Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
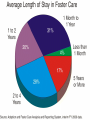
Fostering Hope: A Pediatrician’s Role in Caring for Children in Foster Care Hollie Edwards, MD Pediatric Grand Rounds November 6,Free 2015 Powerpoint Templates WHAT IS THE AVERAGE LENGTH OF STAY FOR A CHILD OR TEEN IN THE FOSTER CARE SYSTEM? 1. 2. 3. 4. 5 years 3 years 1 year 6 months 0% 1 0% 2 0% 3 0% 4 A HEALTHY 6 YEAR OLD FEMALE PRESENTS TO YOUR OFFICE THE DAY AFTER BEING PLACED WITH FOSTER PARENTS. YOU FIND OUT THAT NEGLECT FROM THE BIRTH PARENTS SECONDARY TO ALCOHOL ADDICTION LED TO THE PLACEMENT. PATIENT APPEARS WELL ON EXAM AND HAS NO KNOWN MEDICAL PROBLEMS. WHEN DO YOU NEED TO SEE HER BACK? 1. 2. 3. 4. 1 year 6 months 2 months 1 month 0% 1 0% 2 0% 3 0% 4 FOR A CHILD IN FOSTER CARE, WHO IS ABLE TO CONSENT FOR MEDICAL PROCEDURES? 1. 2. 3. 4. 5. 6. Foster parents Department of Social Services (DSS) Birth parents 1&2 2&3 All of the above 17% 1 17% 2 17% 17% 3 4 17% 5 17% 6 WHICH OF THE FOLLOWING SEQUELAE ARE TRUE CONCERNING THE IMPACT OF TRAUMA ON A CHILD? 1. 2. 3. 4. 5. 6. Chronically elevated stress hormones Development of permanent maladaptive behaviors Altered development of prefrontal cortex and hippocampus 1&2 1&3 All of the above 17% 1 17% 2 17% 17% 3 4 17% 5 17% 6 DISCLOSURES Neither myself nor Dr. Stephenson have any financial relationships to disclose. OBJECTIVES Gain overall knowledge about the process of the foster care system in America and the scope of the problem Review existing recommendations related to the special healthcare needs of children in foster care Become familiar with the sequelae of childhood trauma and adversity Review frequently confused topics related to foster care and medicine THE FOSTER CARE SYSTEM IN AMERICA Temporary service Protection and shelter for children who require out-of-home placement Opportunity for healing Ultimate goal- final placement in a stable, safe, permanent, and secure living arrangement SCOPE OF THE ISSUE Each year, more than 3 million children are involved in investigations of abuse or neglect Nearly 500,000 children are living in foster care on any given day The federal government spends about $4.4 billion a year to maintain children in foster care RACE STATISTICS AGE STATISTICS 40% are teenagers 30% are under the age of 5 Median age entering system 6.7 years Median age currently in system 9.2 years SOUTH CAROLINA DATA COUNTY DATA 0-5yo 6-12yo 13-17yo 18+yo Total Lexington 90 67 49 3 209 Richland 102 68 77 12 259 THE FOSTER CARE PROCESS Report and Referral After Hours Reporting: (803) 714-7444 Richland County DSS 24-Hour Hotline protective services intake Investigation Removal and Placement Service Planning Permanency Planning THE FOSTER CARE PROCESS Report and Referral After Hours Reporting: (803) 714-7444 Richland County DSS 24-Hour Hotline protective services intake Investigation Removal and Placement Service Planning Permanency Planning REASONS FOR REFERRALS Child maltreatment accounts for 70% Child neglect Sexual abuse Emotional abuse Physical abuse Disruptive behaviors Voluntary placements, <1% BIRTH PARENTS 79% have significantly impaired parenting skills* 31% with serious mental health problems 25% with active alcohol abuse 37% with active substance abuse 12% with cognitive impairment *National Survey of Child and Adolescent Well-being (wave 1) THE FOSTER CARE PROCESS Report and Referral After Hours Reporting: (803) 714-7444 Richland County DSS 24-Hour Hotline protective services intake Investigation Removal and Placement Service Planning Permanency Planning THE FOSTER CARE PROCESS Report and Referral After Hours Reporting: (803) 714-7444 Richland County DSS 24-Hour Hotline protective services intake Investigation Removal and Placement Service Planning Permanency Planning REMOVAL IS TRAUMATIC Even if the children came from bad circumstances, removal from family is emotionally traumatizing. This is the only world they have ever known. TYPES OF FOSTER CARE Family foster care Kinship foster care Pre-adoptive foster care Congregate care SOUTH CAROLINA PLACEMENT THE FOSTER CARE PROCESS Report and Referral After Hours Reporting: (803) 714-7444 Richland County DSS 24-Hour Hotline protective services intake Investigation Removal and Placement Service Planning Permanency Planning THE FOSTER