Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
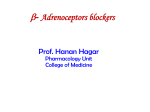
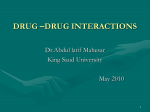
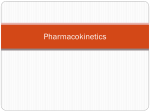
Effect of Propranolol on Elevated Arterial Blood Pressure By DAVI W. RICHARDSON, M.D., JACK FREUND, M.D., ARTHUR S. GEAR, M.D., H. PAGE MAUCK, JR., M.D., AND LESTER W. PRESTON, B.S. SUMMARY Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Nineteen patients with moderately severe arterial hypertension received propranolol (120 mg daily), or chlorthalidone (100 mg daily), both medications together, and placebos in a double-blind crossover trial. Each treatment was given for 5 weeks; blood pressure was measured at weekly intervals. Propranolol alone reduced arterial pressure by 9/8 mm Hg, a statistically insignificant change. Use of chlorthalidone alone was accompanied by an average reduction in arterial blood pressure of 23/9 mm Hg. Both drugs together lowered blood pressure by 33/15 mm Hg. Heart rate was lower in regimens including propranolol; body weight and serum potassium and chloride concentration were lower and blood urea nitrogen and serum creatinine were higher in regimens containing chlorthalidone. Propranolol, in the dose given, is a less effective hypotensive drug than is chlorthalidone. Additional Indexing Words: Chlorthalidone Hypertension Potassium supplementation Weight PRONETHALOL, an effective beta-adrenergic blocking agent, was observed to reduce arterial blood pressure in hypertensive patients being treated for angina pectoris.1 Subsequently Prichard and Gillam2 3 compared propranolol, another beta-adrenergic blocking drug, 120 to 640 mg/day, with previously administered methyldopa in 12 hypertensive patients and reported lower blood pressure during use of propranolol. Since in previous clinical trials2-6 the hypotensive effect of propranolol was not compared with that of placebo, we have evaluated the hypotensive efficacy of propranolol in comparison with Beta-adrenergic blockade Blood chemistry Heart rate tient knew which therapy was being administered. We have compared propranolol, 120 mg/day, placebo, chlorthalidone, 100 mg/ day, and the combination of propranolol and chlorthalidone as hypotensive agents in 19 hypertensive patients. The order of administration of drugs was randomized and unknown to patient or physician. Propranolol, 120 mg/ day, had only moderate hypotensive effect. Methods Twenty-two patients entered the study. One refused to return after the first week, one died 2 weeks before completion of the fourth period, and one was stopped before entering the fourth period which would have included chlorthalidone and potassium, a combination withdrawn by its manufacturer because of toxicity. Thus 19 patients, 5 male and 14 female, completed the entire study. The patients' ages ranged from 35 to 69 years. T.C., a 44-year-old Negro man, had chronic nephritis manifest by persistent proteinuria, microscopic hematuria, cylinduria, and azotemia without pyuria or bacteriuria. G.W., a 57-year-old Negro woman, had probable hyperparathyroidism, with intermittent hypercalcemia, a renal stone, and recurrent duodenal ulcer. She that of inert tablets and a standard diuretic in trials in which neither physician nor paFrom Departments of Medicine and Biometry, Medical College of Virginia, Richmond, Virginia. Work was supported by grants from the Virginia Heart Association and from Ayerst Laboratories and Geigy Pharmaceuticals. Presented at the Fortieth Scientific Sessions of the American Heart Association, San Francisco, California, October 21, 1967. 