Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
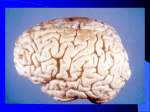
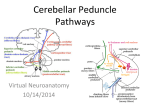
Rhombencephalosynapsis: Review of Cerebellar Embryology, Key Imaging Findings and Associated Anomalies eEdE-175 Abhijit Y. Patil, M.D.* Vinay Kandula, M.D. + Michael Benstock, M.D.# Hemant A. Parmar, M.D.* *Department of Neuroradiology, University of Michigan Health System, Ann Arbor, MI + Nemours/Alfred I. duPont Hospital for Children, Wilmington, DE # Bryn Mawr Hospital, Bryn Mawr, PA Disclosure Authors have no relevant financial disclosures Purpose Rhombencephalosynapsis is a rare congenital malformation characterized by fusion of the cerebellar hemispheres and absence of the cerebellar vermis The exhibit will allow radiologists to: Identify classic features of rhombencephalosynapsis Recognize associated abnormalities such as aqueductal stenosis and other supratentorial anomalies Be familiar with associated syndromes like Gómez-LópezHernández syndrome and VACTERL Improve communication with pediatric neurologist Approach After discussing normal cerebellar development and anatomy, five cases of rhombencephalosynapsis ranging from a newborn to an adult patient are presented to illustrate key imaging findings and associated anomalies The cases include isolated rhombencephalosynapsis as well as cases with associated supratentorial anomalies such as aqueductal stenosis and septo-optic dysplasia Diffusion tensor imaging illustrating cerebellar fusion is shown for one patient Cerebellar Anatomy: Landmarks 1. 2. 3. 4. 5. 6. 7. 8. Quadrigeminal plate Cerebral aqueduct Fourth ventricle Vermis Cerebellar tonsil Pons Tentorium cerebelli Superior medullary velum Cerebellar Anatomy: Landmarks 1. Vermis 2. White matter of cerebellar hemisphere Cerebellar Anatomy: Fissures Primary Fissure (yellow arrow) Horizontal Fissure (blue arrow) Suboccipital Fissure (green arrow) Cerebellar Anatomy: Lobes Anterior Lobe: Anterior to the primary fissure Posterior Lobe: Posterior to the primary fissure Flocculonodular Lobe: Anterior to the posterolateral fissure * Posterolateral fissure Cerebellar Anatomy: Nuclei Dentate Nucleus: Responsible for the planning, initiation and control of voluntary movements. Efferent fibers from this travel through red nucleus to contralateral ventrolateral thalamus Interposed Nucleus*: Consists of globose and emboliform nuclei. Send efferent fibers to contralateral red nucleus. Origin for the rubrospinal tract that mainly influences limb flexor muscles Fastigial Nucleus *: Afferents from vermis. Efferents via inferior cerebellar peduncle to vestibular nuclei Cerebellar Anatomy: Peduncles Superior Cerebellar Peduncle *: Primary output of the cerebellum with mostly fibers carrying information to the midbrain. Most efferent fibers travel in this and arise from dentate nucleus (Tonsil *) Middle Cerebellar Peduncle *: Carry input fibers from the contralateral cerebral cortex. Cortico-pontocerebellar form major fibers (Flocculus*) Inferior Cerebellar Peduncle: Connects the spinal cord and medulla oblongata with the cerebellum. Contain dorsal spinocerebellar tract, olivocerebellar and vestibulocerebellar tracts Afferent fibers are far more numerous that efferent fibers by a ratio of 40:1 Cerebellar Embryology The cerebellum represents a specific development of the alar plate from the rhombic lips of the metencephalon At 50 days, the pontine flexure folds the metencephalon back against the myelencephalon. The rhombic lips of the pontine flexure will give rise to the cerebellum The caudal region of the cerebellar primordia forms the more primitive flocculonodular lobe, whereas the cranial region produces the much larger (and less primitive) vermis and cerebellar hemispheres Rhombencephalosynapsis: Discussion Rhombencephalosynapsis (RES) is a rare midline brain malformation defined by fusion of the cerebellar hemispheres with partial or complete absence of the intervening vermis RES is a rare condition. Approximately 150 cases have been reported in the literature to date RES was first described by Obersteiner in 1914 from a routine autopsy of a 24-year-old male suicide victim RES is probably due to an exaggerated fusion of the two lateral cerebellar primordia. The cause of this exaggerated fusion, associated with a failure of vermian differentiation, is unknown The anomaly is mostly sporadic. Although genetic basis has been suggested based on clinical observations, no single genetic cause has been ascertained Clinical Presentation of RES Clinical presentation is variable due to associated supratentorial anomalies. This may account for the variable age difference at presentation in our cases Wide spectrum of clinical presentation from symptoms such as generalized hypotonia, nystagmus, ataxia, mild to severe mental and motor developmental