Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
In the name of God
Pediatrics hypernatremia
Hypernatremia is defined as a serum sodium concentration of more than 145 mEq/L. It is
characterized by a deficit of total body water (TBW) relative to total body sodium levels due to
either loss of free water, or infrequently, the administration of hypertonic sodium solutions.[1]
In healthy subjects, the body's 2 main defense mechanisms against hypernatremia are thirst and
the stimulation of vasopressin release.
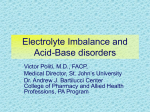
Figure A: Normal cell. Figure B: Cell initially responds to
extracellular hypertonicity through passive osmosis of water extracellularly, resulting in cell
shrinkage. Figure C: Cell actively responds to extracellular hypertonicity and cell shrinkage in
order to limit water loss through transport of organic osmolytes across the cell membrane, as
well as through intracellular production of these osmolytes. Figure D: Rapid correction of
extracellular hypertonicity results in passive movement of water molecules into the relatively
hypertonic intracellular space, causing cellular swelling, damage, and ultimately death.
Pathophysiology
Hypernatremia represents a deficit of water in relation to the body's sodium stores, which can
result from a net water loss or a hypertonic sodium gain. Net water loss accounts for most cases
of hypernatremia. Hypertonic sodium gain usually results from clinical interventions or
accidental sodium loading. As a result of increased extracellular sodium concentration, plasma
tonicity increases. This increase in tonicity induces the movement of water across cell
membranes, causing cellular dehydration.
The following 3 mechanisms may lead to hypernatremia, alone or in concert:
Pure water depletion (eg, diabetes insipidus)
Water depletion exceeding sodium depletion (eg, diarrhea)
Sodium excess (eg, salt poisoning)
Sustained hypernatremia can occur only when thirst or access to water is impaired. Therefore,
the groups at highest risk are infants and intubated patients.
Because of certain physiologic characteristics, infants are predisposed to dehydration. They have
a large surface area in relation to their height or weight compared with adults and have relatively
large evaporative water losses. In infants, hypernatremia usually results from diarrhea and
sometimes from improperly prepared infant formula or inadequate mother-infant interaction
during breastfeeding.
Hypernatremia causes decreased cellular volume as a result of water efflux from the cells to
maintain equal osmolality inside and outside the cell. Brain cells are especially vulnerable to
complications resulting from cell contraction. Severe hypernatremic dehydration induces brain
shrinkage, which can tear cerebral blood vessels, leading to cerebral hemorrhage, seizures,
paralysis, and encephalopathy.
In patients with prolonged hypernatremia, rapid rehydration with hypotonic fluids may cause
cerebral edema, which can lead to coma, convulsions, and death.
Epidemiology
Frequency
United States
Hypernatremia is primarily a hospital-acquired condition occurring in children of all ages who
have restricted access to fluids, mostly due to significant underlying medical problems such as a
chronic disease, neurologic impairment, a critical illness, or prematurity. The incidence is
estimated to be greater than 1% in hospitalized patients. Hospital-acquired hypernatremia
accounts for 60% of hypernatremia cases in children. Gastroenteritis contributes to the
hypernatremia in only 20% of cases. The group most affected is intubated, critically ill patients.
Most cases result from a failure to freely administer water to patients. The incidence of
breastfeeding-related hypernatremia is 1-2%.
International
In developing nations, the reported incidence is 1.5-20%.
Mortality/Morbidity
In children with acute hypernatremia, mortality rates are as high as 20%. Neurologic
complications related to hypernatremia occur in 15% of patients. The neurologic sequelae consist
of intellectual deficits, seizure disorders, and spastic plegias. In cases of chronic hypernatremia
in children, the mortality rate is 10%.
Race
No predilection is documented.
Sex
No sex difference is known.
Age
In the pediatric population, hypernatremia usually affects newborns and toddlers who depend on
caretakers for water, as well patients of any age who have significant underlying medical
problems such as a chronic disease, neurologic impairment, a critical illness, or prematurity.
History
Patients in certain situations or with certain conditions are at risk for hypernatremia, as
follows:
o Hospitalized patients who receive exclusive intravenous fluids
o Patients with coma
o Newborns
o Toddlers
o Patients with diabetes insipidus
o Patients receiving alkali therapy
o Patients with diarrhea
o Patients with fever
o Patients with renal disorders (eg, dysplasia, medullary cystic disease, polycystic
kidney disease, tubulointerstitial disease)
o Patients with obstructive uropathy
o Patients with electrolyte disturbances (eg, hypokalemia, hypercalcemia)
o Patients with heat stroke or excessive hypotonic fluid loss
Signs and symptoms of hypernatremia include the following:
o Irritability
o High-pitched cry or wail
o Periods of lethargy interspersed with periods of irritability
o Altered sensorium
o Seizures
o Increased muscle tone
o Fever
o Rhabdomyolysis[2, 3]
o Oligoanuria
o Excessive diuresis
Physical
Skin turgor is a physical finding in patients with hypernatremia. Extracellular and plasma
volumes tend to be maintained in hypernatremic dehydration until dehydration is severe
(ie, when the patient loses >10% of body weight).
When dehydration is severe, skin turgor is reduced, and the skin develops a characteristic
doughy appearance.
Causes
Hypovolemic hypernatremia
o Diarrhea
o Excessive perspiration
o Renal dysplasia
o Obstructive uropathy
o Osmotic diuresis
Euvolemic hypernatremia
o Central diabetes insipidus causes
o Idiopathic causes
o Head trauma
o Suprasellar or infrasellar tumors (eg, craniopharyngioma, pinealoma)
o Granulomatous disease (sarcoidosis, tuberculosis, Wegener granulomatosis)
o Histiocytosis
o Sickle cell disease
o Cerebral hemorrhage
o Infection (meningitis, encephalitis)
o Associated cleft lip and palate
o Nephrogenic diabetes insipidus causes
o Congenital (familial) conditions
o Renal disease (obstructive uropathy, renal dysplasia, medullary cystic disease,
reflux nephropathy, polycystic disease)
o Systemic disease with renal involvement (sickle cell disease, sarcoidosis,
amyloidosis)
o Drugs (amphotericin, phenytoin, lithium, aminoglycosides, methoxyflurane)
Hypervolemic hypernatremia
o Improperly mixed formula
o NaHCO3 administration
o NaCl administration
o Primary hyperaldosteronism
Differential Diagnoses
Diabetes Insipidus
Nephrogenic Diabetes Insipidus
Laboratory Studies
The following studies are indicated in patients with suspected hypernatremia:
Serum tests of sodium, osmolality, BUN, and creatinine levels
Urine tests of sodium concentration and osmolality
o In cases of hypovolemic hypernatremia, extrarenal losses show urine sodium
levels of less than 20 mEq/L, and in cases of renal losses, urine sodium values are
more than 20 mEq/L.
o In euvolemic hypernatremia, urine sodium data vary.
o In hypervolemic hypernatremia, the urine sodium level is more than 20 mEq/L.
Imaging Studies
Imaging studies of the head should be considered in alert patients with severe
hypernatremia to rule out a hypothalamic lesion affecting the thirst center.
CT scans may help in diagnosing intracranial tumors, granulomatous diseases (eg,
sarcoid, tuberculosis, histiocytosis), and other intracranial pathologies.
MRI further delineates the pathology.
Other Tests
Aldosterone test
Cortisol test
Antidiuretic hormone (ADH) test
Corticotropin (ACTH) test
Medical Care
Medical care involves the correction of hypernatremia. In correcting hypernatremia, do not
rapidly decrease the sodium level because a rapid decline in the serum sodium concentration can
cause cerebral edema. The recommended rate of sodium correction is 0.5 mEq/h or as much as
10-12 mEq/L in 24 hours. Dehydration should be corrected over 48-72 hours. Guidelines for
hydration management have been established.[4] If the serum sodium concentration is more than
200 mEq/L, peritoneal dialysis should be performed using a high-glucose, low-sodium dialysate.
One of the following equations may be used to calculate body water deficit:
o The equations are based on a goal of plasma sodium concentration of 145 mEq/L.
In children, total body water (TBW) is 60% of their lean body weight. Therefore,
TBW = 0.6 X weight. Babies are an exception to these equations and may have a
TBW as much as 80% of their body weight.
Water deficit (in L) = [(current Na level in mEq/L ÷ 145 mEq/L) - 1] X
0.6 X weight (in kg)
Water deficit (in L) = [(current Na level in mEq/L - 145 mEq/L)/145
mEq/L)] X 0.6 X weight (in kg)
Water deficit (in L) = [1- (145 mEq/L ÷ current Na level in mEq/L)] X 0.6
X weight (in kg)
o
Example calculation: A child weighs 10 kg and has a plasma sodium
concentration of 160 mEq/L. By using the first equation, water deficit (in L) =
[(160 mEq/L ÷ 145 mEq/L) - 1] X 0.6 X 10 = 0.62 L.
The volume of replacement fluid needed to correct the water deficit is determined by
using the concentration of sodium in the replacement fluid. The replacement volume can
be determined as follows:
o Replacement volume (in L) = TBW deficit X [1 ÷ 1 - (Na concentration in
replacement fluid in mEq/L ÷ 154 mEq/L)]
o Example calculation: If the patient from the example calculation above has a
TBW of 0.62, and if the replacement fluid contains 0.2% NaCl (Na concentration
of 34 mEq/L), the replacement volume (in L) = 0.62 L X [1 ÷ 1 - (34 mEq/L ÷
154 mEq/L)] = 0.79 L. This volume has to be replaced slowly over 48-72 hours.
The election of intravenous fluid is based on the following:
o If the patient is hypotensive, normal saline (lactated Ringer solution, or 5%
albumin solution) should be used regardless of a high serum sodium
concentration.
o In hypernatremic dehydration, 0.45% or 0.2% NaCl should be used as a
replacement fluid to prevent excessive delivery of free water and a too-rapid
decrease in the serum sodium concentration.
o In cases of hypernatremia caused by sodium overload, sodium-free intravenous
fluid (eg, 5% dextrose in water) may be used, and a loop diuretic may be added.
o The serum sodium concentration should be monitored frequently to avoid toorapid correction of hypernatremia.
o In cases of associated hyperglycemia, 2.5% dextrose solution may be given.
