Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
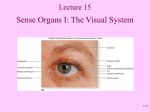
Ophthalmic Surgery Surgery of the Eyes Anatomy of the Eye Bony Orbit – two orbital cavities 7 bones form the orbit Maxilla Palatine Frontal Sphenoid Zygomatic Ethmoid Lacrimal Anatomy of the Eye Bony Orbit Above – ant cranial fossa, frontal sinus Medial – nasal cavity Below – maxillary sinus Laterally - middle cranial and temporal fossae Periosteum of bony orbit is continuous with dura mater Anatomy of the Eye Contents of the Bony Orbit Eyeball Muscles Nerves Vessels Other nerves and vessels of facial area around socket Lacrimal apparatus Lacrimal gland- lateral Produces tears and secretes them through a series of ducts into the conjunctival sac Puncta - medial- opening Lacrimal apparatus Lacrimal canaliculi Passage between conjunctiva and the Lacrimal sac Nasolacrimal duct Directs to the inferior meatus of the nose Conjunctiva Thin transparent mucous membrane, divided into two parts Palpebral – lines back of eyelids, contains the puncta Bulbar - lines front of globe, allows sclera to show through Conjunctiva Continuous at limbus with anterior epithelium of cornea Conjunctival sac, with an opening in front of eye between margins of eyelids called the Palpebral fissure Eyelids Musculofibrinous folds Protect globe and eye from light Upper larger and more mobile Canthi – medial and lateral angles on edge of eye Eyelids Obicularis oculi muscle Circular muscle acts as a sphincter Closes eye Eyelids Levator muscle Opens upper lid Innervated by the third cranial nerve and relaxing of orbicular muscle Eyelids Layers of eyelid Skin Subcutaneous with lymphatics Muscles Tarsal cartilage – dense fibrous tissue, forms the framework of the lids Anchored by medial and lateral palpebral ligaments Eyelids Layers of eyelid Cilia / eyelashes Meibomian glands – post to lashes Secretes a sebaceous substance that keeps the lids from adhering to each other Punctum lacrimale – near med edges of each eyelid Muscles of the Eye Extrinsic – inserted into sclera by tendons that arise from back of orbit (except the Inferior oblique) Work in pairs – antagonistic Muscles of the Eye 4 rectus – insert on side - superior, inferior, medial, lateral 2 oblique – insert on back – superior and inferior Muscles of the Eye Muscles are supplied by the Cranial Nerves 3rd – oculomotor- all ocular muscles except lateral rectus and superior oblique 4th – trochlear- superior oblique 6th – abducens- lateral rectus muscle Eye Muscle Simulator http://rad.usuhs.mil/rad/eye_simulator/e yesim.htm Includes a simulator on how eye muscles work and how the cranial nerves effect them Globe Eyeball or Oculus O.D. - Oculus Dexter – right eye O.S. – Oculus Sinister – left eye Supported on a cushion of fat and fascia Layers or Tunics Corneoscleral Cornea Sclera Choroid Retina External - Corneoscleral Sclera - joins cornea at limbus transitional zone Opaque layer – white Collatgenous fibers connected with fascia Receives tendons Pierced by ciliary arteries and nerves and posteriorly by the optic nerve Cornea Clear, transparent anterior portion of the eye Curvature enables it to function as an important refractive medium Continuous with the sclera Cornea 5 layers Bowman's membrane Connective tissue fibers Forms a barrier to trauma / infection If damaged it does not regenerate and a permanent scar is left Cornea 5 layers Stroma 90% of corneal thickness Multiple lamellar fibers Cornea 5 layers Descemet’s membrane Thin membrane between endothelium and substantia propria (stroma) Can become inflamed and herniate Cornea 5 layers Endothelium Single layer of cells that do not regenerate Responsible for the proper state of dehydration that keeps the cornea clear Damage causes corneal edema and loss of transparency Choroid Middle vascular pigmented layer Main source of nourishment of receptor cell and pigment epithelial layer of the retina Choroid Iris Regulates light entering eye, assists with clear images Pupil is central opening Retina Thin transparent membrane Nerve fibers from the retina converge to become the optic nerve (II) Retina, cont. Optic disk (blind spot)- point at which nerve enters the eyeball Optic nerve travels to contralateral side of brain Retina, cont. Sensory Retina Pigment epithelium – single layer – for O2 and nutrients Photoreceptor cells Macula Lutea – yellow spot, center of retina, 2mm from optic disk Fovea centralis – pit of closely packed cones in center of the macula – highest resolution and central vision. Retina, cont. Sensory Retina Rods and cones Cones- stimulated by light of different colors (color-vision) Rods- responds to dim light (nightvision) Respond to light energy and initiate the neural response, which goes to occipital cortex for interpretation Humors Fluid – gives shape Aqueous- anterior