Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
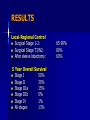
Role of Radiation in Lung Cancer Eyad Alsaeed MD , FRCPC Consultant Radiation Oncology Prince Sultan Hematology Oncology Center KFMC Epidemiology Cancer is a leading cause of death worldwide: it accounted for 7.9 million deaths (around 13% of all deaths) in 2007 making it the number one cancer killer in both men and women worldwide. Exceeding the combined mortality of breast , ovarian , cervical cancer for women. Prostate cancer for men. IN KSA In 2002 lung and bronchial cancer were the third leading cause of death in men . tenth leading cause of death in women. Cancer Incidence for Most Common Sites (2004) Cancer Male Female All % Breast 15 783 798 11.5 CRC 366 281 647 9.3 NHL 332 224 556 8.0 Leukemia 241 194 435 6.2 Thyroid 87 328 415 6.0 Liver 231 93 324 4.6 Lung 233 63 296 4.2 HD 166 98 264 3.8 Skin 136 125 261 3.7 Brain, CNS 147 100 247 3.5 Prostate 214 - 214 3.1 Stomach 141 70 211 3.0 Bladder 160 41 201 2.9 Uterus - 117 117 1.7 Ovaries - 108 108 1.5 All Others 1009 866 1875 26.9 Total 3478 3491 6960 100 Risk Factors Cigarette responsible about 80% of lung cancer&100% SCLC Radon gas the second cause Lung cancer occupational exposure Asbestos Nickel Chromium Arsenic Radon naturally occurring inert gas & decay product of Uranium-238 particularly found in stone houses daughter products emit particles, delivering radiation to depth = 41-71 m RR 1.3-1.8 7 Since 1970 the prevalence of smoking has increased in Saudi Arabia, as in the rest of the world, and this will likely lead to a lung cancer epidemic in the coming decades Presenting Symptoms 1.Local cough, Dyspnea , hemoptysis, pleuritic pain 2.Nodal recurrent laryngeal/ phrenic, SVCO, esophageal compression 3.Distant bony pains, brain mets 4. Nonspecific, initial symptoms such as weight loss, weakness, anorexia, and malaise 5.Paraneoplastic LUNG CANCER paraneoplastic syndromes: (2%) Hypercalcemia (ectopic parathyroid hormone,more common in SCC,mental status changes, hypotension Cushing's Syndrome (2% of SCLC,ectopic ACTH secretion,HTN,hirsutism,moon face,buffalo hump,truncal obesity,thin skin,bruising, abdominal striae.poor prognosis SIADH (10% of SCLC.ectopic ADH secretion. hyponatremia. Seizures) not affect the prognosis Eaton-Lambert Syndrome (impaired release of acetylcholine ,muscle strength improves with repetitive movement,SCLC Pulmonary Hypertrophic Osteoarthropathy (common in Adenoca, periosteal inflammation causing bone and joint pain (usually in knees or ankles), tibial tenderness,digit clubbing, elevating alk phos,x-ray -periosteal inflammation and elevation,bone scan -- intense generalized increased uptake, especially in long bones Peripheral Neuropathy Polymyositis Dermatomyositis Digit Clubbing DIC VIPOMA (flushing, diarrhea, hypotension = carcinoid syndrome Gynecomastia 2% of SCLC INVESTIGATION 1- Sputum cytology ( 3 samples , can diagnos central lesion 80%) < 20% in small peripheral lesion 2- FNA : 90% accuracy 3-CT chest , abdomen ( s/s 70%) MRI( if CT reveal uncerain medistinal or vertebral) 4- Bronchoscopy 5- Mediastinoscopy 6- VAT 7- Staging work up (brain , bone) PFT for Radical RT Consensus conference in Cambridge: FEV1 ≥ 40% FVC ≥ 45% DLCO ≥ 45% pO2 ≥ 60 mmHg pCO2 < 50mmHG O2 sat. ≥ 90% 12 contraindications