534 Circulation, Volume XXXVII, April 1968 PROPRANOLOL AND ELEVATED BLOOD PRESSURE Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 did not have azotemia or infected urine. In the remainder, no cause for hypertension could be demonstrated despite multiple urinalyses, determination of urinary catecholamine excretion, intravenous pyelography, radioactive renography, multiple determinations of serum sodium, potassium, chloride and bicarbonate concentrations, and complete historical and physical examination. None of the patients had hemorrhagic or exudative retinopathy, congestive heart failure, edema, asthma, or gout. Six had chemical diabetes mellitus; none received insulin. Each patient had been followed in the hypertension clinic for months, and each had previously received antihypertensive drugs. Each had diastolic blood pressure averaging 88 mm Hg or more during five weekly visits while receiving placebo tablets, save for one patient whose blood pressure averaged 143/80 mm Hg prior to randomization and 150/85 during the randomization placebo period. All patients carried on their usual work without restriction of diet or exercise. Each patient was seen at weekly intervals for 30 weeks. At each visit the patient was weighed and arterial pressure was recorded by one of two nurses who made all measurements through- 535 out the study. Patients lay for 10 minutes in a quiet room, after which blood pressure was measured three times in the supine position and three times in the standing position. Heart rate was recorded with the patients supine. Pills remaining in the bottles issued the previous week were counted in an attempt to ensure that medication was taken properly, and the patient was reminded how to take the medications. At 3week intervals, blood was drawn for hemoglobin concentration, white cell count, autoanalyzer estimation of urea nitrogen and of serum concentrations of creatinine, sodium, potassium, chloride, bicarbonate, bilirubin, alkaline phosphatase and glutamic-oxalacetic transaminase. At the first five weekly visits, each patient received sufficient medicaments for him to take one dummy capsule of chlorthalidone twice daily and one dummy tablet of propranolol three times daily in the ensuing week. Thereafter, each received treatment for 5 weeks with each of the four possible combinations: (1) both medications dummy; (2) both active (propranolol, 40 mg for use thrice daily, and chlorthalidone, 50 mg for use twice daily); (3) active chlorthalidone, 50 mg for use twice a day and dummy pro- Table 1 Pressures Arterial in Position Between the Initial Placebo Period (Single-Blind) and Comparison of Lying the Treatment Placebo Period* (Randomized; Double-Blind) Patient D.C. J.H. L.G. M.T. G.W. P.A. T.C. S.M. P.T. E.P. C.H. C.B. L.S. P.H. A.R. M.C. L.W. E.A. C.A. Age (yr) Sex Race F 40 M 49 F 40 F 35 F 49 M 55 Average for period 45 M F 52 F 43 F 50 Average for period F 44 F 67 M 54 F 69 F 37 F 55 Average for period F 49 F 45 M 46 Average for period Overall averages *Period = 5 weeks. Circulation, Volume XXXVII, April 1968 N N Treatment placebo period N N N N First First First First First First N N N N Second Second Second Second N N N Third Third Third Third Third Third N N N Fourth Fourth Fourth N N w Systolic (mm Hg) Initial Treatment Diastolic (mm Hg) Initial Treatment 88.8 142.8 229.5 159.4 154.9 210.7 169.6 148.8 216.0 164.1 153.5 99.7 220.8 182.3 120.3 107.3 101.2 126.2 114.0 (177.8) (180.9) (105.5) (110.0) 206.0 168.0 164.3 144.0 191.1 167.2 161.2 148.2 121.9 102.4 115.0 98.9 97.5 104.3 (170.6) (166.9) (104.3) (103.9) 133.0 131.9 150.4 188.0 193.8 160.8 88.1 80.4 112.6 113.7 113.7 110.0 87.8 84.2 121.3 114.0 112.3 108.3 (162.8) (103.1) (104.7) 199.2 137.7 198.1 94.8 94.3 136.9 96.0 99.2 129.0 (178.3) (172.3) (108.7) (105.0) (108.1) (106.7) 143.0 187.6 196.5 152.7 165.0 (163.0) 184.3 131.1 215.9 (177.1) (171.5) 152.2 119.9 97.2 96.5 96.3 93.0 125.7 99.9 RICHARDSON ET AL. 536 Table 2 Arterial Blood Pressure-Lying Position Treatment First week Second week Third week Fourth week Fifth week Systolic pressure 170.08 172.57 172.95 172.00 162.35 162.08 165.84 162.82 146.42 147.10 141.05 144.37 148.56 142.05 143.05 139.80 138.46 138.73 Diastolic pressure 105.18 106.68 108.37 Dummy* 164.82 Propranololt Chlorthalidonet Propranolol plus 153.83 chlorthalidone§ Dummy Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Propranolol Chlorthalidone Propranolol plus chlorthalidone 99.17 97.20 95.45 98.18 92.78 97.05 94.37 96.91 106.70 98.67 97.74 92.28 94.18 91.02 90.63 92.11 103.40 Means not connected by vertical lines are