cavity – fills anterior and posterior chambers Transparent fluid, produced by the cilliary body Passes from the posterior to the anterior chamber, then to the venous system through the canal of Schlemm Humors Fluid – gives shape Vitrous (vitreous body) – fills posterior cavity (posterior to lens) Glasslike, transparent, gelatinous mass 99% water, 1% collagen and hyalurinic acid fills 4/5ths of the eyeball Choroid Ciliary body (intrinsic muscle) Extension of choroidal blood vessels, muscle mass and extension of neuroepithelium of retina Effects accommodation Secrets aqueous humor Choroid Iris (intrinsic muscle) Thin membrane, is the anterior portion of the middle layer, and is situated in front of the lens Peripheral border attached to the ciliary body Divides space between cornea and lens Choroid Iris Anterior chamber Posterior chamber Both filled with aqueous humor Refraction of the Eye Refractive media – bends light so rays strike Macular area Myopia- nearsightedness- light rays focus in front of the retina Hyperopia- farsightedness- light rays focus behind the retina Cornea - greatest refractive power – variations change it’s power Refraction of the Eye Lens – suspended behind the pupillary opening of the iris by the suspensory ligament and zonular fibers which expand and contract lens (accommodation/focus) Does not shed cells, cells become compressed and hard. Presbyopia- accommodation is lost with age as lens loses elasticity – onset usually occurs between age 40 to 45 Blood Supply Ophthalmic artery – for orbit and globe, from internal carotid Divided into globe, muscle and eyelid branches Central retinal artery/vein through optic nerve and serve inner retina Pathology Leading causes of visual impairment and blindness 1st - Macular degeneration 2nd - Cataracts 3rd - Glaucoma Pathology Macular degeneration (1st) Leading cause of vision impairment in persons over 50 Degeneration in the macular area of the retina of the eye This condition will not, in itself, lead to total blindness Pathology Macular degeneration (1st) Can lead to loss of central vision, making it difficult to read or do fine work Have patient look at a grid with each eye separately. If central vision is impaired the lines will appear wavy instead of straight Pathology Cataracts (2nd) Opacification of the lens From Greek word, means mist of a waterfall Common form results from aging, but may be congenital or caused by infection, injury, radiation exposure, complication of diabetes, and smoking Pathology Cataracts Awareness and treatment goes back over 3,000 years “Couching or reclination” tx practiced sporadically from 2,000-1,000 BC until 1745 1745 Jacques Daviel, a French surgeon, performed the first deliberate lens extraction on a monk from a local monastery 18th century attempts to implant lenses were unsuccessful Pathology Cataracts Modern implants evolved from the observation in WWII that noted a lack of reactivity to plastic fragments from shattered plane canopies that penetrated the eyes of fighter pilots Pathology Glaucoma (3rd) Increased intraocular pressure Results in atrophy of the optic nerve Occurs when the aqueous humor drains from the eye to slowly to keep up with production Pathology Retinal disorders Damage to the sensory receiver of light perception Detached retina (pictured) Macular degeneration Diabetic retinopathy Pathology Corneal transplant First performed around 1817 Failed, as they used animal tissue (xenograft) instead of human tissue (allograft) First to remain clear in 1905 1950 Ramone Castroviejo developed the procedure, and promoted the donation of eyes after death that resulted in the formation of eye banks throughout the world Pathology Ametropia Imperfect refractive powers of the eye in which the principal focus does not lie on the retina, as in myopia, hyperopia, and astigmatism Pathology Astigmatism A form of ametropia in which the refraction of a ray of light is spread over a diffuse area, rather than sharply focused on the retina, due to differences in the curvature in various areas of the cornea and lens Pathology Aphakia - absence of the crystalline lens of the eye Aphakia with Soemmering's ring formation. Patient Concerns Preoperatively Orient patient to environment (for visual and/or hearing impairment) Approach patient from non-affected side If walking a patient into OR, offer your arm to lead them instead of pulling them Let them know desired results of eye drops and sedation Explain what to expect from anesthetic Explain routine of intraoperative period Patient Concerns Preoperatively Explain what to expect immediately after surgery They may be restless, have discomfort and anxiety There may be limitations in mobility and prosthesis (positioning) Ask about medical problems, general and ophthalmic (i.e. Diabetes, glaucoma, etc.) Ask