Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
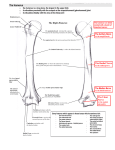
MEDIAN NERVE AND BRACHIAL ARTERY NEUROVASCULAR BUNDLE AT THE ELBOW – DANGEROUS ANTERIOR ANATOMY FOR THE ELBOW ARTHROSCOPIST A Gupta, S Kamineni, H K Ankem, A A Amis Department of Orthopaedics and Biomechanics, Imperial College, London, UK INTRODUCTION Arthroscopic capsulectomy is recognised to be a useful tool for the treatment of contracted elbows. The ultimate success of this technique will play will be determined, in most part, by how successful we are in avoiding nerve injuries. The reported prevalence of neurologic complications after elbow arthroscopy has ranged from 0 to 14 percent, and widely believed to be under-reported. The arthroscopic surgeon needs to be able to identify a safe zone within the elbow, free from neurovasculature, which is in close proximity to some parts the capsule being resected. The knowledge of where these str uctures are at risk of injury during such procedures will help to safeguard them. We performed an anatomical study on fresh human cadaveric elbows to define a zone of safety with regard to median nerve and brachial artery. METHODS Seventy fresh cadaveric elbows were studied for the anatomy of the median nerve and brachial artery, with respect to the bony anatomy that is readily visible during elbow arthroscopy. The bony landmarks utilised were the base width of the coronoid fossa, width between the medial and lateral trochlea ridges at the level of the medial epicondyle inferior margin, and the lateral rim width of the coronoid process. These measurements were performed at 90 degrees of elbow flexion, which is the standard arthroscopic position, and in pronation and supination. RESULTS The average width of the coronoid fossa base, trochlea and the lateral coronoid ridge were 14.3mm (range 13.9mm to 14.6mm), 22.5mm(range 21.6mm to 22.9mm), and 7.4mm (range 7.1mm to 7.6mm) respectively. The average diameter of the neurovascular bundle at the coronoid fossa base, trochlea and coronoid process was 8.6mm(range 8.2mm to 8.9mm), 8.4mm (range 7.9mm to 8.6mm), and 8.3mm(range 8.0mm to 8.5mm), respectively. The neurovascular bundle lies 1.6mm (range 1.4mm to 1.9mm) medial to the coronoid fossa base, 2.4mm (range 2.1mm to 2.9mm) lateral to the medial trochlea ridge and 2.2 mm (range 1.9mm to 2.5 mm) medial to the tip of the coronoid process. DISCUSSION The median nerve is a structure at risk when performing elbow arthroscopy of the anterior compartment. Our data supports the concept of a safe corridor of anterior elbow arthroscopic surgery. The corridor of safety encompasses a lateral margin for the radial nerve, the subject of an accompanying submission. The medial margin for this anterior corridor spans the midpoint of the coronoid fossa, the trochlea groove, and the apex of the coronoid process. This corridor is safe of neurovascular structures in all seventy cadaveric elbows and forms a useful zone for anterior elbow surgery. 5th Combined Meeting of the Orthopaedic Research Societies of Canada, USA, Japan and Europe Poster No: 178