Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
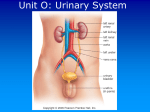
The Urinary System Learning Objectives : Membuat peta konsep sistem ekskresi manusia Mengidentifikasi komponen yang terlibat dalam sistem ekskresi manusia Menggambar struktur ginjal Menjelaskan proses pembentukan urine Membedah serangga untuk diamati struktur alat ekskresinya Menggambar struktur alat ekskresi serangga berdasarkan hasil pengamatan Learning Objectives : To make a concept map of excretory system in human To identify components are involved in human excretory system To draw kidney structure To explain the formation of urine To operate insect for observation its excretory organs structure To draw structure of excretory organs based on observation result Function 1. Remove nitrogenous wastes 2. Maintain electrolyte, acid-base, and fluid balance of blood 3. Homeostatic organ 4. Acts as blood filter 5. Release hormones: calcitriol & erythropoietin Kidneys as Filters • Diuretic- loose water; coffee, alcohol • Antidiuretic- retain water; ADH • Aldosterone- sodium & water reabsorption, and K+ excretion • GFR= 180 liters (50 gal) of blood/day • 178-179 liters are reabsorbed back into blood • Excrete a protein free filtrate Maintaining Chemical Homeostasis The Urinary System The Urinary System blood filtration General Functioning of the Kidney tubular reabsorption and secretion urine “refreshed” blood Nitrogenous Wastes urea uric acid ammonia kidneys Organs of the Urinary System ureters urinary bladder urethra Human Kidney Kidney Anatomy renal pelvis ureter renal pyramids renal cortex renal capsule renal medulla nephron renal artery renal vein Kidney Anatomy blood Nephron Functioning filtration tubular reabsorption and secretion urine “refreshed” blood efferent arteriole afferent arteriole glomerulus artery peritubular capillaries loop of Henle vein Bowman’s capsule proximal convoluted tubule distal convoluted tubule collecting duct Each kidney contains over 1 million nephrons and thousands of collecting ducts Glomerulus DCT renal cortex PCT renal medulla Collecting duct Loop of Henle efferent arteriole afferent arteriole Glomerular Filtration Bowman’s capsule Filters blood; proteins can’t pass through glomerulus The Human Kidney & Nephron How urine produced ?? Composition of Glomerular Filtrate • Water • Small Soluble Organic Molecules • Mineral Ions Proximal Convoluted Tubule Reabsorbs: water, glucose, amino acids, and sodium. • • • • 65% of Na+ is reabsorbed 65% of H2O is reabsorbed 90% of filtered bicarbonate (HCO3-) 50% of Cl- and K+ Loop of Henle Creates a gradient of increasing sodium ion concentration towards the end of the loop within the interstitial fluid of the renal pyramid. • 25% Na+ is reabsorbed in the loop • 15% water is reabsorbed in the loop • 40% K is reabsorbed in the loop Distal Convoluted Tubule Under the influence of the hormone aldosterone, reabsorbs sodium and secretes potassium. Also regulates pH by secreting hydrogen ion when pH of the plasma is low. • only 10% of the filtered NaCl and 20% of water remains Collecting Duct Allows for the osmotic reabsorption of water. ADH (antidiuretic hormone)- makes collecting ducts more permeable to water-- produce concentrated urine Urine Water- 95% Nitrogenous waste: • urea • uric acid • creatinine Ions: • sodium • potassium • sulfate • phosphate From the original 1800 g NaCl, only 10 g appears in the urine How the kidney does its job! Kidney Action Blood enters Bowman’s capsule through a tiny artery — (the renal artery). The artery branches to form a glomerulus. Blood pressure forces some blood plasma and small particles into the surrounding capsule — (this is called the nephric filtrate). Large particles such as blood cells and proteins remain in capillaries. The nephric filtrate is pushed out of the capsule and into the proximal tubule . This is where reabsorption begins. Kidney action (cont) Only materials needed by the body are returned to bloodstream — for example, 99 % of water, all glucose and amino acids and many salts are reabsorbed. Osmosis , diffusion, and active transport draw water , glucose , amino acids and ions from filtrate into surrounding cells. Small villi like projections help in the active transport of glucose out of the filtrate and speed up the reabsorption process. From here, these components return to the bloodstream. Kidney action (cont) The filtrate reaches the end of the proximal tubule and the fluid is isotonic with the surrounding cells. Glucose and amino acids have been removed from the filtrate. The filtrate then moves to the loop of Henle whose primary function is to remove water from the filtrate by osmosis. Kidney action (cont) There is in increase in sodium concentration in the cells of the loop of Henle as we move from the area of the cortex to the inner pelvis of the kidney. This causes water to be drawn from the filtrate. These high levels of sodium are a result of active transport and results in increased concentration of filtrate (due to water loss). Why doesn’t water on outside go back in? The water that left the descending loop cannot enter the ascending loop because it is impermeable to water. As the water concentration in the filtrate decreases, the chlorine concentration increases and causes it to diffuse out of the tubule. This process is helped by the electrical attraction of chlorine to sodium. . Water (cont) The filtrate moves to the distal tubule where tubular secretion occurs. Active transport is used to pull hydrogen ions, creatinine, drugs such as penicillin out of the blood and into the filtrate. Fluid from a number of nephrons moves from the distal tubules to a common collecting duct which carries what can now be called urine to the renal pelvis. NOTE Since the kidneys control what leaves and what remains in the nephrons, they maintain the levels of