delays and early death, to a few reported cases diagnosed at a late age without significant associated clinical findings Complete vs. Partial RES Rhombencephalosynapsis can be considered an anomaly with variable degrees of severity as partial RES has been reported in the literature Complete RES: total absence of the vermis with complete fusion of cerebellar hemispheres Partial RES: retained parts of the anterior and posterior vermis including the nodulus, with partly unfused cerebellar hemispheres One of the cases discussed in this review (Case #3) also demonstrated imaging findings suggestive of partial RES, similar to previously reported cases with fused posterior cerebellar hemispheres, unfused hemispheres anteriorly with intervening anterior vermis, presence of primary fissure as well as normal 4th ventricle fastigial recess Partial RES can be explained by an alternative model of cerebellar development that considers RES as a failure of vermian differentiation with undivided development of the cerebellar hemispheres. This model considers cerebellar primordium as an unpaired structure where the posterolateral fissure is formed initially with subsequent development of the posterior vermis before the anterior vermis Imaging Findings of RES: Sagittal Partial or complete absence of vermis Abnormal shape of 4th ventricle * Absent flow void of aqueduct (yellow arrow) Absence of fissures Absent primary fissure (green arrow) Absent suboccipital fissure (red arrow) Hydrocephalus due to aqueductal stenosis * Imaging Findings of RES: Axial Continuity of transverse folia across midline without intervening vermis (red arrow) Continuity or apposition of middle cerebellar peduncles Fusion or apposition of dentate nuclei (blue arrow) Keyhole or teardrop shape of 4th ventricle due to absence of vermis Imaging Findings of RES: Coronal Fusion of inferior colliculli Fusion or approximation of superior cerebellar peduncles Continuity of normal appearing transverse folia across midline without intervening vermis (yellow arrow) Neuropathological studies Total or partial absence of the cerebellar vermis, including its lobules Absent fastigial nuclei Fusion of cerebellar hemispheres across midline without cleft Reduced transverse diameter of the cerebellum Fusion or close approximation of dentate nuclei Nodulus preserved in subtotal rhombencephalosynapsis Present globose and emboliform nuclei Presence of flocculi Neuropathological studies: contd. Absent incisura cerebelli posterior Absent anterior medullary velum Normal appearing major sulci Normally oriented folia that are fused across midline Absence or abnormality of olivary complexes Midline facial anomalies Associated Abnormalities Prognosis and severity of clinical presentation depends on associated supratentorial anomalies Hydrocephalus : most common associated anomaly In majority of cases due to aqueductal stenosis (green arrow) In a study by Ishak et. al., aqueductal stenosis was present in 22 of 42 subjects and was strongly associated with the degree of cerebellar fusion Other less common reported causes of hydrocephalus include: thalamic fusion and obstruction of 4th ventricle by cerebellar tissue Imaging pearl: In patients with aqueductal stenosis, look for presence of RES Associated Abnormalities Absence of septum pellucidum (arrow) 2nd most common associated abnormality Septo-optic dysplasia has been reported Other associated midlines defects such as fusion of fornices have been reported Associated Abnormalities Dysgenesis of corpus callosum (yellow arrow) Can be associated with septal aplasia Other Associated Abnormalities Holoprosencephaly Absent olfactory bulbs Fusion of thalami Neural tube defects Neurocortical dysplasia Associated Syndromes Gómez-López-Hernández syndrome (GLHS) (aka Cerebello-trigeminal-dermal-dysplasia) Craniosynostosis causing tower-like skull Trigeminal anesthesia Rhombencephalosynapsis Bilateral parietal or temporal alopecia Mental retardation, delayed speech Imaging Pearls: Look for rhombencephalosynapsis in cases highly suggestive of GLHS If rhombencephalosynapsis is diagnosed, the clinical signs of GLHS should be sought Associated Syndromes VACTERL association Frequent occurrence of Vertebral anomalies, Anal atresia, Cardiovascular anomalies, Trachea-oesophagEal fistula, Renal anomalies, Limb defects (VACTERL) as associated findings with RES has been reported Case 1: MRI brain at day 1 and CT at 8 months Axial T2WI MR (a) shows transverse folia (red arrow) and fusion of dentate nuclei (blue arrow). Sagittal T2W MR (b) in the same child shows moderate to severe enlargement of the lateral ventricles (*), and to a lesser degree the third ventricle (*). There is stenosis at the cerebral aqueduct (green arrow) , with absence of the normal flow void. The fourth ventricle is normal in size. Absence