CARE PROCESS Report and Referral After Hours Reporting: (803) 714-7444 Richland County DSS 24-Hour Hotline protective services intake Investigation Removal and Placement Service Planning Permanency Planning PERMANENCY PLANNING Options for permanent placing Reunification Adoption Guardianship to relative Emancipation from foster care system Mandated court reviews Guardian ad litem FOSTER CARE TEAM Department of Social Services (DSS) Caseworkers Foster parents Birth parents Guardian ad litem Pediatricians PEDIATRICIANS ARE A CRITICAL PART OF THE FOSTER CARE TEAM… OVERALL GOALS FOR PEDIATRICIANS Be a medical home Help child welfare agencies, foster families, and birth families minimize the trauma of placement separation Improve the child’s health and development during the period of foster care HIGH RISK POPULATION In 1995, a Government Accounting Office Report stated that children in foster care are “sicker than homeless children and children living in the poorest section of inner cities.” o Compared with children from the same socioeconomic background, they have much higher rates of serious emotional and behavioral problems, chronic physical disabilities, birth defects, developmental delays, and poor school achievement. BARRIERS TO GOOD HEALTH OUTCOMES Lack of a medical home Lack of medical records Inadequate and delayed assessment of needs upon entry into system Lack of follow-through in addressing identified needs Lack of access to other health services Diffusion of authority and responsibility Health providers’ lack of knowledge about child welfare and legal systems NATIONAL INVOLVEMENT AAP Council on Foster Care, Adoption, and Kinship Care Healthy Foster Care America Child Welfare League of America (CWLA) AAP RECOMMENDATIONS Health screening within 72 hours of placement into foster care A comprehensive evaluation within 30 days of placement Follow-up health visit within 60 to 90 days of placement Continuity of care Monthly for infants from birth to age 6 months Every 3 months for children age 6 to 24 months Twice a year for children and teens between 24 months and 21 years of age INITIAL HEALTH SCREENING Review the circumstances that led to placement Monitor adjustment to foster care home Inquire about the agency’s plans for permanency INITIAL HEALTH SCREENING Immunization status Review patient’s medical history Assess developmental or school progress Complete physical exam Height, weight, head circumference All body surfaces should be unclothed Genital and anal examination Laboratory tests when appropriate GENERAL TIPS FOR HEALTH CARE PROFESSIONALS Use respectful language Don’t label children or families Use the term “child in foster care” instead of “foster child” After each visit, contact the DSS caseworker Provide a copy of the health summary to the caseworker and foster parent COMPREHENSIVE EXAM Physical health Oral health Relational health Developmental health (if under 6yo) Educational health (if over 5yo) Mental/behavioral health PHYSICAL HEALTH About 50% have chronic medical problems Asthma Iron deficiency anemia Obesity or FTT Enuresis and encopresis Visual and hearing loss Neurological disorders Genetic disorders Infection (STI, TB) Increased lead levels ORAL HEALTH Approximately 35% enter foster care with significant dental and oral health problems Common problems: bottle tooth decay in young children multiple dental caries in older children AAP recommends that every child and teen entering foster care have a dental evaluation within 30 days of placement RELATIONAL HEALTH Children and teens often enter foster care without a model for normal, healthy family relationships They need to learn some of the basic principles of being a part of a healthy family Overall, foster care is intended to allow children to develop a sense of belonging DEVELOPMENTAL HEALTH 6x more likely to have developmental problems 60% of children <6yo enter foster care with developmental delay in at least one domain Use validated developmental screen Referrals for PT, OT, ST May be a role for developmental pediatric specialists EDUCATIONAL HEALTH Kindergarteners in foster care have half the vocabulary of their peers Nearly half are involved in special education and of these children, half have significant behavioral problems that lead to high rates of school