to curative large field RT – pt on home O2 with such poor pulmonary function from benign lung dz that life expectancy is < 6 mo 7/7/2017 Prognostic Factors Most important are PS, extent, and weight loss. Host: PS, weight loss*, sex Tumor Histo: no difference for advanced disease. extent Treatment: operability, radiation dose, high dose cisplatinum. PATHOLOGY WHO Classification I. Benign II. Dysplasia and CIS III. Malignant 1. Squamous cell carcinoma 30% – and spindle cell carcinoma 2. Small cell carcinoma 18% – 1.Oat cell 3.Combined cell 3. Adenocarcinoma 40% – 1.Acinar 2.Intermediate cell 2.Papillary 3.Bronchoalveolar 4.Mucus secreting 4. Large cell carcinoma 15% – 1.Giant cell 2.Clear cell Others 5. Combined epidermoid + adenocarcinoma 6. Carcinoid 7. Bronchial gland (cylindroma, mucoepidermoid, others) 8. Papillary tumors of surface epithelium 9. Mixed tumors and carcinomas (carcinosarcomas, etc.) 10. Sarcomas 11. Unclassified 12. Mesotheliomas (A.localized, B.diffuse) Up to 45% contain 2 histologic patterns. SCLC STAGING LIMITED DISEASE 30% EXTENSIVE DISEASE 70% SCLC: Staging Limited disease (LD) – Confined to one hemithorax and regional lymph nodes, including ipsilateral supraclavicular lymph nodes Extensive disease (ED) – Extends beyond one hemithorax or involves contralateral mediastinal, hilar, or supraclavicular lymph nodes, and/or pleural effusion with positive cytology Ihde et al. In: DeVita et al, eds. Cancer: Principles & Practice of Oncology. 5th ed. Lippincott-Raven; 1997:911-949. SCLC Stage Distribution at Diagnosis LD: approximately 30–40% of patients . Most patients with 2-year disease-free survival come from this group ED: approximately 60–70% of patients. Common sites of metastasis include: – Bone, 19–38% – Liver, 17–34% – Bone marrow, 17–23% – Brain, 0–14% – Lymph nodes, 7–25% – Soft tissue, 3–11% SCLC Stage Distribution at Diagnosis: 1989–1996 80 Percentage of Patients 70 60 64% 62% 61% 50 Localized Regional Distant Unstaged 40 30 20 18% 10 13% 7% 20% 17% 7% 12% 13% 6% 0 Total Males Females Data from Ries et al, eds. SEER Cancer Statistics Review, 1973-1997. National Cancer Institute; 2000. Importance of XRT in SCLC Chemotherapy vs Chemotherapy + RT • JP Pignon, et al. NEJM. 327:1618-1624, 1992. - meta-analysis – 2,103 pt with limited stage SCLC from 13 randomized trials comparing chemo alone to chemo + RT – end-point: survival – RR of death with addition of RT = 0.86 – administration of thoracic RT produced a 14% reduction in the mortality rate – conclusions : • (1) limited stage SCLC, addition of thoracic RT produced a 14% reduction in mortality rate, corresponding to a 5% greater 3-yr survival • (2)benefit of radiation was greatest in pt < 55 yr 3-yr OS rate pt age chemo alone chemo + RT all pt 10% 15% < 55 yr 9% 17% > 70 yr 10% 9% Importance of XRT in SCLC Chemotherapy vs Chemotherapy + RT not only survival but also Local control • P Warde, et al. J Clin Onc. 10:890-895, 1992. - meta-analysis chemo chemo + RT 2-yr LR rate 77% 52% 2-yr OS rate 16% 23% −1,911 pt with limited stage SCLC from 11 randomized trials −end-points: survival, loco-regional control, toxicity −odds of surviving 2 yr with RT vs without RT = 1.53 −overall increase in 2-yr survival = 5.4% (p<0.05) −odds of thoracic failure at 2 yr with RT vs without RT = 3.02 −overall increase in 2-yr