Insulin treatment is not recommended because the acute decrease in glucose,
which lowers plasma osmolality, may precipitate cerebral edema.
o Once the child is urinating, add 40 mEq/L KCl to fluids to aid water absorption
into cells.
o Calcium may be added if the patient has an associated low serum calcium level.
Serum sodium levels should be monitored every 4 hours.
Consultations
Consultation is also recommended for patients with renal dysplasia, medullary cystic disease,
reflux nephropathy, or polycystic disease.
Diet
Critical care specialist: Patients with symptomatic hypernatremia may need to be
transferred to a pediatric ICU for appropriate treatment and monitoring.
Endocrinologist: Consult an endocrinologist for patients with primary
hyperaldosteronism.
Nephrologist: Consult a nephrologist in cases of renal failure, obstructive uropathy, and
serum sodium levels of more than 180 mEq/L for possible peritoneal dialysis.
In diabetes insipidus, a sodium-restricted and protein-restricted diet should be prescribed.
Medication Summary
Vasopressin and vasopressin analogs
Class Summary
Desmopressin is a synthetic ADH with actions mimicking vasopressin. These agents are
used to treat diabetes insipidus, which deprives the kidney of its capacity to produce
concentrated urine. This effect results in large volumes of dilute urine (polyuria) and
excessive thirst (polydipsia). Serum sodium concentrations may be elevated, but
hypernatremia is most likely to be severe when fluid is restricted.
View full drug information
Desmopressin acetate (DDAVP)
Structural analog of vasopressin (ADH), the endogenous posterior pituitary hormone that
maintains serum osmolality in a physiologically acceptable range. Works in
neurohypophysial (eg, central) diabetes insipidus. Exerts similar antidiuretic effects.
Vasopressin increases resorption of water at level of renal collecting duct, reducing
urinary flow and increasing urine osmolality.
View full drug information
Vasopressin (Pitressin)
Exogenous, parenteral form of ADH. Antidiuretic and increases resorption of water at
renal collecting ducts.
Diuretics
Class Summary
These drugs promote the excretion of water and electrolytes by the kidneys. They are
used in patients with nephrogenic diabetes insipidus.
View full drug information
Hydrochlorothiazide (Esidrix, HydroDIURIL)
Works by increasing excretion of sodium, chloride, and water by inhibiting sodium ion
transport across renal tubular epithelium. Resulting sodium depletion reduces glomerular
filtration rate, enhancing reabsorption of fluid in proximal portion of nephron, decreasing
The medications described below are used in patients with diabetes insipidus who have
hypernatremia.
delivery of sodium to ascending limb of loop of Henle and consequently reducing
capacity to dilute urine.
Further Inpatient Care
Record daily body weights in patients with hypernatremia.
Frequently monitor electrolyte concentrations.
Restrict sodium and protein intake.
Treat the underlying disease.
Further Outpatient Care
Treat the underlying disease.
Restrict sodium and protein intake.
Transfer
Patients with symptomatic hypernatremia should be transferred to a pediatric intensive
care unit for appropriate treatment and close monitoring.
Patients should be transferred to a facility that has dialysis in case of renal failure or in
case the serum sodium concentration is more than 180 mEq/L.
Deterrence/Prevention
Parents and caregivers should avoid making oral rehydration solutions at home or adding
salt to any commercial infant formula.
Treat the underlying cause.
Complications
Seizures can occur because of hypernatremia per se, which is rare. They usually occur
during the treatment of hypernatremia because of a rapid decline in serum sodium levels.
Therefore, slowly correcting hypernatremia is important.
Other complications include the following:
o Mental retardation
o Intracranial hemorrhage
o Intracerebral calcification
o Cerebral infarction
o Cerebral edema, especially during treatment
o Hypocalcemia
o Hyperglycemia
Prognosis
Patients usually recover from hypernatremia.
Patients with recurrent hypernatremic dehydration develop neurologic sequelae,
especially infants with diabetes insipidus.
Patient Education
Parents and caregivers should avoid making oral rehydration solutions at home or adding
salt to any commercial infant formula.
Parents, especially breastfeeding mothers, should watch for neonatal dehydration and
perinatal care.
The breastfed infant should be routinely monitored during the first weeks of life.[5]
In patients with diabetes insipidus, the following is indicated:
o Monitor weight and urine output because clinically significant changes in sodium
values are associated with changes in weight.
o Restrict sodium and protein intake.
o The patient should drink liberal amounts of water.
o The patient and parents should ensure thirst develops before taking or giving
medications.
Pediatric Hyponatremia
Practice Essentials
Hyponatremia, defined as a serum sodium (Na) concentration of less than 135 mEq/L, can lead
to hyponatremic encephalopathy, particularly in prepubescent pediatric patients.
Signs and symptoms
CNS findings
Early signs of hyponatremia include the following:
Anorexia
Headache
Nausea
Emesis
Advanced signs include the following:
Impaired response to verbal stimuli
Impaired response to painful stimuli
Bizarre behavior
Hallucinations
Obtundation
Incontinence
Respiratory insufficiency
Seizure activity
Far-advanced signs include the following:
Decorticate or decerebrate posturing
Bradycardia
Hypertension or hypotension
Altered temperature regulation
Dilated pupils
Seizure activity
Respiratory arrest
Coma
Cardiovascular and musculoskeletal findings
Cardiovascular: Hypotension and tachycardia
Musculoskeletal: Weakness and muscular cramps
See Clinical Presentation for more detail.
Diagnosis
Routine laboratory studies used in the diagnosis and evaluation of hyponatremia include the
following:
Serum Na level
Serum osmolality
Blood urea nitrogen (BUN) and creatinine levels
Urine osmolality
Urine Na level
Urine Na concentrations
The urine Na level differs according to the type of hyponatremia present. In hypovolemic
hyponatremia, Na concentrations are as follows:
Renal losses caused by diuretic excess, osmotic diuresis, salt-wasting nephropathy,
adrenal insufficiency, proximal renal tubular acidosis, metabolic alkalosis, or
pseudohypoaldosteronism result in a urine Na concentration of more than 20 mEq/L
Extrarenal losses caused by vomiting, diarrhea, sweat, or third spacing result in a urine
Na concentration of less than 20 mEq/L secondary to increased tubular reabsorption of
Na
In normovolemichyponatremia caused by syndrome of inappropriate antidiuretic hormone
(SIADH) secretion, reset osmostat, glucocorticoid deficiency, hypothyroidism, or water
intoxication, the urine Na concentration is more than 20 mEq/L
Hypervolemichyponatremia results in the following urine Na concentrations:
If hyponatremia is caused by an edema-forming state (eg, congestive heart failure,
hepatic failure), the urine Na concentration is less than 20 mEq/L
If hyponatremia is caused by acute or chronic renal failure, the urine Na concentration is
more than 20 mEq/L
In SIADH with normal dietary salt intake, urine sodium concentration is more than 40 mEq/L,
while in cerebral salt-wasting syndrome (CSWS), the concentration frequently exceeds
80mEq/L.
Other studies
Special laboratory studies include the following:
Aldosterone level
Cortisol level
Free T4 and thyroid-stimulating hormone (TSH) levels
Adrenocorticotropic hormone (ACTH) level
Antidiuretic hormone (ADH) level
See Workup for more detail.
Management
Hypovolemic hyponatremia
The immediate goal is to correct volume depletion with normal saline. As soon as the patient is
hemodynamically stable, hyponatremia should be corrected.
Physiologic considerations indicate that a relatively small increase in the serum Na
concentration, on the order of 5%, should substantially reduce cerebral edema.
Normovolemichyponatremia
Treatment of normovolemichyponatremia due to SIADH can include fluid restriction and the
administration of normal saline. The use of 3% NaCl and the intravenous (IV) administration of
furosemide may also be needed.
Hypervolemichyponatremia
Treatment includes the following:
Fluid restriction
Administration of 3% NaCl to stop the symptoms
Treatment of the underlying cause
Asymptomatic hyponatremia
Hypovolemic hyponatremia: The main principle is to avoid hypotonic fluids and to
slowly correct Na levels
Normovolemichyponatremia: Restriction of fluids to two thirds (or less) of the volume
needed for maintenance is the mainstay of treatment
Recalcitrant euvolemichyponatremia: Demeclocycline can be used to induce therapeutic
nephrogenic diabetes insipidus, which may help to eliminate excessive water
See Treatment and Medication for more detail.
Image library
Drugs that impair water excretion.
Background
Hyponatremia is defined as serum sodium (Na) concentration of less than 135 mEq/L. Plasma
Na plays a significant role in plasma osmolality and tonicity (serum osmolarity = 2Na + Glu/18
+ BUN/2.8). Changes in plasma osmolality are responsible for the signs and symptoms of
hyponatremia and also the complications that happen during treatment in the presence of highrisk factors. Whereas hypernatremia always denotes hypertonicity, hyponatremia can be
associated with low, normal, or high tonicity. Hyponatremia is the most common electrolyte
disorder encountered in hospitalized patients.
Clinical presentation of hyponatremia happens as a result of a rapid of fall in serum Na and also
the absolute level of serum Na. Fifty percent of presenting children develop symptoms when
serum Na levels fall below 125 mEq/L, a relatively high level when compared with adults.
Although morbidity widely varies, serious complications can arise from hyponatremia and can
also happen during treatment. Understanding the pathophysiology and treatment options for
hyponatremia is important because significant morbidity and mortality are possible.
Pathophysiology
Hyponatremia can develop because of (1) excessive free water, a common cause in hospitalized
patients receiving hypotonic solutions; (2) excessive renal or extrarenal losses of Na or renal
retention of free water; (3) rarely, deficient intake of Na.
Under normal circumstances, the human body is able to maintain serum Na in the normal range
(135-145 mEq/L) despite wide fluctuations in fluid intake. The body's defense against
developing hyponatremia is the kidney's ability to generate dilute urine and excrete free water in
response to changes in serum osmolarity and intravascular volume status.
