Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
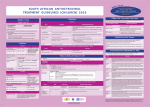
NORTHWEST AIDS EDUCATION AND TRAINING CENTER ART Initiation in Resource-Limited Settings Susan M. Graham Assistant Professor, Medicine and Global Health Adjunct Assistant Professor, Epidemiology Presentation prepared by: Susan M. Graham Last Updated: October 22, 2014 NORTHWEST AIDS EDUCATION AND TRAINING CENTER ART Initiation in Resource-Limited Settings Susan M. Graham, MD MPH PhD Dr. Graham is a member of the Kenya Research Group at the University of Washington. She began working with the University of Nairobi/UW Mombasa Field Site in 2003 as an Infectious Diseases Fellow, and developed the ART program offered at the UW research clinic here and another site north of Mombasa. Her research interests focus on access to and engagement in care for most at-risk populations in Kenya, including female sex workers and men who have sex with men. Dr. Graham holds a medical degree from McGill University, an MPH from Boston University, and a PhD in clinical epidemiology from the University of Toronto. Outline • ART Scale-up and Its Effects • HIV Care in RLS - Treatment eligibility Care cascade Diagnostic testing TB/HIV co-infection Initial treatment regimens • Prognosis following immigration to US ART Scale-up Continues UNAIDS Global Report 2013 Decreasing Mortality The number of AIDS deaths is declining with 1.6 (1.4–1.9) million in 2012, down from 2.3 (2.1–2.6) million in 2005 UNAIDS Global Report 2013 WHO Treatment Eligibility Target population 2006 2010 2013 HIV+ asymptomatic ARV-naive individuals CD4 ≤200 CD4 ≤350 CD4 count < 500, irrespective of WHO clinical stage HIV+ symptomatic ARV-naive individuals • WHO stage 2 or 3 and CD4 ≤200 • WHO stage 3 if CD4 200-350 or not available • WHO stage 4, irrespective of CD4 count • WHO clinical stage 2 if CD4 ≤350 • WHO clinical stage 3 or 4, irrespective of CD4 count WHO Stage 3 or 4, irrespective of CD4 count HIV+ pregnant women • WHO stage 1 or 2 and CD4 ≤200 • WHO stage 3 and CD4 ≤350 • WHO stage 4, irrespective of CD4 count • CD4 ≤350, irrespective of clinical symptoms • WHO clinical stage 3 or 4, irrespective of CD4 count Pregnant or breastfeeding women, irrespective of CD4 count or clinical stage HIV/TB co-infection ARV-naive individuals Active TB disease and CD4 ≤350 Active TB disease, irrespective of CD4 cell count Active TB disease, irrespective of CD4 cell count HIV/HBV co-infection ARV-naive individuals No specific recommendation Individuals who require treatment for their HBV infection, irrespective of CD4 cell count Individuals who require treatment for their HBV infection, irrespective of CD4 cell count HIV+ individuals with in serodiscordant relationships No specific recommendation No specific recommendation Provide ART to all partners infected with HIV regardless of CD4 cell count (to reduce the risk of HIV transmission to the negative partner) World Health Organization treatment guidelines Late Presentation • Median CD4 count at ART initiation, although increasing, has been far lower than 350 in almost all settings • Late presentation associated with high early mortality rates and poor retention in care • HIV stigma is a huge barrier in many areas, and may be worse for men in general • Additional stigma and criminalization are important barriers for many high-risk groups including - men who have sex with men - persons who use drugs - sex workers Koller JAIDS 2014, WHO ART Guidelines 2013 Care Cascade • Increasing knowledge of HIV status, linkage to care if positive, and optimal retention and adherence remain significant challenges • Currently, about half the people living with HIV globally do not know their HIV status. • In a systematic review of programs for HIV+ patients in subSaharan Africa, median estimates were: - 59% (35%–88%) staged clinically or receiving a CD4 count, - 46% (31%–95%) initially ineligible retained until eligibility, - 68% (14%–84%) eligible for treatment initiated ART Rosen PLoS Med 2011 Recommended Baseline Diagnostic Testing Purpose 2006 2010 2013 Monitoring treatment CD4 count CD4 count CD4 count Monitoring for toxicities Hemoglobin if AZT CBC with differential Hemoglobin if AZT Desirable/targeted: • Hemoglobin if AZT • ALT if NVP • Creatinine clearance and urine dipstick for glycosuria if TDF Desirable/targeted: • ALT if NVP • Creatinine clearance if TDF Choice of regimen Pregnancy test if EFZ Co-infections and comorbidities Screen for TB Screen for malaria WHO Treatment Guidelines Desirable: Pregnancy test Screen for TB Screen for TB Desirable: • HBV (HBsAg) serology Desirable: • Blood pressure measurement • HBV (HBsAg) serology • HCV serology • Cryptococcus antigen if CD4 count ≤100 • STD screening • “Assessment for major noncommunicable chronic diseases and comorbidities” (CVD, DM) TB/HIV co-infection • Since 2004, TB-related deaths among people living with HIV have declined by 36% worldwide • The decline is slightly less in Africa, home to 75% of all people living with TB and HIV • TB incidence highest in countries with highest HIV prevalence (Swaziland, Lesotho, South Africa) UNAIDS Global Report 2013, WHO Global Tuberculosis Report 2014 Initial Treatment Regimens Population 2006 2010 HIV+ ARV-naive adults and adolescents AZT or d4T + 3TC (or FTC) + EFV or NVP AZT or TDF + 3TC (or FTC) + EFV or NVP TDF possible as substitute for AZT, but not widely available Phase out d4T as feasible AZT + 3TC + NVP AZT or TDF + 3TC (or FTC) + EFV or NVP HIV+ pregnant women AZT preferred over TDF EFV included as option (but not during first trimester) HIV/TB coinfection HIV/HBV coinfection AZT or d4T + 3TC (or FTC) + EFV AZT or TDF + 3TC (or FTC) + EFV AZT + 3TC + ABC Initiated as soon as possible in all patients with active TB (within 8 wks after TB treatment) TDF + 3TC (or FTC) + EFV NNRTI regimens that contain both TDF + 3TC (or FTC) are required WHO Treatment Guidelines 2013 TDF + 3TC (or FTC) + EFV preferred Alternatives: AZT + 3TC + EFV AZT + 3TC + NVP TDF + 3TC (or FTC) + NVP Discontinue d4T Prognosis Following Immigration • In CA, foreign-born TB patients more likely than U.S.-born patients to have new HIV diagnoses - greater immunosuppression at TB diagnosis - ART or treatment for latent TB infection could have prevented TB • In Antiretroviral Therapy Cohort Collaboration, TB common - During first year of ART, HIV-positive migrants had higher rates of AIDSdefining events than nonmigrants • TB most common ADE among migrants • In NY State from 2001 to 2009 - New HIV diagnoses among FB increased from 17% to 28% of total - Compared with NFB, FB persons were significantly more likely to be diagnosed concurrently with AIDS and had lower median CD4 count - FB persons less likely to have insurance, and 13% needed language interpretation services Kong Public Health Rep 2014, ART-CC AIDS 2013, Wiewel STI 2013