Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
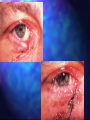
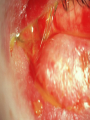
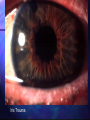
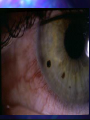
Ocular Trauma Sarah Welch Vitreoretinal Surgeon Eye Dept GLCC; Auckland Eye March 2011 Outline Assessment of Trauma Types of injury Peri-ocular Anterior segment Posterior segment Chemical injury Epidemiology 40% of monocular blindness is related to trauma The leading cause of monocular blindness 70-80% injured are male Age range is 0-100 yrs but most are young average age 30yr Incidence of penetrating eye injuries: 3.6/100000 Incidence of Eye injuries requiring hospitalisation: 15.2 /100000 Sources of Injury Blunt objects - 30-40% Motor Vehicle Injuries - 9% Play or sports - 1/3 rocks, fists, branches, champagne corks golf/squash balls, shoulder/elbow, bats/racquets, horse Falls - 4% Sharp objects - 18% Globe involvement in 22% of cases QuickTime™ and a decompressor are needed to see this picture. Assessment Rule out life threatening injuries Rule out globe threatening injuries Examine both eyes Image Plan for treatment History Mechanism of trauma blunt/penetrating/mixed forces involved Previous injuries Past ocular history Past medical history Examination Pt review are there life threatening injuries which need to be treated first? Facial Exam ?brain injury lacerations/bruising, numbness, weakness Ocular exam VA, lids and lacrimal system, orbital rim/orbital bones, ocular motility, globe, optic nerve Lids and orbits Assessment History Detailed as possible Time and nature of injury Past ocular history Missile, blunt, ? FB remaining, chemical etc Previous VA and lid function remember trauma is a recurrent pathology Med Hx ?tetanus, ? Anticoagulation Examination Rule out life threatening injuries Rule out globe threatening injuries Examine both eyes Assess lid trauma - document +/photos Plan for repair Examination - lids Tissue loss Layers of lid Lid Margin Canaliculi Prolapsed fat/septal involvement Levator function Lagophthalmos Canthal tendon/angle Image CT - fine cuts orbits If ? FB If unable to determine posterior aspect of wound If suspect orbital fracture/ other injuries Repair Timing Ideally within 12-24 hours of injury Can delay up to 1 week Patient factors Gross swelling – Ice packs to reduce – ? steroid Anaesthesia GA / LA Repair: General Principles Clean wound Remove FB Minimal debridement Careful handling of tissues Careful alignment of anatomy Lid margins, lash line, skin folds etc Close in layers Simple laceration Minor, partial thickness May be steri-stripped if not under tension Sutures 6.0/7.0 absorbable (gut or vicryl) or non absorbable Remove at 5 days if non absorbable Deep lacerations Repair in layers as needed Identify septum and do not attach to muscle,skin or tarsus risk of lid lag Lid Margin lacerations Approximate lid margin Tarsal plate first 6.0 vicryl suture - can use as traction 3-4 sutures to plate Spatulated needle is useful Align lashes - silk Skin - nylon or gut or vicryl Traumatic ptosis Trauma to levator aponeurosis and Mullers muscle To repair need to identify levator aponeurosis and reattach to tarsal plate GA (diffiult under LA) Beware involving septum Consider delayed repair (3/12) Canalicular Lacerations Upper Controversial (loss may not affect pt) Either repair laceration and ignore canaliculus, or Stent canaliculus (Mini Monoka) and repair lac Lower Usually needs to be repaired Repair within 24-48 hours Stent bicanalicular or monocanalicular Leave in for 3-6 months 8.0 or 9.0 vicryl to canaliculus Tissue Loss Explore wound thoroughly find all tissue Options Direct repair Tissue advancement Eg lateral canthotomy Advancement flaps Replace in layers Tarsoconjuntival flap and skin graft or vice versa Complications Lid margin notching Lagophthalmos Rare Tearing May improve with time Consider steroid injection into 4-6/52 Infection Due to scarring or tissue loss or septum into wound Try massage, may need scar release Hypertrophic scars If small may resolve, otherwise requires repair canalicular damage, lid malposition, pump