Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
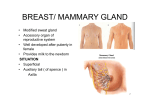
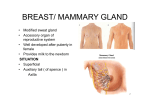
ANATOMY OF THE AXILLA Omar Z. Youssef M.D A. Professor of surgical oncology NCI-‐ Cairo University Contents of the axilla • Axillary Fat • Axillary Lymph Nodes • Axillary Vein • Axillary Artery • Brachial Plexus Boundaries of Axillary Fossa: 1. Clavicle: Anteriorly 2. Scapula: posteriorly 3. 1st rib: medially Walls of Axillary Fossa 1. Anterior wall: • 1st layer: pectoralis major muscle & pectoral fascia • 2nd layer: subclavius muscle • clavipectoral fascia (costocoracoid membrane). • pectoralis minor muscle • suspensory ligament of axilla Walls of Axillary Fossa 2. Posterior wall: • subscapularis muscle -‐ forms majority, esp. medially • teres major muscle -‐ form inf. & lat. porPon of posterior wall • laPssimus dorsi muscle 3. Medial wall: • upper 4 or 5 ribs. intercostal spaces (intercostal muscles & membranes). • above covered by serratus anterior muscle 4. Lateral wall: • bicipital groove of humerus, containing (musculotendinous) porPon • coracobrachialis muscle • biceps brachii muscle Axillary artery • • • • • • • • • 1st part: superior thoracic artery 2nd part: thoracoacromial artery (trunk) long thoracic artery 3rd part: subscapular artery anterior circumflex humeral a. posterior circumflex humeral a Axillary Nodes 1. Anterior (pectoral) set -‐ (along the lat. thoracic v.) 2. Posterior (subscapular) set -‐ (subscap. V.) 3. Lateral (humeral) set -‐ (brachial v.) 4. Central set -‐ (axillary v.) 5. Apical (suprascap. or subclavian) set -‐ (upper axillary/subclavian v.) Axillary vein Brachial plexus Adequacy of ALND • NCCN : Level I and II and a minimum of 10 nodes removed • Controversy whether it is more important number of LN or the % between posiPve/total • Usually median number excised is higher • < 10 LN removed: – neoadjuvant treatment – increasing age – Surgeon experience/pathologist experience ComplicaPons • • • • • • • Lymphedema Axillary Web Syndrome Sensory Morbidity Shoulder FuncPon InfecPon Seroma Brachial Plexus Injury Lymphedema • Level I-‐III axillary nodes ~15-‐50% rates of lymphedema • Even with level I-‐II ~5-‐30% Lymphedema prevenPon • Mapping the Drainage of the Arm with Blue Dye: Axillary Reverse Mapping (ARM) Would ↓ the Likelihood of DisrupPon of the Arm LymphaPc and Subsequent Lymphedema. ComplicaPons • INFECTION Teijeirian et al. 2006-‐ meta-‐analysis Use of intraoperaPve anPbioPcs will lead to reducPon in infecPon (RR = 0.60) • HEMATOMA 2%-‐10%, although prospecPve trials 0%-‐2% • SEROMA Some degree in 100% -‐ not a complicaPon Delay in range of moPon balance against shoulder morbidity Axillary Web Syndrome (AWS) /Cording Incidence: • 6-‐72% following ALND • Reported afer SLNB Clinical picture: • thick, ropelike structures under the skin of axilla • pain and Pghtness • occurs anywhere from several days to several weeks afer surgery EPology ?? Management of Axillary Web Syndrome • Stretching and flexibility exercises • Manual therapy • Moist heat • Pain treatment Conclusion • Knowing the anatomy is crucial for performing an ALND • Several techniques are being developed in order to decrease morbidity from ALND Conclusion • Axillary dissecPon remains the standard approach to the paPent who presents with clinically evident nodal metastases. • Histologic confirmaPon of disease should be obtained by needle biopsy. • If metastases cannot be documented, SLND, including the removal of clinically abnormal nodes, should be carried out prior to proceeding with axillary dissecPon