Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
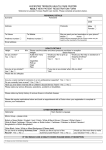
NEW PATIENT QUESTIONNAIRE Welcome to Plowright Medical Centre. Please help us by filling in this questionnaire as it can take a few weeks for your previous medical records to reach us. The information you give will be used to provide you with the medical care you need. PERSONAL INFORMATION Full Name…………………………………………..……………..…..……………Date of Birth…….…………………………………… Address & Postcode………………………………………………………………………..……………………….............................. Home Tel No………………..…………………….. Work Tel No……..…………………..………………...……………………… Mobile…………………………… Email Address………………………………………………………………….. Occupation………………………………………… Are you happy for us to contact you by.email: YES/NO Next of Kin: Name………………………..……………………… Relationship to you …………………………… Address…………………………………………………………………................................................................ Their contact telephone number…….……………..…………………………………………………………………… MILITARY BACKGROUND Do you or have you ever served in the military? Yes No (This question allows us to follow the military covenant guidelines) CARERS Are you a carer? Yes No If yes, please name the person you care for……………………………………………………………………..... Do you have a carer? Yes No If yes, please name the person who cares for you…………………………………………………………… LIFESTYLE Do you smoke? Yes No Never Smoked If yes, How many weekly? (Approx) ………………………………………………………………………………... Are you an ex-smoker? Yes No If you are an ex-smoker, in what year did you give up?....................................................... Do you drink alcohol? Yes No How many units of alcohol do you consume on a weekly basis of: Glasses of wine:……………………..…… Pints of beer:………………….……….. MEDICAL HISTORY d:\493731367.rtf Do you suffer from any of the following conditions listed below? Please tick Heart Problems Asthma/Chest Problems Stroke Epilepsy High Blood Pressure Cancer Diabetes Thyroid Problems Depression Memory Problems Other significant medical problems/pregnancies/operations you may think the surgery should know about……………………………………………………………………..……..………………………………………………………………………………………… ……………………………………………..…..……………………..…………………………………………………………………………………..……………..…… PREVIOUS MEDICAL PRACTICE Name of Practice ………………………………………… Usual GP ……………………………………………. Practice Address ……………………………………………………………………………………………………... Practice Telephone Number ………………………………………………………………………………………. MEDICATIONS If you are taking any medications, please state below. Please also supply us with a repeat slip from your previous surgery if you can. Name of drug……………………….……….Dose……………..……Frequency……………………..…………. Name of drug…………………………….….Dose………………..…Frequency…………………..……………. Name of drug………………………….…….Dose…………..………Frequency…………………..……………. Are you buying Aspirin regularly at the chemists? Yes No Please list any medications that do not agree with you……………………………………………….………… ……………………………………………………………………………………………….………………………... ALLERGIES Do you suffer with any allergies? Yes No If yes, please list…………………………………………………………………………………..…………………. FEMALE PATIENTS ONLY We provide a full range of contraceptive services at the surgery. What form of contraception do you use? ....................................................................................................................................................................... FAMILY HISTORY Have any of your family members suffered from: (Please tick) d:\493731367.rtf Asthma Diabetes Heart trouble below age 60 High Cholesterol Breast Cancer Heart trouble above age 60 High Blood Pressure Ovarian Cancer Stroke Bowel Cancer ETHNIC ORIGIN White British Mixed British Bangladeshi Irish Other White British Bangladeshi White/Black Caribbean White/Black African British Indian White & Asian Other Mixed British Pakistani Indian Other Asian Caribbean African Other Black Chinese Pakistani Other Main Spoken Language…………………………………………………………………… Do you require an interpreter ? Yes No Patient Signature …..………………………………………………………………………………. Date………………………………………..………… When you have answered all the questions, please return to reception. Please remember to bring a urine sample to your New Patient Medical. The reception staff will provide you with a sterile container. Thank you for taking the time to complete this questionnaire d:\493731367.rtf