thoracic control = 25.3% (p<0.05) −conclusions :addition of thoracic RT to chemotherapy produces a modest improvement in survival and a large improvement in intrathoracic control in pts with limited stage SCLC 20 Common Treatment Approach Extensive Disease Standard regimens for SCLC are considered to be CAV or EP, or CAV/EP alternating regimen. + Prophylactic Cranial Irradiation Limited Disease Same chemotherapy + Concurrent Thoracic Radiotherapy + Prophylactic Cranial Irradiation Timing of Chemo/RT 1- N Murray, et al. J Clin Onc. 11:336-344, 1993. - NCI RCT RT - 2nd cycle (n=155) RT - 6th cycle (n=153) p-value CR rate 64% 56% NS median PFS 15 mo 12 mo 0.036 3-yr PFS rate 26% 19% 0.036 median survival 21 mo 16 mo 0.008 3-yr OS rate 30% 21% 0.006 5-yr OS rate 20% 11% 0.006 3-yr LR rate >50% >50% NS randomization: (1) early RT = radiation given concurrently with 2nd cycle of chemotherapy (2) late RT = radiation given concurrently with 6th cycle of chemotherapy conclusions :early thoracic irradiation improves progressionfree survival and overall survival 22 - Pre-Chemo vs Post-Chemo Volumes Kies, et al. J Clin Onc. 4:592-600, 1987. – SWOG Liengswangwong, et al. J Clin Onc. 12:496-502, 1994. - Mayo Clinic conclusions : use of post-chemo tumor volume did not – increase the risk of marginal recurrence – Improve median survival – Improve median RFS AT Turrisi, et al. NEJM. 1999. - ECOG QD RT = 45 Gy in 1.8 Gy fx qd BID RT = 45 Gy in 1.5 Gy fx bid QD RT BID RT p-value response rate – overall 87% 87% NS CR 49% 56% NS PR 38% 31% NS 19 mo 23 mo 0.04 2-yr OS rate 41% 47% 0.04 5-yr OS rate 16% 26% 0.04 2 yr failure-free survival rate 24% 29% 0.10 local failure rate 52% 36% 0.06 median survival treatment related toxicity QD RT BID RT p-value grade 3-4 myelosuppression 85% 87% NS grade 3 esophagitis (unable to swallow solids, narcotic use, G-tube) 11% 27% 0.001 5% 5% NS 5 pt (2%) 6 pt (3%) NS grade 4 esophagitis (hospitalization or perforation) death 24 PCI – 25Gy/10f R Arriagada1995. - Institut Gustave-Roussy, France PCI (n=145) no PCI (n=149) p-value 2-yr brain met rate 40% 67% < 0.0001 2-yr survival rate 29% 21% NS conclusions = PCI given to those with complete remission after initial therapy significantly decreases the risk of brain mets without increasing neurotoxicity at 2.5 yr, and there is a trend toward improved survival A Gregor, et al. 1997. – UKCCCR/EORTC conclusions : (1)for limited stage SCLC in complete remission after initial therapy, PCI significantly decreases the likelihood of brain relapse (2)higher doses were more effective (no difference in brain met rate was seen with 2400 cGy vs no PCI) 25 PCI- meta-analysis ( LD ) Auperin, R Arriagada, et al. NEJM. 341:476-484, 1999. - Institut Gustave-Roussy, France median f/u = 5.5 yr PCI (n=526) no PCI (n=461) p-value 3-yr OS rate 21% 15% 0.01 3-yr DFS rate 22% 13.5% 0.001 3-yr brain mets rate 33% 59% 0.001 3-yr other mets rate 42% 46% NS 3-yr LRR rate 44% 45% NS conclusions : addition of PCI in pt with limited stage SCLC in complete remission 26 after chemo results in significantly improved 3-yr OS and DFS and 50% reduction in the incidence of brain mets. Prophylactic cranial Irradiation in Extensive Small Cell Lung Cancer ( NEJM ) Inclusion Criteria : Age 18 -75 PS (0 – 2) Documented extensive SCLC before starting CTR Response