about medications and allergies Patient Concerns Postoperatively Give verbal and written instructions regarding Use of eye drops, other meds Information on limitations on activities (Awareness that vision with only one eye interferes with depth perception, i.e. Going down steps, driving, etc.) Patient Concerns Postoperatively Give verbal and written instructions regarding Wound care Signs and symptom of complications Who to call with questions or concerns Clinical appointment times or phone number to schedule Anesthesia Understand that most surgery is under local anesthesia Should be quiet and peaceful Most patients are sedated There may be an O2 tube under drapes Anesthesia Topical For cataract-extraction May be supplemented with infiltration anesthesia in anterior chamber Infiltration Injected beneath skin, subconjunctival or into the Tenon capsule (thin connective tissue envelope behind the conjunctiva Anesthesia Peribulbar (preferred) Around soft tissue of globe with needle to floor and roof of orbit Retrobulbar Injection into base of eyelids at the orbital margins or behind the eyeball to block ciliary ganglion Injected 10-15 minutes prior to surgery to paralyze extraocular muscles Positioning Supine Stabilize head with 1” paper tape or other head holding device Protect bony prominences, provide alignment to body Prepping If eyelashes are clipped, do before prepping Spread water soluble lubricant on scissors to catch hairs May order 5% povodine-iodine on conjunctiva 1 –2 drops on surface before prep - then rinse with NS Prepping Cleanse eyelids of operative eye, lid margins, lashes, eyebrows and surrounding skin Lid margins cleaned by everting the lids and cleaning with cotton-tipped applicator moistened with disinfectant. Don’t allow entry into eye or ear. Irrigate with NS in irrigation bulb, should flow medially to laterally Draping Eliminate lint and fiber particles Water repellent Adequate air exchange Place Mayo stand above the patient’s chest or face shield, drape over Draping Use one-piece fenestrated drape Plastic, sticky around hole ALT: head drape with fenestrated plastic eye sheet A fluid drainage bag with wicking strip may be adhered to eye sheet Surgical Needs Be sure implants or prostheses are present Microscope drape or sterile handles Field with lint-free barriers Gloves lubricant free or wiped Powder irritates the cornea Surgical Needs Instrument part used in wound not touched with gloves Debris cleaned with cellulose sponge Meds instilled into eyes Hold light pressure over lacrimal duct for 1 minute to prevent system absorption and drying inner canthus after each drop Surgical Needs Let patient know what to expect from meds. Protect cornea after anesthetic instilled to prevent damage Need to irrigate eye regularly to prevent corneal drying. Know that pressure on eye/tension or traction on ocular muscles can produce bradycardia. Instruments Microscopic, nonreflective finish Storage cases protect tips and cutting surfaces Inspect under magnifiers each time for burrs, nicks, alignment Clean with non fibrous sponge Instruments Know name and purpose of instruments Place on Mayo in order of use Clean in ultrasonic with each not touching another Rinse and dry with blower, not cloth Instruments No instrument milk on irrigating cannulas to prevent damage to eye Do routine maintenance to sharpen, realign, and adjust Tonometer- instrument used for measuring IOP Instruments Fixation forceps – hold tissue or provide traction before incision Angled tooth that overlaps for secure fixation Suturing forceps single toothed at right angle Tying forceps with flat platform to hold suture Suture 4-0 to 10-0 Handle as little as possible – prevent weakening and fraying Gut and collagen should be rinsed before use Needles are delicate, check for burrs and handle carefully Drugs Alex- 669, 670 & 671 “Medications Used During Opthalmic Surgery” Table 18-1 Dressings Prevent palpebral movements Protect wound from contaminants Absorb blood and tears Area cleansed with saline sponges Antibiotic ointment may be spread over plastic repairs, lids and lashes to prevent sticking to dressing Dressings Dressing Sterile eye pad with tape After intraocular – perforated aluminum plate / shield prevents external pressure on eyes Pressure dressing – pad with roller gauze around head prevents eye globe movement Cataract – may use collage corneal shields – rehydrated with anti-infective- antiinflammatory solution for dressing May have no dressing Surgical Interventions Removal of Chalazion Incision and curettage of a chronic granulomatous tumor or cyst of one or more of the meibomian glands in the tarsal plate of the eyelid Performed under local anesthesia Surgical Interventions Repair of Entropion Perform a blepharoplasty to correct Entropion- turning inward