significantly different (P < 0.05). *1 inert tablet resembling propranolol three times daily plus 1 inert tablet resembling chlorthalidone twice daily. tPropranolol, 40 mg, three times daily plus 1 dummy chlorthalidone tablet twice daily. *Chlorthalidone, 50 mg, and KC1, 0.5 g, twice daily plus 1 dummy propranolol tablet three times daily. §Propranolol, 40 mg, three times daily plus chlorthalidone, 50 mg, twice daily. Table 3 Average Arterial Blood Pressure-Standing Position Treatment First week Second week Third week Systolic pressure 165.40 170.50 Dummy* 162.25 Propranololt 153.77 161.55 Chlorthalidonet 142.47 Propranolol plus chlorthalidone§ 136.31 Dummy 113.87 Propranolol Fourth week Fifth week 168.25 170.56 160.75 159.30 158.14 143.22 137.05 138.72 142.63 140.13 135.43 133.37 132.95 114.05 117.25 117.42 116.49 107.95 109.72 106.37 107.72 108.28 Chlorthalidone 105.07 105.37 103.40 104.19 103.93 Propranolol plus 101.70 102.46 99.62 98.65 98.32 Diastolic pressure chlorthalidone Means not connected by vertical lines are significantly different (P < 0.05). *1 inert tablet resembling propranolol three times daily plus 1 inert tablet resembling chlorthalidone twice daily. tPropranolol, 40 mg, three times daily plus 1 dummy chlorthalidone tablet twice daily. *Chlorthalidone, 50 mg, and KC1, 0.5 g, twice daily plus 1 dummy propranolol tablet three times daily. §Propranolol, 40 mg, three times daily plus chlorthalidone, 50 mg, twice daily. Circulation, Volume XXXVII, April 1968 PROPRANOLOL AND ELEVATED BLOOD PRESSURE Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 pranolol; and (4) dummy chlorthalidone and active propranolol, 40 mg for use thrice daily. The order of administration was randomized and unknown to patient and observers. During the period when chlorthalidone was given without propranolol, potassium chloride, 500 mg, was added to each chlorthalidone capsule in order to observe the effect of potassium supplementation on serum potassium concentration. Blood pressure during that period in the double-blind crossover in which the patient received both dummies was used as the control pressure, against which drug effects were compared. Analysis of variance for a randomized block design7 (that is, each patient was considered as a complete block) was performed separately for each treatment period and each variable. Subsequently, Duncan's multiple-range test8 was used to determine the statistical significance of the observed response differences among all treatment Results LYING 170r x ---- 160 H 150 H 140 H Circulation, Volume XXXVII, April 1968 - *'----. x ~x dv0 oe Ke A -o_ __ __ 0 LALJ 30 *-* (1) Effects on Arterial Pressure The effect on blood pressure of the patients' habituation to the examination was observed by comparing the average pressure during the initial 5-week pre-randomization period of placebo administration with the average pressure during the "treatment" 5-week period in the double-blind trial in which the patient received placebos. Table 1 shows the data for each patient. In none of the four placebo periods during the double-blind comparison was the group average pressure significantly different from the average pressure during the pre-randomization period. It is thus reasonable to assume that the changes in blood pressure observed during administration of active drugs are the result of the _ drugs, rather than lapse of time or habituation to the experimental procedure. The blood pressure associated with each regimen is summarized in tables 2 and 3 and figure 1. Propranolol, 40 mg three times a day, reduced blood pressures with the patient in the lying down position by 9 and 8 mm Hg, systolic and diastolic, as compared with placebo. Statistically significant reduction in diastolic pressure attributable to propranolol occurred only in 2 of the 5 weeks. There was no evidence of greater hypotensive effect in the fifth than in the first week of propranolol administration. Chlorthalidone alone, 50 mg twice a day, reduced pressure an average pairs. All patients were interviewed at each visit, after blood pressure and pulse had been recorded. No special effort was made to have a particular physician interview a particular patient throughout the study; in fact, each patient was seen by all four physicians at some time. Physicians were instructed to ask at each visit about anv discomfort or change in daily habit; about sleepiness, diarrhea, shortness of breath, swelling, and dizziness; and to record all symptoms. At the end of the study, all recorded symptoms were tabulated by study period without knowledge of which drug was received in any period. They were then retabulated by drug regimen. 