suspensions and missed educational opportunities 8% of young adults completed a bachelors degree compared to the general population of 24% MENTAL/BEHAVIORAL HEALTH o Largest unmet health need for children and teens in foster care 30% of children in foster care vs. 4% of general population have emotional issues 5x more likely to have behavioral problems 16x more likely to carry a psychiatric diagnosis 8x more likely to be on psychotropic medications Consider referrals to mental health care professionals with expertise in trauma, posttraumatic stress disorder, grief, and separation issues HOW PEDIATRICIANS CAN HELP FOSTER PARENTS Explain health status Help access services Give advice on parenting Teach foster parents how to cope with child’s history of trauma HOW PEDIATRICIANS CAN HELP FOSTER PARENTS Explain health status Help access services Give advice on parenting Teach foster parents how to cope with child’s history of trauma STRESSORS Change in visitation with parents Change in school or child care settings Separation from siblings Parents going to rehab or jail Court dates Another child entering/leaving the foster home Being freed for adoption HOW PEDIATRICIANS CAN HELP FOSTER PARENTS Explain health status Help access services Give advice on parenting Teach foster parents how to cope with child’s history of trauma THE IMPACT OF CHILDHOOD TRAUMA Trauma experiences such as maltreatment, violence exposure, poverty, and impaired caregiving lead to chronic elevations in stress hormones As pediatricians, it is crucial to understand the impact of trauma on the developing brain and its translation into largely predictable emotions and behaviors We must be able to reframe behaviors for foster parents in ways that might be helpful to them in parenting the child PEDIATRICIANS ROLE IN CHILDHOOD TRAUMA: “TRAUMA INFORMED CARE” Identify traumatized child Educate families about toxic stress and the possible biological, behavioral, and social manifestations of early childhood trauma Empower families to respond to child’s behavior in a manner that acknowledges past trauma, but promotes the learning of new, more adaptive reactions to stress COMMON BEHAVIORS Poor affect regulation Impulsive Hyperactive Limited attention span Inflexible Dissociation Poor self concept Act younger than they are Insecure attachment Indiscriminately friendly Avoidant, ambivalent Do not know difference between anger and sadness REASONS FOR THESE COMMON BEHAVIORS These children have developed different ways of perceiving and reacting to their world, ways that often prove maladaptive in a more normal environment Altered neuroendocrine development ADVICE FOR FOSTER PARENTS Do not take these behaviors personally Help child understand your facial expression or tone Avoid yelling and aggression Come down to child’s eye level Validate their feelings Develop breathing techniques, relaxation skills, or exercises that the child can do when getting upset Praise the child for expressing feelings or calming down Be aware of your own emotional responses to child’s behaviors With time, patience, and practice, the child’s brain and body will learn more adaptive ways to respond to a new, safer environment SPECIAL ISSUES TRANSITIONING OUT OF FOSTER CARE AND IN TO ADULTHOOD Importance of mentorship Major decisions Need copy of: medical records including meds, immunizations, full history, birth, medical, and family history emergency contact info legal form with POA health insurance card contact info for former doc, dentist, counselor birth certificate and SS card high school diploma or GED photo ID MEDICAL CONSENT Legal guardianship remains with birth parents unless freed for adoption Whenever possible, the birth parents should make all important decisions and grant consent on behalf of their child DSS also has the ability to consent for routine medical treatment Foster parents do not have the authority to provide consent for medical procedures When freed for adoption, birth parents no longer have any legal rights CONFIDENTIALITY Medical information may be shared with caseworkers and foster parents Need to check with foster care agency before releasing information to birth parents Once freed for adoption, may not share information with birth parents Attorneys and court-appointed special advocates