Hospital-acquired hyponatremia is the most common cause of hyponatremia in children. Some
studies have outlined the association of hyponatremia and the hypotonic fluid typically used in
the pediatric population. Excessive antidiuretic hormone (ADH) is present in most hospitalized
patients, either as an appropriate response to hemodynamic and/or osmotic stimuli or as an
inappropriate secretion of ADH. ADH is also secreted in response to pain, nausea, and vomiting
and during the use of certain medications such as morphine during the postoperative period. Use
of hypotonic fluids in presence of circulating ADH can causes free water retention resulting in
hyponatremia. In certain clinical conditions, ADH secretion occurs even when serum osmolarity
is low or normal, hence the term syndrome of inappropriate ADH secretion (SIADH).
Other conditions that can lead to hyponatremia include states with increased total body water
such as with cirrhosis, cardiac failure, or nephrotic syndrome. Diuretic use and decreased intake
of Na can also lead to hyponatremia.
Loss of Na via the GI tract and or urinary tract in excess of free water can result in hyponatremia.
GI losses can occur in different disease states with excessive fluid loss, namely gastroenteritis,
fistulas, or serous fluid drainage after surgery. Na can be lost via the kidney; use of diuretics is
the most common culprit, followed by other causes, such as salt-losing nephritis,
mineralocorticoid deficiency, and cerebral salt-wasting syndrome (CSWS). Hyponatremia is
rarely caused by deficient Na intake.
Clinical manifestations vary from an asymptomatic state to severe neurologic dysfunction. CNS
symptoms predominate in hyponatremia, although cardiovascular and musculoskeletal findings
may be present. Factors that contribute to CNS symptoms are (1) the rate at which serum Na
levels change, (2) the absolute serum Na level, (3) the duration of the abnormal serum Na level,
(4) the presence of other CNS pathology risk factors, and (5) the presence of excessive ADH
levels.
CNS effects
Hyponatremia exerts most of its clinical effects on the brain. Brain volume is regulated by equal
osmolality of extracellular and intracellular fluid. When extracellular osmolality decreases, water
influx occurs in the brain resulting in cerebral edema. Cerebral edema is responsible for
symptoms such as headache, nausea, vomiting, irritability, and seizures.
If hyponatremia is acute (ie, within hours), the change in osmolality causes influx of water
resulting in cerebral edema. If hyponatremia occurs slowly (ie, over days), the brain has adaptive
response to protect itself from edema formation. The brain’s adaptive response is mediated
through different mechanisms and also modified by different factors as discussed below.
Mechanisms implied in cerebral edema formation include the following:
Na-K ATPase system
Aquaporin channels
Organic osmolytes
Hyponatremia and resulting reduced osmolarity leads to an influx of water into the brain,
primarily through glial cells and largely via the water channel aquaporin (AQP). Water is then
shunted to astrocytes, which swell, largely preserving the neurons. Na is extruded at the same
time using Na-K ATPase system. Potassium ions extrusion follows Na but is slower. In addition,
inorganic osmolytes and organic osmolytes (eg, glycine, taurine, creatine, and myoinositol) have
been shown to efflux from cells during hypo-osmolar states in animal studies.
The brain’s adaptive response to protect itself from edema occurs over several days. Once the
brain has adapted to the hypo-osmolar conditions, a correction of the hypo-osmolar extracellular
space to aneuvolemic or hyper-osmolar state that is too rapid leads to a rapid efflux of water
from brain tissue, resulting in dehydration of brain cells. The resultant condition is called
osmotic demyelination syndrome (ODS). Previously, this pathological injury was described only
in the pons, hence the term central pontinemyelinolysis (CPM). Although it predominantly
affects the pons, this condition is now known to occur in other parts of brain as well (see
Complications).
Hyponatremic encephalopathy
Risk factors for hyponatremic encephalopathy include age, sex, hypoxia and vasopressin levels.
Sex
o
o
Epidemiologic data have shown that the risk for developing permanent neurologic
sequelae or death from hyponatremic encephalopathy is substantially higher in
menstruating women than in men or postmenopausal women.[1] The relative risk
of death or permanent neurologic damage due to hyponatremic encephalopathy is
about 30 times greater for women than for men and about 25 times greater for
menstruating women than for postmenopausal women.
Although estrogen hormones have been implicated as the cause of this high
incidence of hyponatremic encephalopathy, cellular level mechanisms have now
been elucidated. Estrogen has a core steroidal structure similar to cardiac
glycosides known to inhibit the Na-K ATPase system, impairing adaptive
responses. In addition, estrogen also appears to regulate water movement and
neurotransmission by affecting AQP4 expression.
Age
o
o
Prepubescent children are at increased risk to develop complications because of
hyponatremia. Although many other factors may contribute to this increased risk,
brain–to–cranial vault ratio plays an important role.
The brain reaches adult size by age 6 years, whereas the skull does not reach adult
size until age 16 years. As a consequence, children can develop symptomatic
hyponatremia with relatively higher Na concentrations than those observed in
adults.
o
Good outcomes are reported in young babies with open fontanelles; increased
vault compliance supports this hypothesis.
Hypoxia
o Hypoxia is a major risk factor for hyponatremic encephalopathy. Patients with
symptomatic hyponatremia can develop hypoxia by 2 different mechanisms:
noncardiogenic pulmonary edema and hypercapnic respiratory failure.
Hypercapnic respiratory failure is due to central respiratory depression and is
often the first sign of impending herniation. Noncardiogenic pulmonary edema,
on the other hand, is a complex disorder during with increased vascular
permeability and increased catecholamine release that often occurs secondary to
elevated intracranial pressure.
o Hypoxia worsens clinical outcomes in hyponatremic encephalopathy by impairing
the brain’s adaptive response through the active transport of Na, which is an
energy-dependent process that requires oxygen. It also affects astrocyte volume
regulation, which is also energy dependent. Under ordinary circumstances,
hypoxia results in an increase in cerebral blood flow to increase the delivery of
oxygen;[2] the increase in cerebral blood flow can lead to an increase in cerebral
blood volume, which also contributes to an increase in intracranial pressure.
Vasopressin
o Hyponatremia, except in cases of pure water intoxication, virtually always occurs
in the presence of increased plasma levels of vasopressin.[3]
o Vasopressin leads to decreased cerebral oxygen use in female rat brain but not in
male rats. Vasopressin decreases cerebral blood flow by vasoconstriction,
resulting in decreased oxygen delivery that, in turn, impairs brain adaptation.
Vasopressin also facilitates direct movement of water into brain cells independent
of hyponatremia. In addition, it also decreases synthesis of ATP and
phosphocreatine, lowers intracellular pH and intracellular buffering, and
decreases Ca2+, which affects energy-dependent processes involved in brain
adaptation.
Cardiovascular response to hyponatremia
Hyponatremia is also often classified by body water volume status: hyponatremia in conjunction
with hypervolemia, euvolemia, or hypovolemia. The distribution of water and solute in the
intracellular and extracellular spaces determine the intravascular volume. Fluid shifts from the
extracellular space to the intracellular space with a subsequent decrease in arterial blood volume.
The reduction in intravascular volume may result in hypotension. Because of this fluid shift,
hyponatremia causes hemodynamic disturbance more pronounced than that expected for the
degree of dehydration.
Frequency
United States
Reported frequency varies from 1-30% among hospitalized pediatric patients.
International
In India, the frequency of hyponatremia is 29.8%.[4] It is more frequent in summer (36%) than in
winter (24%).
Mortality/Morbidity
Overall morbidity and mortality is 42%.
Sex
The incidence of hyponatremia is equal in both sexes. However, CNS complications are most
likely to occur among premenopausal women.
Age
Hyponatremic encephalopathy is most common in prepubescent children.
History
Physical
Causes
Show All
Multimedia Library
References
History
The history of patients with hyponatremia may include the following:
Hypotonic fluid use for maintenance hydration in hospitalized children (potential risk
factor)
Feeding with hypotonic formula or excessive free water during infancy
Conditions that cause GI, Na-rich fluid loss, including the following:
o Diarrhea
o Vomiting
o Fistulas
Renal disorders, including the following:
o Salt-losing nephropathy
o Acute renal failure
o Chronic renal failure
Postoperative states[5]
Psychiatric conditions
Coma
Drug use
CNS and pulmonary diseases
Hypothyroidism
Adrenal insufficiency
Cirrhosis
Congestive heart failure
Acquired immunodeficiency syndrome (AIDS)
Cystic fibrosis
Physical
CNS findings
Early signs include the following:
o Anorexia
o Headache
o Nausea
o Emesis
Advanced signs include the following:
o Impaired response to verbal stimuli
o Impaired response to painful stimuli
o Bizarre behavior
o Hallucinations
o Obtundation
o Incontinence
o Respiratory insufficiency
o Seizure activity
Far-advanced signs include the following:
o Decorticate or decerebrate posturing
o Bradycardia
o Hypertension or hypotension
o Altered temperature regulation
o Dilated pupils
o Seizure activity
o Respiratory arrest
o Coma
Cardiovascular findings
Hypotension
Tachycardia
Musculoskeletal findings
Weakness
Muscular cramps
Causes
Hypervolemichyponatremia (excess free-water retention)
Congestive heart failure
Cirrhosis
Nephrotic syndrome
Acute or chronic renal failure
Hypovolemic hyponatremia due to renal loss of sodium in excess of free-water
Diuretic excess
Osmotic diuresis
Salt-wasting diuresis
Adrenal insufficiency
Metabolic alkalosis
Pseudohypoaldosteronism
Hypovolemic hyponatremia due to extrarenal loss of sodium in excess of freewater
GI conditions, such as the following:
o Vomiting
o Diarrhea
o Drains
o Fistula
Sweat
Cystic fibrosis
Cerebral salt-wasting syndrome (CSWS)
Third-spacing conditions, such as the following:
o Pancreatitis
o Burns
o Muscle trauma
o Peritonitis
o Effusions
o Ascites
Normovolemichyponatremia
Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
o Tumors - Adenocarcinoma of the duodenum, adenocarcinoma of the pancreas,
carcinoma of the ureter, carcinoma of the prostate, Hodgkin disease, thymoma,
acute leukemia, lymphosarcoma, or histiocytic lymphoma
o Chest disorders - Infection (eg, tuberculosis or bacterial, mycoplasmal, viral, or
fungal infection), positive-pressure ventilation, decreased left atrial pressure (eg,
o
due to pneumothorax, atelectasis, asthma, cystic fibrosis, mitral valve
commissurotomy, ligation of the patent ductusarteriosus ligation), or malignancy
CNS disorders - Infection (eg, tuberculous meningitis, bacterial meningitis,
encephalitis), trauma, hypoxia-ischemia, psychosis, brain tumor, or miscellaneous
CNS disorders (eg, Guillain-Barré syndrome, ventriculoatrial shunt obstruction,
acute intermittent porphyria, cavernous sinus thrombosis, multiple sclerosis,
anatomic abnormalities, vasculitis, stress, idiopathic causes)
o
Drugs (see image below)
Drugs that impair water excretion.