after 4 – 6 cycle Interval of no more than 5/52 between the last cycle of CT and Radiation No evidence of brain metastases No Hx of Rad to H/N area No Hx of CS use No Previous or other current cancer PCI :2 lateral fields Co , 4 – 18 MV Daily RX / 5 weeks Dose was 20Gy / 5–8 fx 24 Gy / 12 fx 25 Gy/ 10 fx 30 Gy/ 10 –12 fx . Radiation started 4 – 6 weeks after CT Point in the study:End Point : Development of symptomatic brain metastases including : 12345- HA N/V cognitive or affective disturbance Seizures Focal neurological symptoms Role of PCI ?? The role of PCI in patient who do not have complete response to CTR is unclear - Usually they don’t have complete response Results Patient in the irradiation group had a lower risk of symptomatic brain metastases - Cumulative risk of brain metastases within 1 year was : 14.6% in the irradiation group. 40.4% in the control group . - The 1 year survival rate was 27.1% in irradiation group and 13.3% in the control group. - Cumulative Incidence of Symptomatic Brain Metastases . Disease-free Survival Overall Survival Conclusion: PCI reduce the incidence of symptomatic brain met and prolongs DFS + OS Current Standard Regimens for First-Line Therapy LD Cisplatin 60–80 mg/m2 d 1 Etoposide 80–120 mg/m2 d 1-3 Concurrent RT (45–50 Gy) q 3 wk† ED Cisplatin 60–80 mg/m2 d 1 Etoposide 80–120 mg/m2 d 1–3 q 3 wk† or or Carboplatin AUC 6 d 1 Carboplatin AUC 5–6 d 1 Etoposide 80–100 mg/m2 d 1–3 Concurrent RT (45–50 Gy)* q 3 wk‡ Etoposide 80–100 mg/m2 d 1–3 q 3 wk‡ AUC = area under the plasma concentration-versus-time curve. *May be 45 Gy bid. †Turrisi et al. N Engl J Med. 1999;340:265-271. ‡Hainsworth and Greco. Semin Oncol. 1999;26(suppl 2):60-66. Outcomes of First-Line Therapy with Current Standard Options Complete response (%) LD 45-75 ED 10-30 Median survival (mo) 15-23 6-11 2-year survival (%) 20-47 10-20 5-year survival (%) 10-26 1-2 NSLC Staging MX of NSLC 1A : SURGEY alone R/O Rad : 1- Inoperable 2- + ve margin IIA – 2B (T2N0 , T1N1, T2N1 , T3N0) Surgey + Chemotherapy ( CALBG , NCIC,IALT ) R/O Rad : 1- Inoperable 2- + ve margine 3- Nodal ECE DEFINITIONS IIIA (T3 N1 or T1-T3, N2) – N2 = single-digit nodes (station 1-9) Station Station Station Station 7 4 2 5 = subcarinal = low paratracheal = high paratracheal / 6 = AP window (accessible via anterior med.) IIIB (any T, N3 or T4 – N3 = ipsilateral scalene or supraclavicular nodes – T4 = invading major organ or satellite nodule same lobe IIIA : Operable 1- chemo – restage – if no progression – surgery –chemo +/- rad if : 1- + margine 2- nodal ECE 2- Concurrent chemorad ( 45 GY) –restage –if no progression surgery – chemo If progression cont chemorad to (61 Gy) ASTRO 2003 RTOG 9309 NSCLC IIIA, pN2 Cisplatin + VP16 q3wk x 2, concurrent with RT Thoracic RT 45 Gy Surgery RT to 61 Gy 2 additional cycles chemotherapy to both groups RTOG 9309 : NSCLC IIIA, CRT vs CRT + S Surgery No Surgery LF + N + DM 15 % 28 % Median PFS 14 mo 12 mo Median survival 22 mo 22 mo Cancer death 71 % 81 % Treatment death 11 % 2% RTOG 9309 : NSCLC IIIA, CRT vs CRT + S Surgery reduces progression but is associated with more treatment deaths More cancer deaths in no surgery group, despite more chemotherapy Despite significantly improved PFS , surgery did not improve overall survival Longer F/U may demonstrate a benefit Stage IIIA