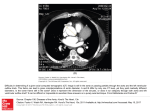
Mediastinum - main bronchi
The mediastinum is usually imaged by slow
withdrawal of the echoendoscope from the gastroesophageal junction. In this image, at 27cm from the
incisors, the left and right mainstem bronchi are seen
anteriorly at the 12 o’clock position, with the aorta and
spine posteriorly. Inserting the probe 1-2 cm will bring
the subcarina into view and it is important to inspect
this area carefully for the presence of subcarinal
lymphadenopathy (level VII).
Mediastinum - aortic arch
Upon withdrawing the echoendoscope 2-3cm from the
subcarina, the two main bronchi will merge to form
the trachea (T) and the aorta will be seen to elongate
as it arches. The area between the transducer and the
aortic arch is the aortopulmonary window (level V)
and must also be examined closely for the presence of
enlarged lymph nodes. This image was taken at 25cm
from the incisors.
Esophagus and stomach
Esophageal wall
Catheter probe image (20MHz) showing normal
esophageal wall layers. The first layer consists of a
hyperechoic interface between lumen and mucosa,
beneath which a hypoechoic layer corresponding to
mucosa can be seen (2). The submucosa appears
hyperechoic (3), while the muscularis can be seen as
inner circular and outer longitudinal layers (4 & 5).
Anatomy - gastro-esophageal junction
Radial image at the level of the gastro-oesophageal
junction, showing aorta and IVC as it runs through the
liver.
Gastric wall layers
Radial image of the water-filled stomach at 7.5MHz.
The 5 layer structure can clearly be seen.
Left adrenal gland
Left adrenal gland
The left adrenal gland (arrow) can often be seen lying
between the superior pole of the left kidney and the
aorta, just proximal to the celiac axis. It appears as a
thin triangular or "seagull"- shaped hypoechoic
structure. The right adrenal is not usually seen at EUS.
Celiac axis
Celiac axis
The celiac axis is usually best scanned from just inside
the GE junction, where it can be identified as it arises
anteriorly from the aorta. It bifurcates into hepatic and
splenic artery, an appearance often described as the
"whale’s tail". It is important to scan carefully in this
region for evidence of celiac LN involvement in
patients with malignancy
Celiac axis
The celiac axis is also easily identified using curved
linear array echoendoscopes, by following the aorta
distally from the GE junction. The SMA is also clearly
seen in this image.
Pancreas - body and tail
Pancreas - body
The pancreas lies between the splenic artery running
along its superior border and the splenic vein inferiorly.
This image shows a normal, homogeneous pasncreatic
echotexture and a portion of the main PD can be seen
at the genu. The confluence of the splenic and superior
mesenteric veins ("clubhead") is also seen.
Pancreas - body
It is important to trace the main PD as it runs
proximally around the genu of the pancreas ("genu
follow-through"). The SMA can be seen in crosssection, behind the splenoportal confluence and neck
of pancreas.
Pancreas - genu
The pancreatic parenchyma is homogeneous, the main
PD is regular and the duct margins are not hyperechoic,
as is often the case in chronic pancreatitis. Note the
"genu follow-through" as the PD turns round the genu.
Confluence of splenic and superior mesenteric
veins
This image demonstrates the "clubhead" sign formed
by the confluence of SV and SMV. Note also the SMA
in cross-section, lying posterior to the confluence.
Pancreas - tail
Because the pancreatic tail lies more cephalad than the
pancreatic head, it is necessary to withdraw the
transducer slowly while rotating slightly to the
patient’s left in order to follow the pancreas out
towards the tail. This can be seen close to the splenic
hilum , which is at the bottom right of the image.
Biliary tree & pancreatic head
Distal CBD and PD
Scanning from the apex of the duodenal bulb , it is
possible to trace the CBD distally as it runs down to
the ampulla. Behind this the main PD can also be seen
Apical view
In this image, the CBD and portal vein can be seen in
long view. The gallbladder contains considerable
sludge. The muscularis of the duodenal wall can also
be seen (arrow).