Reset osmostat
Glucocorticoid deficiency
Hypothyroidism
Water intoxication due to intravenous (IV) therapy, tap-water enema, or psychogenic
water drinking
Differential Diagnoses
Adrenal Insufficiency
Cerebral Salt-Wasting Syndrome
Diarrhea
Hypothyroidism
Syndrome of Inappropriate Antidiuretic Hormone Secretion
Laboratory Studies
Verify the accuracy of laboratory results in patients with hyponatremia.
Exclude pseudohyponatremia.
o Findings on flame emission spectrophotometry
If Na measurement is performed by using flame emission
spectrophotometry, hyponatremia is falsely low in patients with
hyperproteinemia and hypertriglyceridemia.
Raised proteins and lipid levels increase the nonaqueous portion of
plasma, which normally forms 7% of the plasma.
However, new ion-specific Na electrodes measure Na from only the
aqueous phase, enabling accurate estimation of serum Na concentrations.
o Correction factors for raised proteins and lipids
Triglycerides (in milligrams per deciliter) X 0.002 = decrease in plasma
Na level (in milliequivalents per liter)
(Plasma protein level [in grams per deciliter] - 8) X 0.25 = decrease in
plasma Na (in milliequivalents per liter)
Exclude distributive hyponatremia.
o Distributive hyponatremia occurs when the plasma glucose concentration exceeds
100 mg/dL.
o Each 100-mg/dL increase in the glucose level above 100 mg/dL leads to a 1.6mEq/L decrease in the Na concentration.
Obtain routine laboratory studies to assess the following:
o Serum Na level
o Serum osmolality
o BUN and creatinine levels
o Urine osmolality
o Urine Na level
Urine Na level changes according to the type of hyponatremia.
o Hypovolemic hyponatremia
Renal losses caused by diuretic excess, osmotic diuresis, salt-wasting
nephropathy, adrenal insufficiency, proximal renal tubular acidosis,
metabolic alkalosis, or pseudohypoaldosteronism result in a urine Na
concentration of more than 20 mEq/L.
Extrarenal losses caused by vomiting, diarrhea, sweat, or third spacing
result in a urine Na concentration of less than 20 mEq/L secondary to
increased tubular reabsorption of Na.
o Normovolemichyponatremia: When hyponatremia is caused by syndrome of
inappropriate antidiuretic hormone secretion (SIADH), reset osmostat,
glucocorticoid deficiency, hypothyroidism, or water intoxication, the urine Na
concentration is more than 20 mEq/L.
o Hypervolemichyponatremia
If hyponatremia is caused by an edema-forming state (eg, congestive heart
failure, hepatic failure), the urine Na concentration is less than 20 mEq/L
because effective arterial perfusion is low despite an increase in total body
water. Use of diuretics affects urine Na concentration.
If hyponatremia is caused by acute or chronic renal failure, the urine Na
concentration is more than 20 mEq/L.
o SIADH: Urine sodium concentration is more than 40mEq/L with normal dietary
salt intake.
o Cerebral salt-wasting syndrome (CSWS): Urine loss is significantly higher and
frequently exceeds 80 mEq/L.
Special laboratory studies include tests of the following:
o Aldosterone level
o Cortisol level
o Free T4 and thyroid-stimulating hormone (TSH) levels
o Adrenocorticotropic hormone (ACTH) level
o Antidiuretic hormone (ADH) level
Imaging Studies
Neuroimaging (only if clinically indicated, not routinely performed)
o CT scanning is useful for evaluating causative intracranial pathologies, such as
tumors, hydrocephalus, and hemorrhage. It is also useful for detecting cerebral
edema and demyelinating lesions that occur during treatment. CT scanning is
superior to MRI in delineating hemorrhage and calcifications.
o MRI is sensitive for detecting tumors and demyelination.
Abdominal imaging (only if clinically indicated, not routinely performed)
o Ultrasonography may be performed to detect abdominal masses, such as those due
to bilateral adrenal hyperplasia, and adrenal tumors.
Medical Care
Principles of treatment in hyponatremia
o The most common and devastating effects of hyponatremia are of CNS origin.
Therefore, identifying the risk factors that lead to hyponatremia and instituting
prompt treatment while avoiding complications is crucial.
o Although cerebral adaptation to low serum Na occurs slowly, it protects the brain
from deleterious effects of hypo-osmolality. However, this protective mechanism
leaves the brain susceptible to osmotic demyelination syndrome (ODS) during
treatment, especially in persons with chronic hyponatremia, if the correction is
rapid.
Equations used in managing hyponatremia
o To estimate the effect of 1 L of any infusate on serum Na concentration: Change
in Na concentration = (infusate Na level - serum Na level)/(total body water + 1)
o To estimate the effect of 1 L of any infusate containing Na and potassium (K) on
serum Na concentration: Change in serum Na level = [(infusate Na level +
infusate K level) - serum Na level]/(total body water + 1)
Na concentrations of various fluids used in pediatric practice
o 5% NaCl in water - 855 mEq/L
o 3% NaCl in water - 513 mEq/L
o 0.9% NaCl in water - 154 mEq/L
o Ringer lactate solution - 130 mEq/L
o 0.45% NaCl in water - 77 mEq/L
o 0.2% NaCl in water - 34 mEq/L
o 5% dextrose in water - 0 mEq/L
Management of hypovolemic hyponatremia
o The immediate goal is to correct volume depletion with normal saline. As soon as
the patient is hemodynamically stable, hyponatremia should be corrected as per
the treatment principles described below. In patients with seizure, 3% NaCl
should be given while volume depletion is being corrected.
o No consensus has been reached about the optimal treatment of symptomatic
hyponatremia. However, guidelines for hydration management have been
established.[6] Physiologic considerations indicate that a relatively small increase
in the serum Na concentration, on the order of 5%, should substantially reduce
cerebral edema. Available evidence indicates that even a 9 mEq/L increase in
serum Na concentration over 24 hours can result in demyelinating lesions. Given
the risk of demyelinating lesions, the recommended rate of correction should not
exceed 8 mEq/L/d. Even hyponatremia-induced seizures can be stopped with
changes in serum Na concentration of only 3-7 mEq/L.
o Treatment of normovolemichyponatremia due to syndrome of inappropriate
antidiuretic hormone secretion (SIADH) can include fluid restriction, along with
the administration of normal saline; the use of 3% NaCl, and intravenous (IV)
administration of furosemide may also be needed. Furosemide is given to offset
the volume expansion created by the 3% Na infusion. As previously discussed,
when confronted with neurologic symptoms the plan is to raise the serum Na
concentration until symptoms resolve, this can be done by giving doses of 1-2
mL/Kg of 3% saline, symptoms typically resolve with a rise in sodium of 3-7
mEq/L; subsequently, closely monitor electrolyte levels so that the correction
does not exceed 8 mEq/L/d. This appears to leave little room for elevation of
serum sodium after immediately addressing symptoms; however, it appears that
maintaining control of the absolute rise over 24 hours remains beneficial, even
after the immediate emergent increase in serum sodium.
Management of hypervolemichyponatremia: In patients with hypervolemichyponatremia,
restrict fluids, administer 3% NaCl to stop the symptoms, and treat the underlying cause.
Management of asymptomatic hyponatremia
o In asymptomatic individuals with hypovolemic hyponatremia, one should not rush
to correct hyponatremia. The main principle is to avoid hypotonic fluids and to
slowly correct Na levels, especially when hyponatremia has been present for 48
hours or longer. When the duration of hyponatremia is unknown, as is
encountered in outpatient settings, assume hyponatremia is chronic and treat
accordingly. Closely monitor electrolyte values, and the rate of correction should
not exceed 8 mEq/L/d.
o In patients with normovolemichyponatremia, restriction of fluids to two-thirds (or
less) of the volume needed for maintenance is the mainstay of treatment. Diuretics
can be administered with fluid restriction to remove excessive free water. Once
again, the change in Na levels should not exceed 8 mEq/L/d.
o In recalcitrant euvolemichyponatremia, one can use demeclocycline to induce
therapeutic nephrogenic diabetes insipidus, which might help eliminate excessive
water. However, one must remember that total correction should not exceed the
established goal.
Consultations
Transfer patients with symptomatic hyponatremia to a pediatric ICU for appropriate
treatment and close monitoring.
Consult an endocrinologist when patients have hypothyroidism or adrenal insufficiency.
Consult a nephrologist when patients have salt-losing nephropathy, renal failure, or
recalcitrant hyponatremia.
Appropriate neurosurgical care is required when CNS conditions are the cause of
SIADH.
Diet
Patients with salt-wasting disorders (eg, salt-losing nephropathies) need Na
supplementation throughout the period of continued loss of excessive Na.
Patients with SIADH and renal failure require fluid restriction.
o
CT and MRI may help in further delineating the tumor.
Medication Summary
Diuretics
Class Summary
These agents promote renal excretion of water and electrolytes. They are used to treat
heart failure or hepatic, renal, or pulmonary disease when Na and water retention results
in edema or ascites.
View full drug information
Furosemide (Lasix)
Potent loop diuretic. Inhibits reabsorption of sodium and chloride in proximal and distal
tubules and loop of Henle. High efficacy largely due to unique site of action. Action on
distal tubule independent of any possible inhibitory effect on carbonic anhydrase or
aldosterone.