537 120 Dummy x--x Propronolol A-A Chlorthalidone o--o P a C H 0~: KR I I1O 100 X. - * _ __o_ - X. 90 IE 3 2 WEEKS OF TREATMENT 1 4 5 Figure 1 Arterial pressure, recorded in the supine position, on each regimen. Each point is the average for 19 patients. The four regimens were placebo, propranolol, 120 mg daily, chlorthalidone, 100 mg daily, and propranolol plus chlorthalidone (P&C). RICHARDSON ET AL. 538 20 0 10 + * - Lying o - Standing ° 0 o 0 0 0 - 0 * 0 a I 0 i44 -10 0 0 0 88 0 0 0 . -20 _ Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 & 0 * 0 0 0 80 0 8 (5). -30 _ (I) I 0 0 0 0 a 0 0 0 m0 0 m0 -40 _ Zrz. 0 0 0 0 8 0 0 S -50 _- 0 0 0 0 0 -60 _- 0 . -70 _ Propronolol 40mg/ tid Chlortholidone 50mg / bid Propronolol Chlortholidone Figure 2 The changes in systolic arterial pressure observed in individual patients during active drug regimens. The horizontal line at zero represents each patient's pressure during the second through fifth weeks of placebo medication in the double-blind trial. Each point represents the change in blood pressure observed in one patient during the second through the fifth week on the indicated regimen, and is the mean of 12 measurements, three each week. Closed circles show changes in supine and open circles changes in standing blood pressure. of 23/9 mm Hg as compared with the placebo. Propranolol and chlorthalidone together reduced pressure an average of 33/15 mm Hg below that observed during administration of the placebo. Blood pressure was not significantly lower during administration of pro- pranolol and chlorthalidone together than with chlorthalidone alone. The effects of drug regimens on blood pressure in the standing position were similar to those observed in the supine position (tables 2 and 3). Figures 2 and 3 show the changes of systolic and diastolic Circulation, Volume XXXVII, April 1968 PROPRANOLOL AND ELEVATED BLOOD PRESSURE ffi +10 ~r- 0 0 0 0 0 0 LAJ1~ 539 0 IH 0 0 . 0 8 0 o 1 -10 IF oo _00*0~~0 S °° 8 fB 0 ~ 8 A . 9 v 0 -20 I I 0 80 0 * v 0% 0 0 Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 0 -30 -4j * - Lying o - Standing (-40 8 0 Propronolol 40mg/tid Chlorthalidone 50mg /bid Propronolol Chlortholidone Figure 3 Changes in diastolic arterial pressure observed regimens. See legend for figure 2. in individual patients during active drug Table 4 Heart Rate in Treatment Period First week HR Drug C D 79.2 76.8 C + P 71.3 P 65.0 Second week HR Drug Third week Fourth week Drug HR Fifth week HR Drug C 83.9 (Incomplete C 84.1 C 77.8 D 75.1 data not D 76.4 D 77.4 C+P 68.6 analyzed) C + P 66.2 C+P 68.2 P 67.6 P 65.8 P 64.1 Means not connected by the same vertical line are significantly different (P < 0.05)Duncan's multiple range test. Abbreviations: HR = heart rate; D = dummy; P = propranolol; C = chlorthalidone; and C + P = chlorthalidone plus propranolol. individual patients associated with each active drug regimen. pressure in Heart Rate, Weight, and Blood Chemistry The heart rate was consistently lower in the two regimens which included propranolol Circulation, Volume XXXVII, April 1968 (table 4). Sinus rhythm was present in all subjects throughout the study. In each week of the treatment period, there was a significant (P <0.05) difference among the body weights (table 5). For all treatment weeks the weights during the two chlorthali- RICHARDSON ET AL. 540 Table 5 Weight (lb) in Treatment Period First week Drug Weight Second week Drug Weight Fort wee Fourth week Drug Weight Third week Drug Weight Fitwe Fifth week