water, ions and other materials nearly constant and within the limits to maintain homeostasis. Elaborate Exocrine/Endocrine Comparison Research ?????????? Exocrine/Endocrine System BINGO Hormonal Control of Kidney Function Hormonal Control of Kidney Function high plasma solute concentration low blood volume heart receptors hypothalamus Hormonal Control of Kidney Function hypothalamus posterior pituitary antidiuretic hormone collecting ducts Hormonal Control of Kidney Function Hormonal Control of Kidney Function reduced blood pressure and glomerular filtrate juxtaglomerular apparatus renin Hormonal Control of Kidney Function angiotensinogen angiotensin I angiotensin II renin Hormonal Control of Kidney Function angiotensin II adrenal cortex aldosterone convoluted tubules Urinary Bladder ureters external sphincters internal sphincters urethra Bladder 1. Mucosa (transitional epithelium) 2. Muscular layer (detrusor muscle): 3 layers of smooth muscle 3. Fibrous adventia Sphincter Muscles on Bladder Internal urethral sphincter: • Smooth muscle • Involuntary control • More superiorly located External Urethral sphincter: • Skeletal muscle • Voluntary control • Posteriorly located Diuresis (Micturition) When bladder fills with 200 ml of urine, stretch receptors transmit impulses to the CNS and produce a reflex contraction of the bladder (PNS) When is incontinence normal? Distension of the Urinary Bladder Urinalysis Why do doctors ask for a urine sample? characteristics: • smell- ammonia-like • pH- 4.5-8, ave 6.0 • specific gravity– more than 1.0; ~1.0011.003 • color- affected by what we eat: salty foods, vitamins Odor odor- normal is ammonia-like diabetes mellitus- smells fruity or acetone like due to elevated ketone levels diabetes insupidus- yucky asparagus--- pH- range 4.5-8 ave 6.0 vegetarian diet- urine is alkaline protein rich and wheat dieturine is acidic Color Color- pigment is urochrome Yellow color due to metabolic breakdown of hemoglobin (by bile or bile pigments) Beets or rhubarb- might give a urine pink or smoky color Vitamins- vitamin C- bright yellow Infection- cloudy Specific Gravity Water: s.g. = 1g/liter; Urine: s.g. ~ 1.001 to 1.030 Pyelonephritus- urine has high s.g.; form kidney stones Diabetes insipidus- urine has low s.g.; drinks excessive water; injury or tumor in pituitary Abnormal Constitutes of Urine Glucose- when present in urine condition called glycosuria (nonpathological) [glucose not normally found in urine] Indicative of: • Excessive carbohydrate intake • Stress • Diabetes mellitus Abnormal Constitutes of Urine Albumin-abnormal in urine; it’s a very large molecule, too large to pass through glomerular membrane > abnormal increase in permeability of membrane Albuminuria- nonpathological conditionsexcessive exertion, pregnancy, overabundant protein intake-- leads to physiologic albuminuria Pathological condition- kidney trauma due to blows, heavy metals, bacterial toxin Abnormal Constitutes of Urine Ketone bodies- normal in urine but in small amts Ketonuria- find during starvation, using fat stores Ketonuria is couples w/a finding of glycosuria-- which is usually diagnosed as diabetes mellitus RBC-hematuria HemoglobinHemoglobinuria- due to fragmentation or hemolysis of RBC; conditions: hemolytic anemia, transfusion reaction, burns or renal disease Abnormal Constitutes of Urine Bile pigmentsBilirubinuria (bile pigment in urine)- liver pathology such as hepatitis or cirrhosis WBCPyuria- urinary tract infection; indicates inflammation of urinary tract Casts- hardened cell fragments, cylindrical, flushed out of urinary tract WBC casts- pyelonephritus RBC casts- glomerulonephritus Fatty casts- renal damage Summary so far….. Blood enters the kidney through the renal artery at the site of the hilum The PCT is concerned with reabsorption- organic nutrients are reabsorbed and water follows because there is a concentration gradient The remaining filtrate moves into the descending loop of henle. This is lined with thin cells so water moves out A number of other nephrons join up to the cleectig duct which travels through the medulla to the renal papilla wher the filtrate is emptied in the minor calyx 4-5 minor calyces join up to make a major calyx 57 The renal artery divides in to ever smaller arteries and arterioles The filtered substances move into the proximal convoluted tubule Because water has been reabsorbed the concentration of the filtrate is not very high From the DCT the filtrate now passes into the collecting duct. 2-3 major calyces join up to form the renal pelvis Afferent arterioles take blood to the glomerulus to be filtered Once blood is filtered efferent arterioles take blood away from the glomerulus Products which are filtered out: water, mineral salts, amino acids, glucose, hormones, urea, toxins The glomerulus is a network of capillaries which filters the blood The walls of the ascending loop of henle are lined with thicker cells, so water can’t pass in or out. Instead sodium and chloride is pumped out actively In the DCT the volume and composition of the filtrate can be adjusted but this is controlled by hormones The renal pelvis joins the ureter at the hilum Products which do not filter and remain in the blood: Leukocytes, erythrocytes, platelets, plasma proteins The filtrate now enters the distal convoluted tubule- is it now only 20% of what it originally was. The ureter transport the filtrate/urine from the kidney to the bladder INQUIRY 1. 2. 3. 4. 5. List several functions of the kidneys. What does the glomerulus do? What are several constitutes you should not find in urine? What is specific gravity? What two hormones effect fluid volume and sodium concentration in the urine? 6. Where are the pyramids located in the kidney? 7. What vessel directs blood into the glomerulus? 8. Where does most selective reabsorption occur in the nephron?