only have access to medical information through subpoena or written consent ADVOCACY OPPORTUNITIES Volunteering in agencies that serve children or teens in foster care Becoming a mentor Teaching independent living skills Advocating for services and policies at the federal and state level Starting a “backpack” program so that children in foster care have items for school Donating to a fund that pays to enroll children in foster care in extracurricular activities CONCLUSIONS The foster care system aims to uphold the health and well-being of children and teens in foster care, keep them safe, and promote stability It is our job as pediatricians to provide high quality health services, health care coordination, and advocacy on their behalf It is crucial to understand the impact of trauma on the developing brain and its translation into largely predictable emotions and behaviors We must be able to reframe behaviors for foster parents in ways that might be helpful to them in parenting the child WHAT IS THE AVERAGE LENGTH OF STAY FOR A CHILD OR TEEN IN THE FOSTER CARE SYSTEM? 1. 2. 3. 4. 5 years 3 years 1 year 6 months 0% 1 0% 2 0% 3 0% 4 A HEALTHY 6 YEAR OLD FEMALE PRESENTS TO YOUR OFFICE THE DAY AFTER BEING PLACED WITH FOSTER PARENTS. YOU FIND OUT THAT NEGLECT FROM THE BIRTH PARENTS SECONDARY TO ALCOHOL ADDICTION LED TO THE PLACEMENT. PATIENT APPEARS WELL ON EXAM AND HAS NO KNOWN MEDICAL PROBLEMS. WHEN DO YOU NEED TO SEE HER BACK? 1. 2. 3. 4. 1 year 6 months 2 months 1 month 0% 1 0% 2 0% 3 0% 4 FOR A CHILD IN FOSTER CARE, WHO IS ABLE TO CONSENT FOR MEDICAL PROCEDURES? 1. 2. 3. 4. 5. 6. Foster parents Department of Social Services (DSS) Birth parents 1&2 2&3 All of the above 17% 1 17% 2 17% 17% 3 4 17% 5 17% 6 WHICH OF THE FOLLOWING SEQUELAE ARE TRUE CONCERNING THE IMPACT OF TRAUMA ON A CHILD? 1. 2. 3. 4. 5. 6. Chronically elevated stress hormones Development of permanent maladaptive behaviors Altered development of prefrontal cortex and hippocampus 1&2 1&3 All of the above 17% 1 17% 2 17% 17% 3 4 17% 5 17% 6 REFERENCES Ahrens, KR. et al. Youth in foster care with adult mentors during adolescence have improved adult outcomes. Pediatrics 2008; 121 (2): e246-e252. “Foster Care.” American Academy of Pediatrics. Web. <www.aap.org/fostercare>. “Smart Spending.” Casey Family Programs. Web. <http://www.casey.org/smarter-spending/>. Committee on early childhood, adoption, and dependent care. Health care of young children in foster care. Pediatrics 2002; 109 (3): 536-540. Greiner, MV. et al. Foster caregivers’ perspectives on the medical challenges of children placed in their care: Implications for pediatricians caring for children in foster care. Clinical Pediatrics 2015. epub ahead of print. American Academy of Pediatrics District II New York State Task Force on Health Care for Children in Foster Care. Fostering Health: Health care for children and adolescents in foster care. Elk Grove Village, IL: American Academy of Pediatrics; 2005. Szilagyi, M. The pediatrician and the child in foster care. Pediatrics in Review 1998; 19 (2): 39-50. Jee, SH. et al. Foster care issues in general pediatrics. Current Opinion in Pediatrics 2008; 20 (6): 724728. Bruskas, D. Children in foster care: a vulnerable population at risk. Journal of Child and Adolescent Psychiatric Nursing 2008; 21 (2): 70-77. Task Force on Health Care for Children in Foster Care. Fostering health: Health care for children and adolescents in foster care, 2nd addition. New York: American Academy of Pediatrics, 2005. Print. Leslie, LK. Et al. Comprehensive Assessments for children entering foster care: A national perspective. Pediatrics 2003; 112 (1): 134-142. Halfon, N. et al. Health status of children in foster care. The experience of the Center for the Vulnerable Child. Arch Pediatr Adolesc Med. 1995; 149 (4): 386-392. Chernoff, R. et al. Assessing the health status of children entering the foster care system. Pediatrics. 1994; 93 (4): 594-601. American Academy of Pediatrics and Dave Thomas Foundation for Adoption. Helping Foster and Adoptive families cope with trauma: A guide for pediatricians. Elk Grove Village, IL: American Academy of Pediatrics; 2013. Schor, E. The foster care system and health status of foster children. Pediatrics 1982; 69 (5): 521-528. QUESTIONS?? (THIS EXCLUDES DR STALLWORTH)