Drug Weight P 167.4 P 167.8 P 166.6 P 166.8 P 166.6 D 165.7 D 165.4 D 166.0 D 165.4 D 165.8 C 163.0 C+P 163.8 C 162.8 C + P 162.8 C+P 163.7 C + P 163.2 162.4 C C C+P 164.9 162.3 C 163.2 Means not connected by the same vertical line are significantly different (P < 0.05) Duncan's multiple range test. Abbreviations: D = dummy; P - propranolol: C -- chlorthalidone; and C + P - chlorthalidone plus propranolol. Table 6 Clinical Laboratory Data: Fifth Week of Each Treatment Period Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Chloride Chloride (mEq/L) Blood urea nitrogen Blood urea nitrogen (mg/100 ml) 25.2 C+P C P D 24.0 20.0 18.4 P D C C+P C+P 1.56 C P 1.52 1.38 1.35 C+P C D P Sodium (mEq / L) D p C C+P C+P (mg/100 ml) 103.3 103.2 99.8 99.5 C+P P C 0.107 0.094 0.060 D 0.058 26.4 26.3 25.5 25.4 Bilirubin, total (mg! 100 ml) C+P P C 143.8 143.0 142.8 142.0 C+P C D P 21.3 20.6 19.0 18.4 Alkaline phosphatase (Bessey-Lowry units) 4.31 4.28 3.90 3.891 P C C+ P D 1.69 1.47 1.42 1.29 0.334 0.321 0.310 0.270 D White cell count (cell / mm3) SGOT (Karmen units) Potassium (mEq / L) p D C Bilirubin, direct Carbon dioxide (mM/L) Creatinine (mg/100 ml) D Biliruhin, direct P D C C+P 6952i 6511 6327 6280 Hemoglobin (gl 100 ml) C D C+P P 13.62 13.39 13.34 12.98 Means not connected by the same vertical line are significantly differenct (P < 0.05)Duncan's multiple range test. Abbreviations: D - dummy; P - propranolol; C - chlorthalidone; and C + P - chlorthalidone plus propranolol. done regimens were slightly less, but the statistical significance of these differences was more definitive in the earlier weeks. Blood chemical and hematological analyses are shown in table 6. During the administration of the two chlorthalidone regimens, concentration of blood urea nitrogen and serum creatinine were higher; those for se- rum potassium and chloride were lower. There was no difference between the serum potassium levels for the chlorthalidone regimen and for the combined chlorthalidone and propranolol regimen; in the former regimen, 0.5 g of potassium chloride was incorporated into each capsule of chlorthalidone. No significant differences among the four Circulation, Volume XXXVII, April 19(38 PROPRANOLOL AND ELEVATED BLOOD PRESSURE 541 Table 7 Possible Side Effects Placebo Pt. t No. * Symptom Headache Dizziness Dyspnea Cough and wheezing Fatigue Sleepiness Nausea Propranolol Pt. No. 6 6 11 4 1 6 3 1 5 2 1 1 3 0 4 3 3 0 1 4 0 3 2 3 2 2 2 0 Chlorthalidone and KC1 Pt. No. Propranolol and chlorthalidone Pt. No. 2 9 2 2 6 1 2 7 9 1 1 3 5 3 6 3 2 5 7 5 6 7 3 4 5 3 1 1 *No. = Number of times symptom was recorded. tPt. - Number of patients who developed this symptom. Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 regimens were noted with respect to blood hemoglobin, white cell count, serum carbon dioxide content, bilirubin concentration, nor serum glutamic-oxalacetic transaminase and alkaline phosphatase. Side Effects Table 7 presents the number of times a symptom occurred during each regimen, and the number of patients who experienced each symptom. Headache occurred most frequently during placebo administration and least frequently in regimens containing chlorthalidone. Dizziness, on the other hand, occurred least frequently during the placebo period, and most frequently during administration of chlorthalidone. Dyspnea, cough, and wheezing occurred more frequently in regimens containing propranolol, with or without chlorthalidone. Fatigue occurred more often with regimens containing chlorthalidone or propranolol than with placebo. Other recorded symptoms, mentioned by only one or two patients each, included nocturia, present in all four regimens; angina pectoris, also present in all four regimens; urinary urgency, diarrhea, indigestion, nocturnal leg cramps, and stuffy nose. Discussion Propranolol in a dose of 40 mg three times daily caused an average blood pressure reduction of 9 mm Hg systohic and 8 mm Hg diastolic. These changes are statistically insignificant. The modest effect of propranolol is similar to that found by Waal,4 who obCirculation, Volume