Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
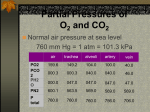
1. 2. 3. 4. 5. 6. Points to know and remember! Air moves from regions of high pressure to low pressure Ventilation is a mechanical process which is dependent on volume changes in the thoracic cavity If thoracic volume changes thoracic pressure changes If thoracic volume increases, gas pressure in the thorax decreases and… If thoracic volume decreases pressure increases All atmospheric pressures refer to pressures at the nose! Objective 5 Ventilation Ventilation (breathing) consists of: 1. Inspiration (inhalation): air moves from the atmosphere into the alveoli 2. Expiration (exhalation) air moves from the alveoli into the atmosphere Air Movement Between the Atmosphere and Terminal Bronchioles: 1. Air moves from areas of high pressure to areas of low pressure 2. As air flows, it encounters resistance Therefore, the flow of air through the passageways of the respiratory system can be described by the following equation: Air Flow = Pressure 1 - Pressure 2 ____________________________ Resistance Where pressure 1 is atmospheric pressure pressure 2 is alveolar pressure Inhalation Air moves from higher pressure atmosphere into lower pressure lungs Exhalation Air moves from higher pressure lungs into lower pressure atmosphere Atmospheric pressure > Alveolar pressure Atmospheric pressure < Alveolar pressure 760 mmHg – 759mmHg = a positive pressure, therefore air enters 760 mmHg – 761mmHg = a negative pressure, therefore air moves out Air movement between terminal bronchi and alveoli: powered by diffusion ….. Mechanism: three relevant pressures intra-alveolar pressure (intrapulmonary pressure) the pressure within the alveoli of the lungs; this pressure fluctuates between 759 and 761 mmHg Intrapleural pressure the pressure within the pleural cavity; this pressure is always less than the pressure in the lungs by about 4 mmHg atmospheric pressure the pressure exerted by gases in the atmosphere; at sea level, averages 760 mmHg Intrapulmonary (Intra-alveolar) pressure falls below atmospheric pressure during inhalation and rises above atmospheric pressure during exhalation: During Inspiration During Expiration Atmospheric pressure = 760 mmHg Intra-alveolar pressure = 759 mmHg Atmospheric pressure = 760 mmHg Intra-alveolar pressure = 761 mmHg P = 759 mmHg P = 761 mmHg How Does Intra-alveolar Pressure Rise and Fall? Boyle’s Law: gas pressure is inversely related to the space (volume) that it occupies 2. Expansion of alveoli causes decreased alveolar gas pressure and promotes inspiration Compression of alveoli causes increased alveolar gas pressure and promotes expiration Compliance refers to the ability of the lungs to expand which is important for inspiration (high compliance =easy expansion) Elasticity refers to the ability of the lungs to recoil, which is important for expiration Factors That Promote Expansion Factors That Promote Compression 1. Pleural fluid surface tension 1. Alveolar fluid surface tension 2. Negative intrapleural pressure 2. Elastic recoil of the lungs 3. Structural elements of the lungs (alveolar septal walls) Forced expiration can be accomplished when intrapulmonary pressure is reduced beyond that of quiet breathing; this is accomplished by actively recruiting additional muscles abdominal muscles: external oblique, internal oblique, transverse abdominus thoracic muscles: internal intercostals, latissimus dorsi, quadratus lumborum Recall, the flow of air through the passageways of the respiratory system is described by the following equation: Air Flow = Pressure 1 - Pressure 2 Resistance C. Air Flow resistance the pressure gradient between the alveoli and the atmosphere is the force that drives lung ventilation this driving force is opposed by resistance: the greatest resistance is encountered in medium sized bronchioles (at terminal bronchioles, diffusion