of the primary fissure (yellow arrow) in a child with Rhombencephalosynapsis (RES). RES is complete in this child. Axial CT (c) also clearly depicts fusion of cerebellar hemispheres (white arrow). Case 2: MRI brain at 2 years of age Sagittal T2W MR (a) shows absence of the primary fissure (yellow arrow) in a child with isolated Rhombencephalosynapsis (RES). Foliation is that of the cerebellar hemisphere as no vermis is present. Note prominent corpus medullare (*). Coronal T2W MR (b) shows transverse folia (red arrow) and interfoliate sulci (green arrow) in the same child. RES is complete in this child. (c) DTI showing transverse fibers across the cerebellar hemispheres (white arrow). Case 3: MRI brain at 9 years of age Coronal T2W MR (a) shows fusion of cerebellar hemispheres posteriorly with continuous transversely oriented folia and fissures extending across the midline (yellow arrow) in a child with partial Rhombencephalosynapsis (RES). Coronal T2W MR (b) shows unfused cerebellar hemispheres anteriorly with intervening anterior vermis (blue arrow). Sagittal T1W MR (c) shows presence of normal primary fissure (green arrow), however, absence of prepyramidal fissure (red arrow). There is normal 4th ventricle fastigial recess (*). Atrophy of corpus callosum (*) as a result of old stroke superimposed on dysgenesis of corpus callosum with associated Wallerian degeneration (white arrow) in brainstem. Case 4: MRI brain at 10 years of age Sagittal T2W MR (a) shows dysgenesis of corpus callosum (yellow arrow) in a child with complete Rhombencephalosynapsis (RES). Primary fissure (green arrow) and prepyramidal fissure (red arrow) are absent. Axial T2W image (b) showing absence of septum pellucidum (white arrow). Coronal T1WI MR (c) shows associated mildly hypoplastic optic chiasm (blue arrow). Case 5: MRI brain at 28 years of age Sagittal T1W MR (a) shows aqueductal stenosis (yellow arrow) causing hydrocephalus with enlarged lateral ventricles (*) in an adult with complete Rhombencephalosynapsis (RES). Absence of the primary fissure (green arrow) and prepyramidal fissure (red arrow) is also seen. There is rounded 4th ventricle fastigial recess (*) secondary to hypoplasia of nodulus. Coronal T2WI MR (b) shows fusion of cerebellar hemispheres and continuous transversely oriented folia and fissures extending across the midline without intervening vermis (blue arrow). Axial T2W image (c) showing fused dentate nuclei without intervening vermis (white arrow). Conclusion Rhombencephalosynapsis (RES) although a rare congenital disorder, can be encountered in pediatric as well as occasionally in adult patients RES is prone to be underreported due to radiologists’ relative lack of awareness of this condition Familiarity with classic imaging findings, associated supratentorial anomalies and related syndromes will allow correct identification and reporting of this rare condition References 1.Obersteiner H. Ein Kleinhirn ohne Wurm. Arb Neurol Inst 1914;21:124 – 136. 2.Barth PG, Rhombencephalosynapsis. Chapter 4, Handbook of Clinical Neurology, Vol. 87 (3rd series). 3.Truwit CL, Barkovich AJ, Shanahan R, et al. Imaging of rhombencephalosynapsis: Report of three cases and review of the literature. AJNRAmJ Neuroradiol 12:957-965, 1991 4.Oei AS, Vanzieleghem BD, Kunnen MF. Diagnostic imaging and clinical findings in rhombencephalosynapsis: case report and literature review. JBR-BTR 2001;84:197 – 200. 5.Demaerel P, Morel C, Lagae L, Wilms G. Partial rhombencephalosynapsis. AJNR Am J Neuroradiol. 2004 Jan;25(1):29-31. 6.Sidman RL, Rakic P. Development of the human central nervous system. In: Haymaker W, Adams RD, eds. Histology and histopathology of the nervous system. Springfield, Ill.: Thomas; 1982:3–145 7. Pasquier L, Marcorelles P, Loget P, Pelluard F, Carles D, Perez MJ, et al. Rhombencephalosynapsis and related anomalies: a neuropathological study of 40 fetal cases. Acta Neuropathologica 2009;117:185-200. 8. Ishak GE, Dempsey JC, Shaw DWW, Tully H, Adam MP, Sanchez-Lara PA, et al. Rhombencephalosynapsis: an under-recognized hindbrain malformation associated with incomplete separation of midbrain and forebrain, hydrocephalus, and a broad spectrum of severity. Brain 2012. 9.Cakirer S, Joubert Syndrome vs Rhombencephalosynapsis: Differentiation on the Basis of MRI Findings. Clinical Radiology Extra 02/2003; 58(2):13-17. 10.Poretti A, Bartholdi D, Gobara S, Alber FD, Boltshauser E, Gomez-Lopez-Hernandez syndrome: an easily missed diagnosis. Eur J Med Genet. 2008 May-Jun;51(3):197-208. 11.Shekdar K, Posterior fossa malformations. Semin Ultrasound CT MR. 2011 Jun;32(3):228-41. Contact Information Abhijit Y. Patil, M.D. Fellow, Neuroradiology Division Dept. of Radiology, University of Michigan 1500 E. Medical Center Drive, UH B2-A209, Ann Arbor, MI 48109-5030 E-mail: [email protected]