Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
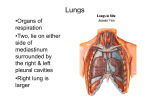
RADIOLOGY OF RESPIRATORY SYSTEM Weizhong Cheng Dept. Radiology, Zhongshan Hospital Institute of Medical Imaging, Shanghai AIMS •Basics •Best exam results •Appreciate the role radiology plays •? Instill an interest in radiology BEFORE CLASS: Textbook Reference book Literature Internet Apps Teacher & classmate Histology and Embryology Anatomy Pathology Internal Medicine Surgery Gynecology Pediatrics Neurology 。。。 Everything。。。U need to know METHODS X-ray CT MR DSA US Nuclear Medicine PET/CT Radionuclide ventilation perfusion imaging X-RAY TECHNIQUES PA (posteroanterior) & Lateral More information Two views Standardized Distance Pt needs to be stable Portable Quick Anywhere One shot No standardization Portable PA TECHNIQUES - PROJECTION •P-A (relation of x-ray beam to patient) TECHNIQUES - PROJECTION (CONTINUED) •A-P Supine/Erect TECHNIQUES - PROJECTION (CONTINUED) •Lateral TECHNIQUES - PROJECTION (CONTINUED) •Lateral •Oblique Decubitus TECHNICAL DETAILS •Type •Orientation •Rotation •Inspiration/expiration •Penetration ROTATION ROTATION (CONTINUED) PENETRATION INSPIRATION/EXPIRATION THINGS TO SEE ABCDE… Airways Bones Trachea, endotracheal tube, etc Clavicles, ribs, etc… Cardiac Diaphragm (Right hemidiaphragm slightly higher (~1.5 cm) Everything else (tubes), effusions DENSITIES The big two densities are: (1) WHITE - Bone (2) BLACK - Air The others are: (3) DARK GREY- Fat (4) GREY- Soft tissue/water And if anything Man-made is on the film, it is: (5) BRIGHT WHITE - Man-made ANATOMY ANATOMY BRONCHOPULMONARY ANATOMY CROSS-SECTIONAL ANATOMY OF LUNG SEGMENTS (CT) LOBES • Right upper lobe: LOBES (CONTINUED) • Right middle lobe: LOBES (CONTINUED) • Right lower lobe: LOBES (CONTINUED) • Left lower lobe: LOBES (CONTINUED) • Left upper lobe with Lingula: LOBES (CONTINUED) • Lingula: LOBES (CONTINUED) • Left upper lobe - upper division: HEART Right border: Edge of (r) Atrium 3. Left border: (l) Ventricle + Atrium 4. Posterior border: Reft Ventricle 5. Anterior border: Right Ventricle HEART (CONTINUED 。。。。) HEART IT’S NOT MINE…. HILUM Made of: 1. Pulmonary Art.+Veins 2. The Bronchi Left Hilum higher (max 1-2,5 cm) Identical: size, shape, density HILUM RIBS REVIEW AREAS: Apices • Behind the heart • Costophrenic angle (CPA) • Below the diaphragm • Soft tissues ( breast, surgical emphysema) • Ribs & clavicle •Vertebrae • ABNORMALS LUNG FINDINGS Darker areas radiolucent Pneumothorax Cysts/bulla Air bronchograms Lighter areas Opacities Atelectasis “infiltrates” Blood Pus Water Nodules or mass OPACITIES Lobar or not…. Pneumonia Pulmonary Edema “fluffy,” diffuse, “bat wing” distribution Hemorrhage Can’t tell by x-ray, need bronch RML pneumonia Opacities Opacities RLL pneumonia RUL pneumonia LLL pneumonia Consolidation on CT THE ENLARGED HILA Causes: 1. Adenopathies (neoplasia, infection) 2. Primary Tumor 3. Vascular 4. Sarcoidosis Mass Hilar Lymphadenopathy - BL Multiple Masses Metas Pleural Effusion Pulmonary Fibrosis Heart failure, Kerley A/B line (Interstitial lung hyperplasia edema) Heart failure Pneumothorax Emphysema Cavitating lesion Thin-walled Cavitating lesion 3mm Thick-walled Cavitating lesion Bronchiectasis Miliary shadowing CALCIFICATION Benign Patterns of Calcification Within a Solitary Pulmonary Nodule Chest Tube, NG Tube, Pulm. artery cath CT INDICATIONS KEY Clinical Factors Growth Pattern Size Margin (Border) Characteristics Density Contrast-Enhanced CT Other findings PULMONARY INFECTION dense multifocal segmental airspace opacification pneumonia air bronchograms lung abscess Pneumonia finding Lobar/segmental consolidation cavitation TUBERCULOSIS infiltrates Miliary shadowing Tuberculoma Chronic fibro-cavitary TB CAUSES OF SOLITARY PULMONARY NODULES (SPN) Neoplastic: Malignant Bronchogenic carcinoma Solitary metastasis Lymphoma Carcinoid tumor Neoplastic: Benign Hamartoma Benign connective tissue and neural tumors (e.g., lipoma, fibroma, neurofibroma) Inflammatory Granuloma Lung abscess Rheumatoid nodule Inflammatory pseudotumor (plasma cell granuloma) Congenital Arteriovenous malformation Lung cyst Bronchial atresia with mucoid impaction Miscellaneous Pulmonary infarct Intrapulmonary lymph node Mucoid impaction Hematoma Amyloidosis Normal confluence of pulmonary veins Mimics of SPN Nipple shadow Cutaneous lesion (e.g., wart, mole) Rib fracture or other bone lesion loculated pleural effusion NEOPLASTIC: BENIGN