Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
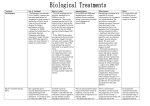
UNIT 3 PSYCHOPATHOLOGY UNIT THREE BIOLOGICAL THERAPIES FOR DEPRESSION Specification requirements LEARNING OBJECTIVES: You will be able to: -Outline the biological therapies for depression -Evaluate the biological therapies for depression in terms of appropriateness and effectiveness. INTRODUCTION The most widely used treatment for depression is chemotherapy, i.e. the use of antidressant drugs. Effective drug treatments for depression developed rapidly in the 1960s with the introduction of two groups of drugs. Monoamine-oxidase inhibitors (MAOIs) These work by inhibiting the work of an enzyme (Mono-amine oxidase) which flushes neurotransmitters such as serotonin and norepinephrine (noradrenaline) out of the synapse like a waste product. MAOIs reduce this action which means that there is more availability of these neurotransmitters in the synapse. Effectiveness and appropriateness They are effective, and are still used for severe cases of depression, but they have severe side-effects if taken with certain food and drink, e.g. marmite, red wine. This is due to the fact that blood pressure is raised which can result in death. For this reason they are not used so much now and patients taking them have to be carefully monitored. Adolescents are not usually prescribed MAOs as they may not monitor their diet so carefully. Sometimes they are used when other drug treatments have failed and/or the patient is hospitalised and their diet can be controlled. Tricyclic antidepressants These drugs work in a different way by blocking the reuptake of neurotransmitters like norepinephrine (noradrenaline) and serotonin so that more remains in the synapse. The end result is the same – there is more neurotransmitter available to pass to the next neurone. 1 UNIT 3 Later, a new class of drug was discovered - Selective serotoinin reuptake inhibitors (SSRIs) These work in the same way as tricyclics but they target serotonin specifically and have fewer side effects. Appropriateness of drug therapy in the treatment of depression The development of anti-depressant drugs was welcomed when they first appeared. They were thought of as a quick, easy and cheap alternative to lengthy psycho therapies. However these features are also their downfall as they are becoming over prescribed. While they might offer hope to some, they only treat the symptoms; the root causes of the depression may remain so that when the patient comes off the medication, the low mood may return. Depressed individuals usually have to continue to take drugs for some time after they have shown improvement. This ‘maintenance therapy’ (Kessler et al, 2002) significantly reduces the rates of relapse. However, anti-depressant drugs are not thought to be addictive (unlike tranquilizers). If addiction does occur, it is only in a minority of people. Nevertheless, it is advisable to come off them slowly and under medical supervision. A number of studies have reported a much higher rate of reduction of symptoms for drugs compared to placebos – more than twice as high (Thase and Kupfer, 1996). However, depression covers a wide range of symptoms which may respond differentially to different treatments and so the same drug doesn’t work for everyone. One of the main problems of using drugs as a treatment for depression is that scientists don’t really know why they work. One curiosity is that serotonin levels are altered immediately by the use of SSRIs and yet symptoms may are not usually relieved for a couple of weeks or even longer. This suggests that there is something else involved apart from the serotonin levels. All of the drugs have potential unwanted side-effects e.g. drowsiness, nausea, decreased sex drive etc. These are far less severe with the more recent SSRI drugs and disappear fairly soon. It seems clear that very few, if any, depressions arise solely from biological factors. Antidepressants seem to be quite effective in reducing some of the symptoms of depression, but they can have no effect on the life circumstances of the individual. For this reason, drug therapy is often combined with various psychological interventions. BE SELECTIVE IN THE MATERIAL YOU INTEND TO PREPARE TO WRITE ABOUT IN AN EXAM SITUATION. YOU ONLY HAVE 30 MINUTES TO PLAN AND WRITE YOUR RESPONSE. YOU WILL NOT NEED TO USE ALL OF THIS MATERIAL. 2 UNIT 3 ELECTRIC CONVULSIVE THERAPY (ECT) ECT was first introduced as a therapeutic technique in the 1930s. It was frequently misused and caused physical and emotional damage to many patients. However, its use today is highly controlled and it is administered under considerably safer conditions. Patients are given sedatives and muscle relaxants. Electrodes are attached to the scalp and a small electric current is passed through the brain for a fraction of a second inducing a convulsion that lasts for approximately one minute. When the patient comes round from the anaesthetic, they will normally have no recollection of the treatment. Clinicians differ int he precise way that they administer the procedure. For example it is not clear exactly how much current should be passed through the brain or whether the treatment is effective when electrodes are only placed on one side of the head instead of both. Similarly there is variability in the number and regularity of treatments offered within a course. A double-blind study (Lerer et al, 1995) comparing the efficacy of the treatment when given twice or three times weekly found little difference in clinical outcomes but there were fewer cognitive side-effects in the twiceweekly programme. It is thought that ECT increases the availability of monoamines e.g. serotonin and norepinephrine (noradrenaline) and that it reduces blood flow in the frontal temporal regions, but the precise mechanisms are unclear. It is extremely effective in cases of severe depression particularly where there are psychotic features or suicidal intent (Sackheim and Rush, 1995). Effectiveness There are contradictory findings regarding the effectiveness of ECT. Rey and Walter (1997) claim that up to 70% of patients with severe depression get relief with ECT. On the other hand, Schwartz (1995) says that 85% of those who are initially helped by ECT relapse, so any benefits can be short-lived. This is supported by Breggin (1997) who found that ECT may have some benefits to certain patients, but that these benefits do not generally last for more than four weeks. Overall, research indicates that ECT is successful for some individuals with depression, although it is often a last resort. For severe cases where the sufferer is suicidal it is thought that ECT has saved many lives as it is fast acting compared to drugs. When compared with sham ECT the real treatment is more effective (according to Buchan et al, 1992) but only when the patient suffers delusions as well as depression (which is rare). Buchan concluded that ECT has few benefits. Appropriateness ECT remains a controversial treatment because it is an invasive assault on the brain and no one is entirely clear how it works. Although modern techniques have eliminated some of the more serious side-effects associated with ECT, there is some evidence that it causes short-term memory loss. There is some disagreement about this. Rogers et al (1993) state that about one third of patients receiving ECT report the experience as distressing and say that they have experienced significant memory loss as a result of their treatment. However in a review of research in this area, Devanand et al (1994) found no convincing evidence that ECT causes long-term memory deficits or that it causes any structural brain damage. There are also ethical considerations with the use of ECT. Although informed consent should be given before this treatment is carried out, it is questionable whether severely depressed people really understand the procedures or the implications of the treatment. 3