Approximately 20 % of all stage IIIA resectable Different clinical gradations of N2 disease, with differing prognoses: – Easily visible on CXR / CT = “bulky” N2 – Single station enlarged node – Normal CT, only positive at mediastinoscopy – Normal CT, -ve mediastinoscopy, only found at final, post-resection pathology = “incidental” N2 Inoperable IIIA : 1- Concurrent chemorad (63 Gy ) +adjuvant chemo ( RTOG 9410 ) 2- Induction chemo – rad (sequential) 3- Rdaiation alone Option depends on patient , PS , Wt loss. Radiation and Chemotherapy for St III NSCLC CALBG 1990 Arm1 RT 60Gy/30f Arm 11 Vinblastine /CPP x 2 cycles followed by RT 60Gy/30f Interim analysis favored combined modality with median S 13.6 mos vs 9.7 mos Dillman,R NEJM 1990:323,940 Radiation and Chemotherapy for St III NSCLC1 RTOG 88-08 Arm 1 Standard RT 60 Gy/30f Arm 11 Vinblastine/CPP x 2cycles followed by 60 Gy/30f Arm 111 RT bid fractionation 69.6 Gy/1.2 Gy/fraction Results Median S Arm 1---11.4 mo. Arm 11---13.8 mo. Arm111---12.3 mo. Sequential therapy became the standard J. Nat. Cancer Inst.. 1995: 87,3 Concurrent Chemotherapy and Radiotherapy St III RTOG 94-10 SIII,III, KPS> 70, wt loss <5% Arm I VLB/CPP followed by 63 Gy Arm II VLB/CPP concurrent with 63 Gy Arm III Oral VP-16/CPP concurrent with bid RT 69Gy Results Median S Arm I 14.6 mo. Arm II 17 mo. Arm III 15.6 Concurrent therapy has become standard therapy IIIB IF Localized & no pleural effusion As IIIA If pleural effusion or Stage IV PS ( 0-2) Palliative chemotherapy+Rad PS (3-4) Best supportive care RESULTS Local-Regional Control Surgical Stage 1-2: Surgical Stage T3/N2: After sleeve lobectomy: 5 Year Overall Survival Stage I 50% Stage II 30% Stage IIIa 15% Stage IIIb 5% Stage IV 1% All stages 13% 85-90% 80% 60% Survival Curves Lung Cancer 50% 30% 17% 2% Pancoast's syndrome and superior (pulmonary) sulcus tumors PANCOAST Tumors located at the upper part of the pulmonary sulcus near the thoracic inlet may correctly be regarded as superior sulcus tumors, although the inferior margins of the superior sulcus are not well defined. CLINICAL PRESENTATION Lesions in the superior sulcus may result in: shoulder and arm pain (in the distribution of the C8, T1, and T2 dermatomes) Horner's syndrome, and weakness and atrophy of the muscles of the hand, a constellation of symptoms referred to as Pancoast's syndrome . The majority of patients with superior sulcus tumors present with one or more of these complaints. CLINICAL PRESENTATION shoulder and arm pain (in the distribution of the C8, T1, and T2 dermatomes) Horner's syndrome, and weakness and atrophy of the muscles of the hand. What is make it unresectable? Involvement of : 1. Brachial plexus grossly 2. Subclavin artery 3. Vertebral body 4. Esophagus 5. Medistainal L.N 6. Distance Metastasis Induction chemoradiation and surgical resection for non-small cell lung carcinomas of the superior sulcus T3 - T4 N1: SWOG,IG(PhaseII) ROUCH CONCLUSIONS: (1) This combined modality treatment is feasible in a multi-institutional setting. (2) the pathologic complete response rates were high (3) resectability and overall survival were improved compared with historical experience, especially for T4 tumors, which usually have a grim prognosis. 2 y survival 55% Complete resection 70% CR or micro residual 65 % tx related death 3 patients