of the lower lid margin In-turned lashes and skin rub and irritate the cornea Seldom occurs in people under age 40 Performed under local anesthesia Surgical Interventions Repair of Ectropion Lateral canthal sling repositions and tightens the lower lid in a horizontal direction Ectropion- sagging and eversion of the lower lid Usually bilateral, and usually in older persons Symptoms include tearing, conjunctival infection and irritation, and inadequate corneal protection leading to corneal injury Surgical Interventions Surgery for Ptosis Correction of drooping of the upper lid, commonly by a levator apponeurosis repair Incision is made in the upper lid apponeurosis is dissected, divided, and reattached proximally with interrupted 6-0 n.a. Performed under local anesthetic- awake patient is asked to look forward so the sutures may be adjusted Surgical Interventions Dacryocystorhinostomy Establishment of a new tear passageway for drainage into the nasal cavity Performed for chronic dacryocystitis (infection of the lacrimal sac) causing resistant obstruction of the nasolacrimal duct Performed under general anesthesia Surgical Interventions Evisceration Removal of the contents of the eye, leaving intact the sclera and the attached muscles Implant may be placed within the empty shell Surgical Interventions Enucleation Removal of the entire eyeball, usually with insertion of a round implant into the socket to replace the globe May use donor sclera to reattach the muscles to the globe for movement Surgical Interventions Exenteration Removal of the entire orbital contents, including the periosteum Performed for certain malignancies of the globe or orbit Procedure may or may not include removal of the eyelids Surgical Interventions Stabismus Inability to direct the two eyes on the same object because of lack of coordination of the extraocular muscles Surgical Interventions Stabismus Deviation commonly corrected by: Resection- removal of a portion of the muscle and attachment of the cut ends- strengthens the muscle Surgical Interventions Stabismus Deviation commonly corrected by: Recession- severs the muscle from its original insertion with reattachment more posteriorly on the sclera- weakens the muscle Surgical Interventions Pterygium excision Excision of a fleshy, triangular encroachment of conjunctiva onto the peripheral area of the cornea Tend to be recurrent, so surgery is delayed until vision is affected by encroachment on the visual axis Surgical Interventions Keratoplasty (aka- corneal transplant) Graft of tissue from one human eye to another Performed when the patients cornea is thickened and opacified by disease or degeneration, or if the transparency of the cornea is impaired as the result of scars, infections, or burns Trephine A cutting instrument used to make a circular cut of the cornea Pathology Keratoplasty (aka- corneal transplant) Surgical Interventions Radial Keratotomy Refractive procedure to correct myopia, hyperopia, astigmatism, and aphakia Series of precise, partial-thickness radial incisions in the cornea Results in a flattening of the cornea, which reduces the refractive error First performed in 1978 Surgical Interventions Radial Keratotomy Surgical Interventions LASIK Surgery Refractive procedure to correct myopia, hyperopia, astigmatism, and aphakia Laser-assisted in-situ keratomileusis Curvature of the cornea is modified using a excimer laser Surgical Interventions Cataract extraction Surgical Interventions Cataract extraction- removal of the opaque lens from the interior of the eye ICCE- intracapsular cataract extraction Removes the lens within its capsule Rarely performed today Requires breaking the zonules Cryoprobe “frozen” to the lens Surgical Interventions Cataract extraction ECCE- extracapsular cataract extraction Anterior capsule is ruptured and removed, and the lens is expressed from the eye, generally using phaecoemulsification (ultrasonic energy with irrigation and aspiration, aka cavitron unit) Surgical Interventions Cataract extraction IOL- intraocular lens Optics- clear round portion Haptics- springs on either side- hold lens in position Surgical Interventions Iridectomy Removal of a section of iris tissue Performed to reestablish communication between the posterior and anterior chambers Performed to treat glaucoma Surgical Interventions Scleral buckling Performed to treat retinal detachment Causes an intrusion or push into the eye at the site Performed under general anesthesia May use cryosurgery (cold) or diathermy (use of high frequency current to generate heat for electrocoagulation) Surgical Interventions Vitrectomy Removal of all or a part of the vitreous body (gel) May also include coagulation of retinal vessels for bleeding, which causes the fluid to become opaque You made it through Eyes! Have a GREAT day!!!