failure Traumatic ptosis Myogenic or neurogenic Orbital Fractures Orbital #s classification Open or closed Internal (orbital skeleton), rim, complex (internal +rim) Type Blowout - typically 10-15mm behind rim, just medial infraorbital canal Tripod - disruption of zygoma at z-f and z-m sutures & along arch Enophthalmos, malar flattening, inf lat cantus displacement Pathogenesis of orbital floor blow-out fracture Evaluation of the orbit Eyelids Globe Displacement, proptosis Motility - ductions and diplopia, include FDT Pupil - APD, efferent, mydriasis Palpate Telecanthus - tendon disruption or nasoethmoidal #, suspect nld involvement Rim, crepitus, retropulsion Nerves - V1 & V2 Signs of orbital floor blow-out fracture • Periocular ecchymosis and oedema • Infraorbital nerve anaesthesia • Enophthalmos - if severe • Ophthalmoplegia typically in up- and downgaze (double diplopia) Imaging CT Axial and coronal 3mm sections 1.5 through apex if suspect TON MRI No good - bone, metal FB Subdural optic n haematoma Investigations of orbital floor blow-out Coronal CT scan • Right blow-out fracture with ‘tear-drop’ sign Hess test • Restriction of right upgaze and downgaze • Secondary overaction of left eye QuickTime™ and a decompressor are needed to see this picture. QuickTime™ and a decompressor are needed to see this picture. Surgical treatment of blow-out fracture a b c d (a) Subciliary incision • Coronal CT scan following repair of right blow-out fracture with synthetic (b) Periosteum elevated and entrapped material orbital contents freed (c) Defect repaired with synthetic material (d) Periosteum sutured Zygoma Tripod Fractures Tripod fractures consist of fractures through: Zygomatic arch Zygomaticofrontal suture Inferior orbital rim and floor Zygoma Tripod Fractures Imaging Studies Radiographic imaging: Waters, Submental and Caldwell views Coronal CT of the facial bones: 3-D reconstruction Zygoma Tripod Fractures Clinical Features Clinical features: Periorbital edema and ecchymosis Hypoaesthesia of the infraorbital nerve Palpation may reveal step Concomitant globe injuries are common Medial wall blow-out fracture Signs Periorbital subcutaneous emphysema Ophthalmoplegia - adduction and abduction if medial rectus muscle is entrapped Treatment • Release of entrapped tissue • Repair of bony defect Anterior Segment Trauma Assessment History Forces involved Blunt, FB?, Penetrating Chemical Acid? Alkali? Contact allergy? Common Causes Abrasion Foreign body Grinding Penetrating Injury Minor trauma - lash, finger Recurrent Epithelial Erosion Syndrome Plant Hammering metal on metal Explosion Dirty / clean Blunt Fist Ball Bungy cord Examination Visual Acuity Skin/lids Evert lids Evidence of severity of injury ? Subtarsal FB Look for fine scratches on upper cornea Conjunctiva Laceration Look carefully for scleral injury beneath Sub conj hemorrhage Examination… Cornea Fluorescein stain - abrasion/wound Leak Infiltrate FB Anterior chamber Cells Hyphaema Hypopyon Examination…. Iris Lens Transillumination defects Peaked pupil Dilated pupil Check for RAPD Red reflex Stability IOP +/- angle Iris Trauma RAPD RAPD Relative afferent pupillary defect Corneal foreign body Grinding most common cause Usually do not need surgery Treatment Removal of foreign body with needle and/or burr Children may require GA Corneal Abrasion Common Usually resolve quickly Very painful initially Treatment Exclude other injuries Chloramphenicol ointment Patch 24 hours +/- pain relief / sleeping tablets w+XDwvc Recurrent Epithelial Erosion History gives clue Often triggered by minor trauma Treatment Lubricants Bandage contact lens Epithelial debridement Tetracyclines Laser Phototherapeutic Keratectomy (PTK) Anterior Stromal Puncture Hyphaema Hyphaema Blunt injury Complications: Raised IOP Angle recession Corneal staining Rebleed Treatment Steroid Bed rest - debatable Frequent monitoring wrt IOP Angle recession Traumatic Uveitis Ranges from Mild to Severe Usually other injuries as well Treat as for normal uveitis but may not require long taper Vossius ring Iris Dialysis Lens subluxation Cataract Thank you for listening!