takes over) although resistance in the bronchial tree is usually pretty low, it exists and can be related to this equation: length of tube X viscosity Resistance radius4 Factors Increasing Resistance Factors Decreasing Resistance bronchoconstriction bronchodilation -PNS -SNS -acetylcholine -epinephrine -histamine -increased pO2 -decreased pCO2 Other factors •solid obstructing tumors •mucus accumulation •inflammation Objective 8 External/Internal Respiration A. Basic Principles Dalton’s Law of Partial Pressures: the total pressure exerted by a mixture of gases is the sum of the pressures exerted individually by each of the gases in the mixture Note: the individual pressure of a single gas in a mixture is called partial pressure (p); and it is directly proportional to the percentage of that gas in the total mixture Thus: 760 mmHg = pN2 + pO2 + pCO2 + other gases..... Dalton’s Law And: pO2 = 20.9% X 760 mmHg 0.209 X 760 mmHg 159 mmHg pCO2 = 0.04% X 760 mmHg .0004 X 760 mmHg 0.3 mmHg Percentages of Atmospheric Gases What is the partial pressure of O2 in a space cabin filled with 60% O2 at total pressure of 380 mmHg? Assume little or no humidity. a.152 mmHg b.190 mmHg c. 228 mmHg d. 633 mmHg e. 684 mmHg Henry’s Law: when a mixture of gas comes into contact with a liquid, a gas will dissolve into the liquid in proportion to its partial pressure (p) and will diffuse until equilibrium is achieved (gases diffuse into and out of liquids from high to low partial pressure) As the partial pressure gradient rate of transfer Note: other factors that effect gas movement into and out of the blood are: •properties of the diffusion barrier (as thickness , rate of transfer •gas solubility (as solubility , rate of transfer •temperature of the liquid (as the temperature of the liquid , gas solubility B. External and Internal Respiration External Respiration: the diffusion of gases between the alveolar air and the blood in the pulmonary capillaries across the respiratory membrane O2 diffuses into the blood and CO2 diffuses out of the blood Internal Respiration the diffusion of gases between the blood of tissue capillaries and interstitial fluid CO2 diffuses into the blood and O2 diffuses out of the blood Gases diffuse into and out of the blood from high to low partial pressure Arterial Blood: pO2 = 100 mmHg pCO2 = 40 mmHg Venous Blood: pO2 = 40 mmHg pCO2 = 45 mmHg Remember - gases diffuse according to partial pressure gradients! Which way do they diffuse? External respiration Internal respiration Alveoli Arterial blood Partial pressures of alveolar air pO2 pCO2 104 mmHg 40mmHg Partial pressures arterial blood leaving alveolar capillaries pO2 pCO2 104mmHg 40mmHg Gas exchange pO2 pCO2 40mmHg 45mmHg Partial pressures venous blood entering alveolar capillaries Pulmonary capillaries Partial pressures arterial blood entering tissue pO2 pCO2 104mmHg 40mmHg Gas exchange Partial pressures venous blood leaving tissue pO2 pCO2 40mmHg 45mmHg Venous blood pO2 pCO2 < 40mmHg 45mmHg Partial pressures in tissue interstitial fluid Tissues Ventilation-Perfusion Coupling: When alveolar pO2 is low, local arterioles constrict When alveolar pO2 is high, local arteriole dilate When alveolar pCO2 is low, bronchioles constrict When alveolar pCO2 is high, bronchioles dilate Objective 9 Blood Gas Transport:O2 A. Oxygen Transport oxygen is transported through the blood in two ways about 1.5% of the O2 transported is dissolved in the plasma; this is the O2 that exerts partial pressure about 98.5% is carried by hemoglobin in RBC’s: Hb + reduced hemoglobin 4O2 Hb(O2)4 oxyhemoglobin Most important factor in determining how much O2 combines with Hb is ???? The Hb-O2 Dissociation Curve – describes the relationship between partial pressure and the % of O2 binding sites on Hb that are full % saturation (% HbO2) in arterial blood, at pO2 = 104 mmHg % saturation (% HbO2) in venous blood, at pO2 = 40mmhg