Apical view
This image, from the apex of the duodenal bulb,
shows a long view of the CBD and a portion of the
portal vein behind it. A periampullary diverticulum
(D) is also seen . This may impede adequate
visualisation of the ampullary segment of the CBD.
The portal vein is usually larger in calibre than the
CBD and lies caudal to the CBD. It is seen best by
insertion of the echoendoscope slightly beyond the
CBD.
"Stack sign"
In 70-80% of patients it is possible to visualise the
CBD, PD and PV in the same echo plane, from the
duodenal bulb. This is referred to as the "stack sign"
and is an important landmark as it ensures that the
echo plane is passing through the pancreatic head,
distal CBD and portal vein - making it less likely to
miss small lesions in this area.
Gallbladder
The gallbladder is usually best seen from the gastric
antrum or, less often, the duodenal apex. The
echogenic wall consists of 3 layes. It is important to
scan carefully over the gallbladder to look for calculi
(with acoustic shadowing), sludge or hyperechoic
‘floaters’.
Pancreas - uncinate and ampulla of Vater
Ampulla
Good visualisation of the ampulla may be difficult to
obtain. It is often best seen by inserting the endoscope
into the second or third part of duodenum, then slowly
withdrawing. The uncinate process will come into
view and then, with further withdrawal of the probe,
the ampullary region. This image shows both PD and
CBD in cross-section through the ampulla
Ampulla
This image demonstrates a slightly thickened but
otherwise normal ampullary sphincter around the
distal CBD (arrow).
Pancreas - ventral anlage
The ventral portion of the pancreas (V) contains
relatively less fat than the larger dorsal portion (D) and
therefore appears darker on EUS. This appearance is
seen in up to 75% of normal people and should not be
mistaken for a mass. It is seen upon withdrawing the
probe proximally through the duodenal sweep. This
distinctive pattern may be lost in patients with chronic
pancreatitis or pancreatic cancer, when it is seen in
40% approximately
Anatomy - distal duodenum
By placing the transducer in the duodenal sweep
beyond the ampulla, a longitudinal view of the aorta
can be obtained as well as the SMA arising from it.
Pancreas - uncinate process
As the scope is withdrawn the aorta will ‘round up’
and the uncinate process of the pancreas will come
into view. The SMA will also appear in cross section
and, lateral to this, a portion of SMV can be seen.
Upon further withdrawal, the splenoportal confluence
("clubhead" view) will appear (see slides 3.12 and
3.13).
Rectum and anal canal
Rectum
As well as rectal wall layers, it is possible to identify
seminal vesicles (SV) which appear as tortuous, paired
hypoechoic structures on either side of the bladder
base. Orientation of structures is best performed by
rotating the image until the bladder (B) lies at the 12
o’clock position.
Prostate gland
The prostate is seen inferior to the bladder base. This
image shows a normal-looking prostate (Pr). In
asymptomatic, elderly men, calcification within the
gland is often noted.
Endoanal ultrasound - puborectalis
On withdrawing the probe through the anal canal, the
puborectalis sling, extenal anal sphincter and internal anal
sphincter progressively come into view. The puborectalis sling
of the levator ani muscle is seen in this image as a hyperechoic
(striated muscle) sling running anteroposteriorly around the
upper anal canal (arrows). The external anal sphincter, also
composed of striated muscle, is hyperechoic and separates into
three distinct bands in the lower canal. The internal anal
sphincter (smooth muscle) is seen as a concentric 2-3mm
hypoechoic zone internal to the external sphincter and visible
in the lower 2cm of the anal canal.
Endoanal ultrasound - anal sphincters
This image (B&K rigid rectal probe) shows normal
internal (hypoechoic concentric ring) and external
(hyperechoic) anal sphincters.
Endoanal ultrasound - anal sphincters
In contrast, this image (B&K rigid rectal probe) shows
a large, wedge-shaped anterior defect involving both
sphincters (arrow), in a middle-aged woman with a
history of obstetric trauma and fecal incontinence
Thank you