XXXVII, April 1968 served an average decrease in blood pressure of 12/6 mm Hg when propranolol, 45 to 150 mg/day, was added to other antihypertensive medication in 89 hypertensive patients. Similarly, Richards5 found an average decrease in pressure of 11/12 mm Hg in nine patients with elevated arterial pressure during administration of propranolol, 150 to 300 mg/day for 8 to 15 weeks. Paterson and Dollery6 compared the effects of propranolol, 80 mg/ day, propranolol, 240 mg/day, and hydrochlorthiazide, 50 mg/day, on 11 hypertensive patients who received each regimen for 6 weeks. Arterial pressure (lying) was 13/5 mm Hg higher with propranolol, 240 mg/day, and 14/6 mm Hg higher with propranolol, 80 mg/ day, than with hydrochlorthiazide. Though Prichard and Gillam3 have suggested that prolonged administration (4 weeks or more) of propranolol produces greater reduction of arterial pressure than is seen in the first 3 weeks, our results with those of Waal4 and of Paterson and Dollery6 show no greater hypotensive effect after 5 or 6 weeks of propranolol than after 1 to 3 weeks. Addition of potassium chloride, 0.5 g twice a day, to chlorthalidone had no noticeable effect on serum potassium concentration. Thus, there seems little reason for administration of capsules combining potassium, at least in this dose, with chlorthalidone. Analysis of side effects suggests that reduction in blood pressure lessened the prevalence of headache in this group of patients 542 Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 with mild to moderate hypertensive disease. The greater frequency with which dyspnea and wheezing occurred while patients were taking propranolol is in keeping with known effects of the drug, which blocks adrenergic bronchodilation and, by reducing adrenergic stimulation of the heart, favors cardiac decompensation. In no patient were symptoms severe enough to require alteration of medication. One patient died in the fourth week period of the study, while taking propranolol alone. She was a 52-year-old Negress with recurrent ventral hernia which had previously been repaired surgically without prolonged success. The hernia protruded one day, producing pain and vomiting for 2 hours, and then reduced itself spontaneously. She stopped taking propranolol that day. Two days later the hernia protruded again, and she entered the hospital with abdominal pain, vomiting, and hypotension. The hernia could not be reduced. Shock and puhnonary edema followed, and the patient died 36 hours later with continued pulmonary edema. Permission RICHARDSON ET AL. for autopsy was not given. The contribution of propranolol to her death is uncertain. Infusion of isoproterenol resulted in tachycardia and reduction in arterial pressure, suggesting that beta-adrenergic blockade was not present. References 1. PRIcEun, B. N. C.: Hypotensive action of pronethalol. Brit Med J 1: 1227, 1964. 2. PmcHARw, B. N. C., AND GILLAM, P. M. S.: Use of propranolol in the treatment of hypertension. Brit Med J 2: 725, 1964. 3. PiCuHARD, B. N. C., AND GILLAM, P. M. S.: Propranolol in hypertension. Amer J Cardiol 18: 387, 1966. 4. WAAL, H. J.: Hypotensive action of propranolol. Clin Pharmacol Ther 7: 588, 1966. 5. RcHADs, F. A.: Propranolol in hypertension. Amer J Cardiol 18: 384, 1966. 6. PATERSON, J. W., AND DOLLERY, C. T.: Effect of propranolol in mild hypertension. Lancet 2: 1148, 1966. 7. BAILEY, N. T. J.: Statistical Methods in Biology. London, English Universities Press, 1959, p. 108. 8. STEEL, R. G. D., AND ToRRIE, J. H.: Principles and Procedures of Statistics. New York, McGraw-Hill Book Co., 1960, p. 107. Circulation, Volume XXXVII, Aprl 1968 Effect of Propranolol on Elevated Arterial Blood Pressure DAVID W. RICHARDSON, JACK FREUND, ARTHUR S. GEAR, H. PAGE MAUCK, JR. and LESTER W. PRESTON Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Circulation. 1968;37:534-542 doi: 10.1161/01.CIR.37.4.534 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1968 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/37/4/534 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/