ADH inhibitors
Class Summary
These agents produce diuresis by inhibiting antidiuretic hormone (ADH)-induced water
reabsorption. Rarely used to treat pediatric hyponatremia in the pediatric ICU setting.
View full drug information
Lithium (Eskalith, Lithobid)
Inhibits renal response to ADH.
View full drug information
Medical therapy in hyponatremia includes the administration of 3% Na chloride (Na, 513
mEq/L), normal Na chloride solution (Na, 154 mEq/L), diuretics, and other drugs used to
treat syndrome of inappropriate antidiuretic hormone secretion (SIADH), such as lithium
carbonate, demeclocycline, ethanol, phenytoin, and vasopressin analogs.[7]
Demeclocycline (Declomycin)
Only tetracycline used to treat SIADH. Produces diuresis by inhibiting ADH-induced
water reabsorption in distal portion of convoluted tubules and collecting ducts of kidneys.
Effects observed within 5 d and are reversed 2-6 d after cessation of therapy. Administer
1 h before or 2-3 h after ingestion of milk or food.
View full drug information
Phenytoin (Dilantin)
Inhibits secretion of ADH.
Deterrence/Prevention
Carefully monitor patients receiving drugs that can cause hyponatremia.
Give careful consideration to the type of intravenous (IV) hydrating solution used in
pediatric patients. The findings of one study conclude that the use of hypotonic
maintenance fluids increases the incidence of hyponatremia because they decrease blood
sodium levels in normonatremic patients. Isotonic maintenance fluids did not increase the
incidence of dysnatremia and showed a reduced incidence of hyponatremia in the patients
studied. The findings suggest that the administration of isotonic fluids should be
considered the standard of care in critically ill children.[8]
Prudently monitor serum electrolytes in postoperative patients, patients on IV fluids, and
in those with brain tumors, intracranial infections, pulmonary infections, or head trauma.
Complications
Osmotic demyelination syndrome (ODS)
Brain damage and cerebral demyelination can develop if the serum Na level raises rapidly in
chronic hyponatremia.
Epidemiology: The exact incidence of ODS is unknown, and data are derived primarily
from autopsy series. In 3548 consecutive autopsies in adults with ODS, the typical
lesions were found in 9 (0.25%).[9] In another study, Sterns et al observed myelinolysis in
as many as 25% of patients with hyponatremia who were treated with aggressive
protocols.[10] The incidence is highest among high-risk groups.
Risk factors
o Alcoholism (common)
o Malnutrition (common)
o After prolonged diuretic use (frequent)
o Psychogenic polydipsia (rare if acute)
o Burns (infrequent, and often in context of hypernatremia)
o
o
o
o
o
Liver transplantation (well recognized)[11]
Pituitary surgery (rare)
Urologic or gynecologic surgery, especially if it involved glycine infusions (rare)
Correcting serum Na into hypernatremic levels
Hypoxia
Subtypes
o Central pontinemyelinolysis (CPM): Lesions are confined to the pons.
o Extrapontinemyelinolysis (EPM): Lesions are confined to the basal ganglia,
cerebrum, and cerebellum.
o ODS: CPM and EPM lesion sites are both present.
Pathogenesis: The pathogenesis of ODS is unknown. Cells conditioned to hypo-osmotic
hyponatremia may have a decreased adaptive capacity to osmotic stress. The predilection
for myelinolysis in the pons is thought to be a result of the grid arrangement of the
oligodendrocytes in the base of pons, which limits their mechanical flexibility and,
therefore, their capacity to swell. During hyponatremia, these cells can adapt only by
losing ions instead of swelling. This limitation makes them prone to damage when Na is
replaced. The risk factors mentioned above make normal adaptation difficult.
Clinical manifestations of CPM
Ataxia
Coma
Depressed or absent reflexes
Dysarthria
Dysphasia
Lethargy
Ophthalmoplegia
Quadriparesis
Clinical manifestations of EPM
Akinesis
Ataxia
Catatonia
Choreoathetosis
Cogwheel rigidity
Disorientation
Dysarthria
Dystonia
Emotional lability
Extra pyramidal symptoms
Gait disturbance
Movement disorders
Mutism
Myoclonus
Myokymia
Parkinsonism
Rigidity
Tremor
Diagnosis of CPM
The diagnosis of CPM is based on clinical suspicion and confirmed with imaging studies. MRI is
the primary method for diagnosis and is superior to CT. During the acute phase, symmetrical and
hypointense lesions can be identified on a T1-weighted MRI. During the subacute phase,
symmetrical and hypointense lesions are seen on T2-weighted images. Lesions on MRI may
appear days to weeks after the onset of symptoms; in some cases, these may resolve, over
months.
Management
At present, supportive treatment is all that can be recommended with certainty.
Therefore, prevention becomes important because hyponatremia is preventable and
causes neurologically significant morbidity and mortality.
To the authors' knowledge, no trials for the treatment of ODS have been conducted.
Small case series or single case reports of treatments, including steroids, IV
immunoglobulin, and thyrotrophin-releasing hormone, have all shown good outcomes.
However, the results are difficult to interpret because of the lack of clinical trials.
Prognosis
Older reports of ODS indicated almost a 100% mortality rate within 3 months after
hospital admission.
More recent studies of ODS reveal a relatively mild clinical course without substantial
neurologic deficits in survivors.
Patient Education
Advise parents not to replace diarrheal fluid loss with hypotonic fluids such as tea or
soda.
Pediatrics Hyperkalemia
Background
Hyperkalemia is defined as a serum potassium concentration greater than the upper limit of the
normal range; the range in children and infants is age-dependent, whereas the range for adults is
approximately 3.5-5.5 mEq/L. The upper limit may be considerably high in young or premature
infants, as high as 6.5 mEq/L[1] . Because hyperkalemia can cause lethal cardiac arrhythmia, it is
one of the most serious electrolyte disturbances.
Pathophysiology
Potassium is the primary intracellular cation; more than 95-98% of the total body potassium is
found in the intracellular space, primarily in muscle. Normal homeostatic mechanisms serve to
precisely maintain the serum potassium level within a narrow range. The primary mechanisms
for maintaining this balance are the buffering of extracellular potassium against a large
intracellular potassium pool (via the sodium-potassium pump) and urinary excretion of
potassium.
Under normal, nonpathologic conditions, approximately 90% of potassium excretion occurs in
the urine, with less than 10% of potassium excreted through sweat or stool. Within the kidneys,
potassium excretion occurs mostly in the principal cells of the cortical collecting duct (CCD).
Urinary potassium excretion depends on adequate luminal sodium delivery to the distal
convoluted tubule (DCT) and CCD, as well as the effect of aldosterone and other adrenal
corticosteroids with mineralocorticoid activity.
Laboratory hyperkalemia (fictitious or pseudohyperkalemia) can easily occur because of
hemolysis, tissue lysis, and "milking" of extremities (which can introduce a significant amount
of interstitial fluid into the blood sample) during phlebotomy, especially with heel-poke and
finger-stick phlebotomy, which are commonly performed in infants and small children.
Hemolysis can also be caused by fist clenching during phlebotomy or during prolonged
tourniquet application, which can also lead to an acidotic sample with resultant hyperkalemia).
Blood sampled "upstream" of an intravenous line with potassium-containing fluid (or from a
multiple lumen central venous catheter where the sampling lumen is near the lumen containing
potassium-rich infusate) can have falsely elevated levels of potassium that do not reflect
circulating levels.
Similarly, serum potassium levels may be falsely lowered by sampling upstream of a catheter
delivering fluid deficient in potassium or when a small blood sample is obtained and placed in
testing media low in potassium, which may be the case with specific point-of-care analyzers.[2]
When in doubt, blood samples should be obtained and tested using standard methods.
Thrombocytosis can also lead to false elevations of serum potassium levels. The normal serum
potassium level is 0.4 mEq/L higher than the plasma level because of potassium release during
clot formation. For every 100,000/mL elevation in the platelet count, the serum potassium
increases by approximately 0.15 mEq/L. This can easily be corrected based on a measurement of
whole blood potassium level. A similar effect on serum but not plasma potassium can also be
seen with leukocytosis.
True hyperkalemia is caused by one of 3 basic mechanisms, although the root cause for any
individual patient is often multifactorial.
Increased K+ intake: Increased K+ intake is most commonly caused by intravenous or oral
potassium supplementation. Packed RBCs (PRBCs) also carry potentially high
concentrations of potassium that can lead to hyperkalemia during PRBC transfusion[3] .
Since serum potassium levels represent only a small percentage (usually < 2-5%) of total
body potassium stores, long-term increases in potassium intake are only rarely associated
with significant serum hyperkalemia, unless excretion is inadequate.
Decreased potassium excretion: The most common cause of decreased potassium
excretion leading to hyperkalemia is oliguric renal failure. Other causes include primary
adrenal disease (eg, Addison disease, salt-wasting forms of congenital adrenal
hyperplasia), hyporeninemichypoaldosteronism, renal tubular disease
(pseudohypoaldosteronismI[4] or II), or medications (eg, ACE inhibitors, angiotensin II
blockers, spironolactone or other potassium-sparing diuretics).
Transcellular potassium shifts: In a transcellular potassium shift, a hydrogen ion enters a
cell and leads to decreased K+ uptake by the cell in order to maintain electrical neutrality.
Acidosis is the most common cause of hyperkalemia due to transcellular potassium shift,
but any process that leads to cellular injury or death (eg, tumor lysis syndrome,
rhabdomyolysis, crush injury, massive hemolysis) can cause hyperkalemia, as
intracellular potassium is released by disruption of the cell membrane. Other causes of
hyperkalemia due to transcellular shift of potassium include propofol ("propofol infusion
syndrome"),[5] toxins (digitalis intoxication or fluoride intoxication), succinylcholine,
beta-adrenergic blockade, strenuous or prolonged exercise, insulin deficiency, malignant
hyperthermia, and hyperkalemic periodic paralysis.
