Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
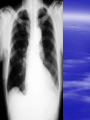
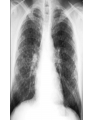
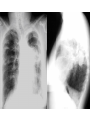
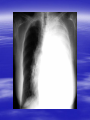
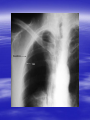
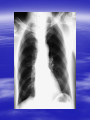
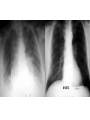
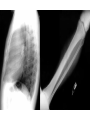
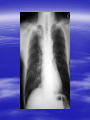
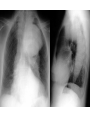
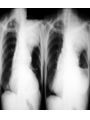
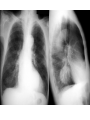
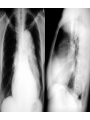
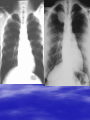
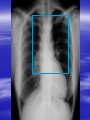
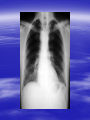
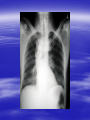
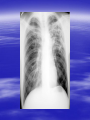
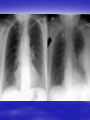
Radiological signs of Disease Air Fluid Levels You can encounter air fluid levels in chest x-rays in the following conditions: Cavitary lung lesions Loculated empyema Hydropneumothorax Esophageal obstruction Mediastinal abscess Hydropneumopericardium Hiatal hernia Chest wall abscess Most disease processes will either increase or decrease the density of the lung parenchyma A mediastinal lesion should have a sharp margin convex towards the lungs and its base abutting the mediastinum . A pleural lesion should be seen as a homogenously dense opacity abutting the pleural surface, without air bronchogram. If the pleural lesion is free fluid, it will gravitate to the dependant lung parts first to form a miniscus (concavity) along its upper surface. An extra pleural lesion demonstrates a homogenous density which makes obtuse angles with the chest wall, or may appear similar to pleural disease. A lung opacity may be due to a mass or lung- parenchymal opacification. Identification of clear margins vs indistinct or diffuse opacification is important in making the differentiation.If the diffuse opacification demonstrates lucencies or air bronchogram within it, it is most likely air space disease (consolidation). Signs of lobar collapse Local increase in density due to nonaerated lung. Decreased lung volume. Displacement of pulmonary fissures. Elevation of hemidiaphragm. Displacement of hila. Pleural effusion + lobar densities Pneumonia with empyema Pulmonary infarction Bronchogenic carcinoma Tuberculosis Pleural effusion + subsegmental atelectasis Postoperative (thoracotomy, splenectomy, renal surgery) secondary to thoracic splinting + small airway mucous plugging Pulmonary infarction Abdominal mass Ascites Rib fractures Upper lung zone distribution Cystic fibrosis Ankylosing spondylitis Sarcoidosis Silicosis Histiocytosis (Langerhan's cell) TB, fungal Radiation pneumonitis ( cancers of head/neck and breast) Peripheral lung zone distribution BOOP (bronchiolitis obliterans organizing pneumonia) UIP (usual interstitial pneumonitis, and DIP desquamative interstitial pneumonitis) Infarcts Eosinophilic pneumonia Alveolar sarcoidosis Contusions 'Bat's wing distribution Acute Chronic * Pulmonary oedema: * Atypical pneumonia - cardiac * Lymphoma/Leukemia - non cardiac * Sarcoidosis: interstitial * Pneumonia: form much more common - often 'unusual' etiology; * Pulmonary alveolar - pneumocystis carinii (AIDS); proteinosis - TB, viral pneumonias; * Alveolar cell carcinoma: - mycoplasma. localised form more common * Pulmonary haemorrhage: - Goodpasture's syndrome; Wegner's and other vasculitides - anticoagulants; - bleeding diathesis: haemophilia, DIC; extensive contusion. LUNG VOLUME *Reduced Idiopathic pulmonary fibrosis. Chronic interstitial pneumonia Asbestosis Collagen vascular disease Chronic pulmonary tuberculosis *Normal Sarcoidosis Histiocytosis *Increased Bronchial Asthma Emphysema Lymphangioleiomyomatosis Reticulations & Hilar Adenopathy - Sarcoidosis Silicosis carcinoma obstuction/spread - Lymphoma/leukemia Lung primary: particulary oat cell Metastases: lymphatic Fungal disease Tuberculosis Viral pneumonia (rare combination) Lung mass of more than Clinical history and patient’s age . Mass borders . Comparison with previous examinations. Presence of calcifications. Associated adjacent rib erosions, pleural effusion, hilar or mediastinal nodal enlargement. Presence of more than one mass. SIGNS OF INTERSTITIAL DISEASE Distribution of opacities Unifocal or multifocal. Lobar. Segmental. Perihilar. Peripheral. Upper, middle or lower zones. Lung fields appear dark because of air. Ninety-nine percent of the lung is air. The pulmonary vasculature, interstitium constitute 1% and give the lacy lung pattern. You have to know what is normal before you can recognize abnormalities. Knowledge of anatomy is essential for this purpose. Which lung is larger? Which diaphragm is higher and why? What is the normal size of the heart? What is the normal size and shape of the aorta? Silhouette sign is extremely useful in localizing lung lesions Silouhette Adjacent lobe/segment Right Diaphragm RLL/Basal segments Right Heart margin RML/Medial segment Ascending Aorta RUL/Anterior segment Aortic knob LUL/Posterior segemnt Left Heart margin Lingula/Inferior segment Descending Aorta LLL/Superior and medial segments Left Diaphragm LLL/Basal segments Hyperlucent Lung Factors – Vasculature: Decrease – Air: Excess – Tissue : Decrease Bilateral diffuse – Emphysema – Asthma Unilateral – – – – – Swyer James syndrome Agenesis of pulmonary artery Absent breast or pectoral muscle Partial airway obstruction Compensatory hyperinflation Localized – Bullae – Westermark's sign : Pulmonary embolus . Honeycombing Seen in end stage lung disease Indicative of diffuse interstitial fibrosis Due to bronchiolectasia Most of the time in bases Upper lobe distribution seen in eosinophilic granuloma Bronchiectasis Normal appearing CXR in most Tubular shadows Tram line Gloved fingers Mucocele Ring shadows with thickened bronchial walls Air fluid levels Watch for dextrocardia – Immotile cilia syndrome Diffuse lung fibrosis – Due to recurrent infections Pulmonary Embolism . The primary purpose of a chest film in suspected PE is to rule out other diagnoses as a cause of dyspnea or hypoxia. Most CXRs in patients with PE are normal.