Under normal circumstances, tissue only receive 25% of the O2 delivered to them by HbO2 The Hb-O2 Dissociation Curve S shaped curve with plateau At pO2 less than 40mm Hg the affinity of O2 for Hb is low. Think, where is pO2 40mm Hg? What does this mean for the unloading of O2 in the tissues? At pO2 = 60mm Hg Hb is 90% saturated, additional in pO2 has little effect the extent to which hemoglobin binds to oxygen depends on several factors, including pO2, pCO2, temperature and blood BPG levels the oxygen-hemoglobin dissociation curve demonstrates the effect of pO2 and the principle of cooperative binding pO2, veins pO2, arteries Factors that Favor a “Right Shift” (Reduce HbO2 Affinity): Increased temperature Elevated pCO2 Reduced pH Elevated 2,3 bisphosphoglycerate Factors that Favor a “Left Shift” (Increase HbO2 Affinity): Decreased temperature Reduced pCO2 Elevated pH Reduced 2,3 bisphosphoglycerate The 2,3-Bisphosphoglycerate Pathway in Erythrocytes note: the Bohr Effect refers to the effect of pH on hemoglobin/O2 affinity; low pH weakens the hemoglobin-O2 bond When tissues are active: •Increased CO2 is released •This increases H+ concentration (lowers pH) •At higher p CO2 and lower pH, O2 has a lower affinity for Hb •Therefore more O2 is released Globin binds to NO and protects it from being destroyed by heme: when HBO2 circulates to tissues, it releases both O2 and NO NO induces vasodilation and increases blood flow Whose hemoglobin has more O2 Affinity? Objective 10 Carbon Dioxide Transport carbon dioxide is carried in three ways 7-10% of the CO2 is dissolved in the plasma; this is the pCO2 that exerts partial pressure 20-30% of the CO2 diffuses into red blood cells and attaches to hemoglobin (not to heme, the globin portion): Hb + hemoglobin CO2 HbCO2 carbaminoglobin 60-70% of the CO2 diffuses into the red blood cell and is converted to HCO3- (bicarbonate) which is then carried in the plasma CO2 CO2 CO2 + H 2O + H 2O CO2 + Hb CO2 Haldane Effect: H+ + HCO3- HCO3- HCO3Cl- H+ HHbCO2 reduced Hb has a greater capacity to bind CO2 than HbO2 does Objective 11 Neural Control of Ventilation There are two clusters of neurons involved in the regulation of ventilation rate: Ventral Respiratory Group Location ventral medulla; extends from the pons to the spinal cord Function: sets the basic ventilation rate contains inspiratory neurons and expiratory neurons Dorsal Respiratory Group: Location: dorsal medulla, near the root of cranial nerve IX Function: integrate impulses from peripheral stretch receptors and chemoreceptors and relays them to the ventral respiratory group Ventral Respiratory Group Inspiratory Neurons Fire Impulses are carried to the diaphragm by the phrenic nerve and the external intercostal muscles by the intercostal nerves The thorax enlarges and inspiration occurs Inspiration lasts for 2 seconds Expiratory Neurons Fire Inhibitory impulses are delivered to the inspiratory neurons; the diaphragm and the external intercostals relax The thorax compresses and exhalation occurs Expiration lasts for 3 seconds The Pons Pontine Respiratory Center: modifies the basic rhythm in concert with vocalization, sleep, exercise and other activities Apneustic Center assists in the transition between inspiration and expiration Central receptors Peripheral chemoreceptors (aortic and carotid bodies) Dorsal respiratory group Pontine respiratory centers Modifies respiratory rhythm to match body activities Ventral respiratory group Other inputs include: Hypothalamus and cerebral cortex (I’m gonna hold my breath until you let me …) Respiratory diaphragm Peripheral stretch receptors (Herring Breuer Reflex) Inflation Reflex (Hering Breuer Reflex) lung inflation activates stretch receptors in the visceral pleura and in the conducting portions of the bronchial tree vagal afferents inhibit VRG neurons phrenic nerve is inhibited, inspiration stops Hypothalamus various stimuli (pain, fear, increased temperature) alter breathing rate/pattern The most important regulator of ventilation is arterial pCO2 concentrations pO2, pCO2, pH and Ventilation Rate ….. pCO2 and peripheral chemoreceptors: increased pCO2 leads to hyperventilation decreased pCO2 leads to hypoventilation Normal pCO2 in arteries is 40 mmHg Note: Hypercapnia is increased arterial pCO2 Hypocapnia is decreased arterial pCO2 The most important regulator of ventilation is arterial pCO2 concentrations Remember the value! Arterial PCO2 is 40 mmHg Central Chemoreceptors CO2 diffuses into the CSF and reacts with H2O to form H2CO3 the H+ that is generated activates central chemoreceptors decreased CSF pH leads to hyperventilation increased CSF pH leads to hypoventilation Normal arterial pO2 is 100 mmHg pO2 and peripheral chemoreceptors if pO2 falls below 60 mmHg, hyperventilation occurs ventilation rate is less sensitive to pO2 than pCO2 Arterial pH: Decreases in arterial pH lead to hyperventilation and increases in arterial pH lead to hypoventilation, even if the pO2 and pCO2 are normal Decreased arterial pH leads to hyperventilation Increased arterial pH leads to hypoventilation Terms used for ventilation eupnea: normal quiet breathing apnea cessation of breathing hyperpnea deep, vigorous breathing dyspnea difficult, labored breathing tachypnea rapid breathing Objective 12 Disorders Associated With Respiration Emphysema: Cause(s): decreased antitrypsin activity increased elastase activity compounded by smoking, pollution, aging and COPD Characteristics: permanent enlargement of respiratory bronchioles, alveolar ducts and alveoli destruction of alveolar walls loss of elasticity Leads to dyspnea, enlarged (barrel) chest, low diffusing capacity Emphysema Patient With “Barrel Chest” http://www.pathguy.com/lectures/emphysema_blues.jpg Asthma Cause(s): Intrinsic Asthma: caused by Type I hypersensitivity Extrinsic Asthma nonimmune; caused by infection, stress, inhaled irritants, drug ingestion or exercise Characteristics: chronic airway inflammation and hyperresponsive tracheobronchial tree leads to dyspnea, coughing wheezing and copious mucus secretion http://www.aaaai.org/patients/topicofthemonth/1105/images/asthma.jpg Tuberculosis Cause: Characteristics: Infection with Mycobacterium tuberculosis reactivation or reinfection produces respiratory symptoms: chest pain, bloody sputum, granulomas and lung cavitation can spread to other organs such as the skeleton, digestive viscera, adrenal glands, genitourinary tract and the heart http://www.hipusa.com/eTools/webmd/AZ_Encyclopedia/tuberculosis.jpg Lung Cavitation Lung Granuloma http://www.inflammation-atinterfaces.de/content/images/897fccd1 0585a8b8ce4ccd011563e178.jpg http://images.google.com/imgres?imgurl=http://w ww.granuloma.homestead.com/files/tb_gross_lun g44.jpg&imgrefurl=http://www.granuloma.home stead.com/TB_cavitary_gross.html&h=529&w=3 90&sz=53&hl=en&start=3&tbnid=5CMaF3cxp5CCM:&tbnh=132&tbnw=97&prev=/ima ges%3Fq%3Dlung%2Bcavitation%26gbv%3D2 %26svnum%3D10%26hl%3Den%26sa%3DG Bronchogenic Carcinoma genetic causes; smoking, air pollution, Cause: Characteristics: radiation exposure, industrial chemicals cough, weight loss, chest pain and dyspnea; increased sputum production; tumor obstruction of airways; frequent metastasis http://www.som.tulane.edu/cl assware/pathology/medical_ pathology/New_for_98/Lung _Review/Lung_carcinoma/Br onchogenicCA-gross.jpg Cystic Fibrosis Cause: Characteristics: defective gene encoding Cl- transporter in respiratory epithelial cells mucus accumulation leads to chronic cough, persistent lung infections, obstructive pulmonary disease digestive tract and reproductive tract also involved; malabsorption of nutrients, fat soluble vitamin deficiencies http://www.pathguy.com/l ectures/cystic_fibrosis.jp g Normal People People With Cystic Fibrosis http://www.the-aps.org/education/lot/cell/diag2.JPG