Plasma potassium levels are generally maintained at 3.5-5 mEq/L in adults, with higher levels in
neonates and small infants. levels greater than 7 mEq/L can lead to significant hemodynamic and
neurologic consequences, while levels exceeding 8.5 mEq/L can cause respiratory paralysis or
cardiac arrest and can quickly be fatal. High levels of potassium cause abnormal heart and
skeletal muscle function by lowering cell-resting action potential and preventing repolarization,
leading to muscle paralysis. Classic ECG findings begin with tenting of the T wave (as is shown
in the image below), followed by lengthening and eventual disappearance of the P wave and
widening of the QRS complex.[6]
Peaked T waves.
Prior to asystole, the QRS and T wave may merge to form a sinusoidal wave (as is shown in the
image below).
Sinusoidal wave.
Table. Select Factors Affecting Plasma Potassium (Open Table in a new window)
Factor
Aldosterone
Insulin
Effect on
Plasma K+
Decrease
Decrease
Mechanism
Increases sodium resorption, and increases K+ excretion
Stimulates K+ entry into cells by increasing sodium efflux
(energy-dependent process)
Beta-adrenergic
agents
Alpha-adrenergic
agents
Acidosis (decreased
pH)
Alkalosis (increased
pH)
Cell damage
Succinylcholine
Decrease
Increases skeletal muscle uptake of K+
Increase
Impairs cellular K+ uptake
Increase
Impairs cellular K+ uptake
Decrease
Enhances cellular K+ uptake
Increase
Increase
Intracellular K+ release
Cell membrane depolarization
Epidemiology
Frequency
United States
Hyperkalemia is a manifestation of a disease and is not a disease by itself. The incidence of
hyperkalemia in the pediatric population is unknown, although the prevalence of hyperkalemia in
extremely low birth weight premature infants can exceed 50%.[7] Hyperkalemia in pediatric
patients is most commonly associated with renal insufficiency, acidosis, and with diseases that
involve defects in mineralocorticoid, aldosterone, and insulin function.[8]
Mortality/Morbidity
Sudden and rapid onset of hyperkalemia can be fatal. With slow or chronic increase in potassium
levels, adaptation occurs via renal excretion, with fractional potassium excretion increasing by as
much as 5-10 times the reference range.
Race
No racial predilection is observed.
Sex
No sex-related predilection is observed. However, neuromuscular disorders including myotonic
and muscular dystrophies and related disorders that can predispose patients to hyperkalemia with
succinylcholine administration are more prevalent in males.[9]
Age
Extremely low birth weight premature infants are particularly prone to hyperkalemia primarily
due to immature renal function. Even otherwise full-term infants may have transient
hyperkalemia and hyponatremia due to decreased responsiveness to aldosterone
(pseudohypoaldosteronism I).
History
History for a previously well child with acute hyperkalemia should focus on how the blood
sample was obtained, potassium intake or recent blood product transfusion, risk factors for
transcellular shift of potassium (acidosis) or tissue death/necrosis, medication use (by the child,
other family members, pets, etc) associated with hyperkalemia, and presence or signs of renal
insufficiency.
Specific questions may be focused on the following:
Urine output (last void or number of wet diapers) and fluid intake
Cola-colored urine (which may indicate acute glomerulonephritis)
Bloody stool (which may indicate hemolytic-uremic syndrome [HUS])
Presence of drugs in the household (or used by recent visitors), such as potassium
preparations, digoxin, and diuretics
Any history of trauma (crush injuries) or thermal injury (burns)
Medical history, family history, and review of systems should be explored for any of the
following:
Acute or chronic renal failure
Hypertension
Diabetes
Adrenogenital syndromes
Malignancy (tumor lysis syndrome)
Family history (hyperkalemic periodic paralysis, miscarriages, deaths of very young siblings)
Neuromuscular disorders
Malignant hyperthermia
Physical
High potassium levels interfere with repolarization of the cellular membrane following
completion of the action potential. Findings depend on the degree of hyperkalemia and primarily
relate to the deleterious effects of elevated plasma potassium levels on cardiac conduction.
Children with hyperkalemia can present with cardiac arrest due to wide-complex tachycardia or
ventricular fibrillation.
Symptoms short of circulatory collapse/cardiac arrest include respiratory failure and weakness
that progresses to paralysis. Patients may report nausea, vomiting, and paresthesias (eg, tingling).
Most often, patients with hyperkalemia are asymptomatic, with the first clinical manifestation of
the condition either ECG changes (peaked T waves) or sudden cardiac arrest.
Nonspecific findings can include muscle weakness (skeletal, respiratory), fatigue, ileus with
hypoactive or absent bowel sounds, and depression.
Causes
Although the etiology of hyperkalemia can be multifactorial, differential diagnoses include
fictitious hyperkalemia and hyperkalemia due to increased potassium intake, transcellular
potassium shift, or decreased potassium excretion.
Fictitious hyperkalemia
o Hemolysis, tissue lysis, or tissue ischemia during phlebotomy
o Contamination of blood sample with potassium-containing fluids
o Thrombocytosis or leukocytosis (affects serum K+ but not plasma K+)
Hyperkalemia due to increased K+ intake
o Blood transfusion (increasing risk with increased duration of cell storage)
o Intravenous (IV) or oral potassium
o Maintenance K+ in IV or oral solutions combined with decreased renal function
Hyperkalemia due to transcellular K+ shift
o Metabolic acidosis
o Beta-adrenergic blockade[10, 11]
o Acute tubular necrosis
o Electrical burns
o Thermal burns
o Cell depolarization
o Head trauma
o Rhabdomyolysis
o Digitalis toxicity
o Fluoride toxicity[12]
o Cyclosporin A[13]
o Methotrexate[14]
o Propofol infusion syndrome
o Tumor lysis syndrome
o Succinylcholine use in a child with neuromuscular disease, prolonged bed rest
(including patients in ICUs), or more than 24 hours after crush or burn injury[15]
Hyperkalemia due to decreased K+ excretion
o Acute renal failure
o Primary adrenal disease (Addison disease, salt-wasting congenital adrenal
hyperplasia)
o Hyporeninemichypoaldosteronism
o Renal tubular disease
Medications (eg, potassium sparing diuretics, ACE inhibitors, angiotensin II blockers,
trimethoprim, nonsteroidal anti-inflammatory agents [NSAIDs])
Differential Diagnoses
Acidosis, Metabolic
Acute Tubular Necrosis
Burns, Electrical
Burns, Thermal
Congenital Adrenal Hyperplasia
Head Trauma
Rhabdomyolysis
Toxicity, Digitalis
Tumor Lysis Syndrome
Laboratory Studies
Laboratory studies depend on the etiology of hyperkalemia but may include the following:
Serum electrolyte tests
Serum BUN and creatinine tests
Urinalysis (UA)
Depending on the etiology or on clinical suspicion, other studies to consider include the
following:
Arterial or free-flowing venous blood gas sampling (for acid-base disorders): Capillary
blood gas sampling should not routinely be used to evaluate for hyperkalemia due to
significant risks of factitious hyperkalemia.
Serum uric acid and phosphorous tests (for tumor lysis syndrome)
Serum creatinine phosphokinase (CPK) and calcium measurements (for rhabdomyolysis)
Urine myoglobin test (for crush injury or rhabdomyolysis; suspect if UA reveals blood in
the urine but no RBCs are seen on urine microscopy)
Specific drug level tests for suspected toxicity (digoxin)
CBC count (for thrombocytosis, leukocytosis, or malignancy)
Urine electrolyte tests, including potassium and osmolality (osm) tests
Plasma osm test
When the etiology of hyperkalemia remains unclear, calculation of the transtubular potassium
gradient (TTKG) using the following formula may be useful: TTKG = (K+ urine X Osm
plasma)/(K+ plasma X Osm urine)
The normal TTKG varies from 5-15. In the setting of hyperkalemia with normal renal excretion
of potassium, the TTKG should be greater than 10. A TTKG of less than 8 in the setting of
hyperkalemia implies inadequate potassium excretion, which is usually secondary to aldosterone
deficiency or unresponsiveness. Checking a serum aldosterone level may be helpful.
Imaging Studies
Imaging studies are not generally indicated, except to assess the primary disease state (eg,
excluding obstructive uropathy as a cause for acute renal failure).
Other Tests
An ECG is essential in all children in whom hyperkalemia is suspected. ECG reveals the
sequence of changes as follows:
Serum K+ 5.5-6.5 mEq/L - Tall, peaked T waves with narrow base, best seen in precordial leads
(as is shown in the image below)
Peaked T waves.
Serum K+ 6.5-8.0 mEq/L - Peaked T waves, prolonged PR interval, decreased or disappearing P
wave, widening of QRS, amplified R wave
Serum K+ greater than 8.0 mEq/L - Absence of P wave; progressive QRS widening,
intraventricular/fascicular/bundle branch blocks; progressive widening of QRS, eventually
merging with the T wave just before cardiac arrest, forming the sine wave pattern (as is shown in
the image below)
Sinusoidal wave.
dical Care
Hyperkalemia is a true medical emergency, with 3 primary goals of immediate management (in
addition to prompt discontinuation of potassium-containing fluids and medications that lead to
hyperkalemia):[16]
Stabilize the myocardial cell membrane to prevent lethal cardiac arrhythmia (and to gain
time to shift potassium intracellularly and enhance potassium elimination - Intravenous
(IV) calcium chloride or gluconate
Enhance cellular uptake of potassium
o Sodium bicarbonate IV
o Regular insulin and glucose IV
o Beta-adrenergic agents, such as albuterol (used to manage hyperkalemia with
variable results), terbutaline, dobutamine
Enhancing total body potassium elimination
o Sodium polystyrene sulfonate (Kayexalate) orally (PO)/rectally (PR)
o Furosemide (only if renal function is maintained)
o Emergent hemodialysis
Arrhythmias due to hyperkalemia are very difficult to treat with defibrillation, epinephrine, or
antiarrhythmic drugs without emergently lowering the serum potassium level.
After initial stabilization, further workup should be performed to diagnose the etiology of the
hyperkalemia. Children with acquired Addison disease or other primary adrenal disease require
stress-dose steroid supplementation and children with hypoaldosteronism require
mineralocorticoid supplementation.
Emergent hemodialysis is sometimes necessary to treat severe symptomatic hyperkalemia that is
resistant to drug therapy, particularly in patients without adequate renal function.
Even in patients with severe hyperkalemia and a high gradient, peritoneal dialysis (PD) is
not as efficient as hemodialysis in the removal of potassium. Rates of removal with PD
are almost equal to the removal rate using sodium polystyrene sulfonate (Kayexalate).
Continuous arteriovenous hemofiltration with dialysis (CAVHD) or continuous venovenous hemofiltration with dialysis (CVVHD) have also been used to remove potassium.
However, potassium removal with these methods is similar to that of PD and sodium
polystyrene sulfonate (Kayexalate). CVVHD or CAVHD may be used for long-term
removal of potassium, but in acute, severe, life-threatening hyperkalemia unresponsive to
medical therapy, hemodialysis remains the procedure of choice.
Surgical Care
Tumor debulking may be considered to decrease the risk of hyperkalemia from tumor lysis
syndrome for solid tumors.[17]
Consultations
Consultations with the following specialists may be necessary in cases of hyperkalemia that
result from certain conditions or disease states:
Pediatric intensivist or neonatologist - Management of life-threatening hyperkalemia
(hyperkalemia with ECG changes)
Nephrologist - Hyperkalemia associated with renal failure
Hematologist/oncologist - Hyperkalemia resulting from tumor lysis syndrome
Social services specialist - Children who develop hyperkalemia following unintentional
ingestions or poisonings
Nutritional support specialist - Particularly for patients whose hyperkalemia is caused by
renal failure, which requires close regulation of potassium and sodium intake
Endocrinologist - Patients with suspected mineralocorticoid abnormalities such as
congenital adrenal hyperplasia
Diet
Potassium intake must be closely monitored (and possibly restricted) in patients with renal
failure.
Medication Summary
Myocardium stabilizers
Intracellular transporters
Alkalinizing agents
Exchange resins
Multimedia Library
Tables
References
Medication Summary
Treatment for severe hyperkalemia consists of 3 steps: (1) immediate stabilization of the
myocardial cell membrane, (2) rapidly shifting potassium intracellularly, and (3) enhancing total
body potassium elimination (see Medical Care).
In addition, all sources of exogenous potassium should be immediately discontinued; including
intravenous (IV) and oral (PO) potassium supplementation, total parenteral nutrition, and any
blood product transfusion. Drugs associated with hyperkalemia should also be discontinued.
Albuterol and other beta-adrenergic agents induce the intracellular movement of potassium via
the stimulation of the sodium/potassium–adenosine triphosphate (Na+/K+ -ATP) pump. Studies
have shown that IV salbutamol (not available in the United States) is highly effective in lowering
serum potassium levels. Some studies in adults and children using nebulized albuterol indicate
that this method of therapy is effective in lowering serum potassium levels. However, peak
response is unclear; therefore, it has not been established as the first line of therapy in severe
hyperkalemia.
Myocardium stabilizers
Class Summary
Calcium does not lower serum potassium levels. It is primarily used to protect the myocardium
from the deleterious effects of hyperkalemia (ie, arrhythmias) by antagonizing the membrane
actions of potassium.
View full drug information
Calcium chloride
IV calcium is indicated in all cases of severe hyperkalemia (ie, >7 mEq/L), especially when
accompanied by ECG changes. Calcium chloride contains about 3 times more elemental calcium
than an equal volume of calcium gluconate. Therefore, when hyperkalemia is accompanied by
hemodynamic compromise, calcium chloride is preferred over calcium gluconate.
Administration of calcium should be accompanied by the use of other therapies that actually help
lower the K+ serum levels.
Other calcium salts (eg, glubionate, gluceptate) have even less elemental calcium than calcium
gluconate and are generally not recommended for therapy of hyperkalemia. Calcium chloride 1 g
= 270 mg (13.5 mEq) of elemental calcium.
Calcium gluconate 1 g = 90 mg (4.5 mEq) of elemental calcium.
Intracellular transporters
Class Summary
Regular insulin and glucose cause a transcellular shift of potassium into muscle cells, thereby
temporarily lowering K+ serum levels.
Insulin and dextrose, IV
Regular insulin presence results in intracellular movement of glucose, followed by K+ entry into
muscle cells. Although effect is almost immediate, it is temporary, and, therefore, should be
followed by therapy that actually enhances potassium clearance (eg, sodium polystyrene
sulfonate).
Alkalinizing agents
Class Summary
Sodium bicarbonate IV is used as a buffer that breaks down to water and carbon dioxide after
binding free hydrogen ions.
View full drug information
Sodium bicarbonate
IV infusion helps shift K+ into cells, further lowering serum K+ levels. Can be considered in
treatment of hyperkalemia even in absence of metabolic acidosis. Also increases sodium delivery
to the kidney, which assists in potassium excretion.
Exchange resins
Class Summary
Sodium polystyrene sulfonate is an exchange resin that can be used to treat mild-to-moderate
hyperkalemia. Each mEq of potassium is exchanged for 1 mEq of sodium.
View full drug information
Sodium polystyrene sulfonate (Kayexalate)
Exchanges sodium for potassium and binds it in the gut, primarily in large intestine, and
decreases total body potassium. Onset of action after PO administration ranges from 2-12 hours
and is longer when administered PR.
Do not use as a first-line therapy for severe life-threatening hyperkalemia. Use in second stage of
therapy to reduce total body potassium
Pediatrics Hypokalemia
Background
Potassium is the most abundant intracellular cation and is necessary for maintaining a normal
charge difference between intracellular and extracellular environments. Potassium homeostasis is
integral to normal cellular function and is tightly regulated by specific ion-exchange pumps,
primarily by cellular, membrane-bound, sodium-potassium adenosine triphosphatase (ATPase)
pumps. Derangements of potassium regulation may lead to neuromuscular, GI, and cardiac
conduction abnormalities.
Hypokalemia is generally defined as a serum potassium level of less than 3.5 mEq/L in children,
although exact values for reference ranges of serum potassium are age-dependent, and vary
among laboratories. It is frequently present in pediatric patients who are critically ill and reflects
a total body deficiency of potassium or, more commonly, reflects conditions that promote the
shift of extracellular potassium into the intracellular space.
Pathophysiology
Hypokalemia may be due to a total body deficiency of potassium, which may result from
prolonged inadequate intake or excessive losses (including but not limited to, long-term
diureticor laxative use, and chronic diarrhea, hypomagnesemia, or hyperhidrosis). Acute causes
of potassium depletion include diabetic ketoacidosis,[1] severe GI losses due to vomiting and
diarrhea, dialysis, and diuretic therapy.
Hypokalemia may also be the manifestation of large potassium shifts from the extracellular to
intracellular space, as seen with alkalosis, insulin, catecholamines (including albuterol and other
commonly-used beta2-adrenergic agonists),sympathomimetics, and hypothermia.
Other recognizable causes include renal tubular disorders, such as distal renal tubular acidosis,
Bartter syndrome,[2] and Gitelman syndrome, periodic hypokalemic paralysis, hyperthyroidism,
andhyperaldosteronism.
Other mineralocorticoid excess states that may cause hypokalemia include cystic fibrosis (with
hyperaldosteronism from severe chloride and volume depletion), Cushing syndrome, and
exogenous steroid administration. Excessive natural licorice consumption can also cause or
exacerbate potassium loss due to inhibition of 11-betahydoxysteroid dehydrogenase, which leads
to elevated endogenous mineralocorticoid activity.[3]
Epidemiology
Mortality/Morbidity
Mortality is rare, except when hypokalemia is severe or occurs following cardiac surgery, when
accompanied by arrhythmia, or in patients who have underlying heart disease and require
digoxin therapy.
Short-term morbidity is common and may include GI hypomotility or ileus; cardiac dysrhythmia;
QT prolongation; appearance of U waves that may mimic atrial flutter, T-wave flattening, or STsegment depression; and muscle weakness or cramping.
Mortality and morbidity can also be related to treatment for hypokalemia with potassium
supplementation, particularly if potassium is given in large doses or rapidly. Because of the risk
associated with potassium replacement, alleviation of the cause of hypokalemia may be
preferable to treatment, especially if hypokalemia is mild, asymptomatic, or transient and is
likely to resolve without treatment.
Race
Racial differences may be present in predisposing conditions such as Bartter syndrome, Gitelman
syndrome, Conn syndrome (ie, hyperaldosteronism), Cushing syndrome, and familial
hypokalemic paralysis. In addition, significant hypokalemia and hypokalemic paralysis develop
in 2-8% of Asians with hyperthyroidism.
Sex
No known sex predilection has been noted.
Age
Viral GI infections tend to be more common in infants and younger children. Younger children
with emesis or diarrhea are at an increased risk of hypokalemia because the depletion of fluid
volume and electrolytes from GI loss is relatively higher than that found in older children and
adults.
Insulin-dependent diabetes mellitus that results in diabetic ketoacidosis (with its inherent fluid
and potassium loss) is more common in children. Excessive corticosteroid and mineralocorticoid
secretion, as in Cushing syndrome and Conn syndrome, is a less common cause of hypokalemia
in the pediatric patient. Periodic hypokalemic paralysis may appear in childhood or young
adulthood, precipitated by rest after strenuous exercise, physical or metabolic stress (eg,
exposure to cold, alcohol ingestion), a high-carbohydrate meal, or exposure to exogenous insulin
or catecholamines (eg, epinephrine and albuterol). Hypokalemia due to hyperthyroidism is
generally observed in adults.
History
Hypokalemia due to excessive loss is usually accompanied by a history of GI loss
(emesis or diarrhea), urinary output, or sweating. This may be exacerbated by inadequate
oral intake.
Query about current or recent treatment with medications and herbal products (especially
natural licorice), including insulin, albuterol or other beta2-sympathomimetics,
corticosteroids, diuretics, laxatives,enemas, or bowel-prep solutions. A complete and upto-date medication and supplement list is essential, especially if the patient is taking new
medications or may have had medication substitutions.
The patient may have had similar episodes in the past. Familial historical data may
include surgery for pituitary or adrenal tumors or acute intermittent episodes of paralysis,
with or without association with hyperthyroidism.
Periodic familial hypokalemia
Physical
Physical examination findings may frequently be within the reference range.
Occasionally, muscle weakness is evident.
Cardiac arrhythmias and acute respiratory failure from muscle paralysis are lifethreatening complications that require immediate diagnosis.
Cardiovascular examination findings may also be within normal limits. Occasionally,
tachycardia with irregular beats may be heard. Severe hypokalemia may manifest as
bradycardia with cardiovascular collapse.
Hypoactive bowel sounds may suggest hypokalemic gastric hypomotility or ileus.
Causes
Hypokalemia may be due to a total body deficit of potassium, which may occur
chronically with the following:
o Prolonged diuretic use
o Inadequate potassium intake
o Laxative use
o Diarrhea (including congenital chloride diarrhea)[4]
o Hyperhidrosis
o Hypomagnesemia
o
Renal tubular losses (including Fanconi syndrome,[5] Bartter syndrome, Gitelman
syndrome, and others)
o Dengue syndrome[6]
Acute causes of potassium depletion include the following:
o Diabetic ketoacidosis
o Severe GI losses from vomiting and diarrhea
o Dialysis and diuretic therapy
o Alcohol intoxication/overdose[7]
Hypokalemia may also be due to excessive potassium shifts from the extracellular to the
intracellular space, as seen with the following:
o Alkalosis
o Insulin use
o Catecholamine use
o Sympathomimetic use
o Use of sodium bicarbonate, especially during therapeutic alkalinization
(commonly used to treat salicylate and cyclic antidepressant overdoses, tumor
lysis syndrome, rhabdomyolysis, etc)
o Use of sodium polystyrene sulfonate to treat transient hyperkalemia
o Hypothermia
Other recognizable causes of hypokalemia include the following:
o Renal tubular disorders, such as Bartter syndrome and Gitelman syndrome
o Type I or classic distal tubular acidosis
o Periodic hypokalemic paralysis
o Hyperaldosteronism
o Celiac disease[8]
Other states of mineralocorticoid excess that may cause hypokalemia include the
following:
o Cystic fibrosis with hyperaldosteronism from severe chloride and volume
depletion
o Cushing syndrome
o Exogenous steroid administration, including fludrocortisone and other
mineralocorticoids
o Excessive licorice consumption[3]
Other conditions that may cause hypokalemia include acute myelogenous,
monomyeloblastic, or lymphoblastic leukemia.
Drugs that may commonly cause hypokalemia include the following:
o Furosemide, bumetanide, and other loop diuretics
o Methylxanthines (theophylline, aminophylline, caffeine)
o Verapamil (with overdose)
o Amphotericin B, micafungin[9]
o Quetiapine (particularly in overdose)
o Ampicillin, carbenicillin, high-dose penicillins[10]
o Sirolimus[11]
o Drugs associated with magnesium depletion, such as aminoglycosides,
amphotericin B, and cisplatin
Differential Diagnoses
Bartter Syndrome
Hyperthyroidism
Hypochloremic Alkalosis
Hypomagnesemia
Metabolic Alkalosis
Laboratory Studies
The following studies are indicated in patients with hypokalemia:
Serum electrolyte tests: Screen for concurrent electrolyte abnormalities, which may affect
treatment.
Blood gas analysis
o Assess acid-base status.
o Alkalosis may induce hypokalemia, and treatment of acidosis may worsen
existing hypokalemia.
Drug screen (serum or urine)
o Amphetamines and other sympathomimetic stimulants can cause hypokalemia.
o Other drugs that can cause hypokalemia include verapamil (with overdose),
theophylline, amphotericin B, aminoglycosides, and cisplatin.
Serum adrenocorticotropic hormone (ACTH), cortisol, renin activity, and aldosterone
tests: Evaluate for suspected Cushing, Conn, or adrenal hyperplasia syndromes, including
11-beta-hydroxylase deficiency.
Simultaneous serum insulin and C-peptide tests: Because hyperinsulinism can cause
transient hypokalemia, elevated serum insulin without appropriately elevated C-peptide
suggests exogenous insulin administration, which may represent Münchhausen-by-proxy
syndrome.
Imaging Studies
MRI: Perform brain MRI if a brain or pituitary tumor is suspected as a cause of
hypercortisolism.
Ultrasonography and CT scanning: Perform abdominal ultrasonography or CT scanning
if an adrenal tumor or hyperplasia is suspected.
Other Tests
Although ECG changes may be helpful if present, their absence should not be taken as
reassurance of normal cardiac conduction.[12]
The ECG in hypokalemia may appear normal or may have only subtle findings
immediately before clinically significant dysrhythmias.
ECG findings may include the following (see the image below):
o
o
o
o
Ventricular dysrhythmia
Prolongation of QT interval
ST-segment depression
T-wave flattening
o
Appearance of U waves
Prominent U waves after T
waves in hypokalemia.
During therapy, monitor for changes associated with overcorrection and hyperkalemia,
including a prolonged QRS, peaked T waves, bradyarrhythmia, sinus node dysfunction,
and asystole.
Medical Care
The treatment of hypokalemia depends on severity and etiology.
Unlike hyponatremia, in which the total body sodium deficit can be readily estimated,
serum potassium may not accurately reflect total body stores. Indeed, during diabetic
ketoacidosis, serum potassium levels are usually initially elevated, even in the face of
severe depletion of total body potassium. Correction of acidosis in diabetic ketoacidosis
may cause a precipitous drop in serum potassium levels.
Treatment of hypokalemia should be directed at the etiology of hypokalemia as well as its
correction, as treatment of hypokalemia carries with it a significant risk of iatrogenic
hyperkalemia.
Transient, asymptomatic, or mild hypokalemia may spontaneously resolve or may be
treated with enteral potassium supplements.
Symptomatic or severe hypokalemia should be corrected with a solution of intravenous
potassium.
Whenever practical, treatment of hypokalemia should be performed in a monitored
setting with medications and personnel available to intervene in the event that treatment
results in symptomatic hyperkalemia.
Surgical Care
Except for excision of tumors leading to hypokalemia, management is nonsurgical.
Consultations
After resolution, consultation with subspecialists (including, but not limited to,
endocrinologist, nephrologist, pulmonologist, gastroenterologist, geneticist, or specialist
in metabolic disease) may be necessary to diagnose and manage predisposing conditions.
Consultation with a dietitian may be helpful in cases of hypokalemia due to inadequate
dietary intake.
Consultation with mental health professionals may be necessary for ongoing treatment of
hypokalemia secondary to anorexia and/or bulimia.
Diet
Dietary modification may be necessary for patients with excessive potassium losses (eg,
diuretic or laxative use) or patients with hypokalemia who are at increased risk, such as
those receiving digoxin.
Avoidance of specific foods (eg, licorice) may also be necessary for high-risk individuals.
Activity
Patients with hypokalemic periodic paralysis may need to modify exercise regimens to
avoid periods of strenuous exercise.
Patients at risk of hypokalemia from sweat losses should have adequate potassium and
fluid available during activities likely to result in significant sweating and should be
given anticipatory guidance regarding symptoms of hypokalemia.
Medication Summary
Potassium supplements
Class Summary
These agents are used to restore body potassium storage. Electrolytes are used to correct
disturbances in fluid and electrolyte homoeostasis or acid-base balance and to reestablish
osmotic equilibrium of specific ions.
View full drug information
Potassium chloride (also citrate, acetate, bicarbonate, gluconate)
Potassium chloride is the preferred salt for patients with preexisting alkalosis. First
choice for IV therapy. Essential for transmission of nerve impulses; contraction of
cardiac muscle; and maintenance of intracellular tonicity, skeletal and smooth muscles,
and normal renal function. Gradual potassium depletion occurs via renal excretion,
through GI loss, or because of low intake. Depletion may result from diuretic therapy,
primary or secondary hyperaldosteronism, diabetic ketoacidosis, severe diarrhea,
vomiting, or inadequate replacement during prolonged parenteral nutrition.
Medical therapy is aimed at potassium supplementation by the enteral (ie, oral or through
feeding tubes) or parenteral route. Transient, asymptomatic, or mild hypokalemia may
resolve spontaneously, or it may be treated using enteral potassium supplements.
Symptomatic or severe hypokalemia should be corrected with intravenous potassium
preparations.
Further Inpatient Care
After the initial phase of hypokalemia therapy is completed, focus further inpatient care
on matching potassium intake to losses, periodic testing of serum potassium levels, and
electrocardiographic monitoring for hypokalemia or hyperkalemia due to therapy.
Alleviation of aggravating conditions, simplification of medication administration, and
patient education form the basis of ongoing patient health and safety.
Further Outpatient Care
If the condition is expected to persist beyond inpatient care, patients should receive
follow-up medical care for home treatment.
Additional medical follow-up must be obtained for associated medical conditions.
Inpatient & Outpatient Medications
Other than potassium supplementation as described above, no additional medications are
required.
If current medications are responsible for hypokalemia, substitution of potassium-sparing
alternatives may help reduce degree of hypokalemia and may help minimize
requirements for potassium supplementation.
Transfer
Patients with severe or symptomatic hypokalemia require transfer to an ICU for
intravenous potassium supplementation and continuous electrocardiographic monitoring.
Deterrence/Prevention
Because many medications (particularly loop diuretics, mineralocorticoids,
catecholamines, methylxanthines, alkalinizing agents) may be responsible for
hypokalemia, eliminating or reducing the doses of these medications may be helpful in
preventing or minimizing hypokalemia.
Complications
Hyperkalemia due to excessive/rapid potassium replacement
Cardiac dysrhythmia
Gastric erosions
Strictures
Prognosis
With adequate control of potassium levels and resolution of any predisposing condition,
prognosis is excellent.
Patient Education
Patients should be educated in terms of predisposing conditions. The importance and
risks involved with potassium supplementation and the warning signs of hypokalemia or
overtreatment must be emphasized upon discharge from the hospital.
Knowledge of cardiopulmonary resuscitation and education on timely access to
emergency medical services may prevent morbidity or mortality.
Ongoing communication is essential for reducing the risks and in therapy, especially in
patients with chronic conditions associated with hypokalemia.
For excellent patient education resources, see the Endocrine System Center, as well as
Low Potassium.