Hamartoma Bronchogenic carcinoma NEOPLASTIC: MALIGNANT NEOPLASTIC: MALIGNANT Bronchogenic carcinoma INFLAMMATORY Granuloma chest radiograph shows a small, wellcircumscribed, round opacity at the right lung base (arrows). Lateral view shows that the opacity is within the lung on two views (posterior segment of the right lower lobe) and thus represents a pulmonary nodule (arrow). Malignant SPN Contrast CT in Malignant Solitary Pulmonary Nodule. Thin-collimation (3mm) CT scans through left upper lobe nodule in a 62-year-old woman with biopsy-proven lung cancer shows a lobulated contour with positive enhancement of 50 H after contrast administration BRONCHOGENIC CARCINOMA(CLINICAL) Age at diagnosis: 55-60 years (range 40-80 years); M:F = 1.4:1 asymptomatic (10-50%) usually with peripheral tumors symptoms of central tumors: cough (75%), wheezing, pneumonia hemoptysis (50%), dysphagia (2%) symptoms of peripheral tumors: pleuritic/local chest pain, dyspnea, cough Pancoast syndrome, superior vena cava syndrome hoarseness symptoms of metastatic disease (CNS, bone, liver, adrenal gland) paraneoplastic syndromes: cachexia of malignancy clubbing + hypertrophic osteoarthropathy nonbacterial thrombotic endocarditis migratory thrombophlebitis ectopic hormone production: hypercalcemia, syndrome of inappropriate secretion of antidiuretic hormone, Cushing syndrome, gynecomastia, acromegaly RISK FACTORS Cigarette smoking (squamous cell carcinoma + small cell carcinoma) 鈥搑elated to number of cigarettes smoked, depth of inhalation, age at which smoking began 85% of lung cancer deaths are attributable to cigarette smoking! Passive smoking may account for 25% of lung cancers in nonsmokers! Radon gas: may be the 2nd leading cause for lung cancer with up to 20,000 deaths per year Industrial exposure: asbestos, uranium, arsenic, chlormethyl ether Concomitant disease: chronic pulmonary scar + pulmonary fibrosis Scar carcinoma 45% of all peripheral cancers originate in scars! Incidence: 7% of lung tumors; 1% of autopsies Origin: related to infarcts (>50%), tuberculosis scar (<25%) Histo: adenocarcinoma (72%), squamous cell carcinoma (18%) Location: upper lobes (75%) TYPES: Adenocarcinoma (50%) Most common cell type seen in women + nonsmokers Intermediate malignant potential (slow growth, high incidence of early metastases) almost invariably develops in periphery; frequently found in scars (tuberculosis, infarction, scleroderma, bronchiectasis) + in close relation to preexisting bullae solitary peripheral subpleural mass (52%)/alveolar infiltrate/multiple nodules may invade pleura + grow circumferentially around lung mimicking malignant mesothelioma upper lobe distribution (69%) air broncho-/bronchiologram on HRCT (65%) calcification in periphery of mass (1%) smooth margin/spiculated margin due to desmoplastic reaction with retraction of pleura solitary peripheral mass Adenocarcinoma Presenting as Solitary Pulmonary Nodule. A.Cone-down view of posteroanterior radiograph shows nodule in the right mid-lung (arrow). B.Thin-section CT shows 12-mm nodule with spiculated margins (arrow) in the superior segment of the right lower lobe. Transthoracic needle biopsy revealed adenocarcinoma. Squamous cell carcinoma (30-35%) Strongly associated with cigarette smoking Central location within main/lobar/segmental bronchus (2/3) large central mass & cavitation distal atelectasis & bulging fissure (due to mass) postobstructive pneumonia All cases of pneumonia in adults should be followed to complete radiologic resolution! airway obstruction with atelectasis (37%) Solitary peripheral nodule (1/3) characteristic cavitation (in 7-10%) Squamous cell carcinoma is the most common cell type to cavitate! invasion of chest wall Squamous cell carcinoma is the most common cell type to cause Pancoast tumor Central lung cancer Squamous Cell Carcinoma. A.Posteroanterior chest film in a 58-year-old male smoker with hemoptysis shows a left hilar mass with left upper lobe atelectasis. B.Enhanced CT scan shows the left hilar mass occluding the left upper lobe bronchus with an endobronchial component (straight arrow). Note the presence of mucus bronchograms within the atelectatic lung (curved arrow) Squamous Cell Carcinoma Small cell undifferentiated carcinoma (15%) Strongly associated with cigarette smoking Rapid growth + high metastatic potential typically large hilar/perihilar mass often associated with mediastinal widening (from adenopathy) extensive necrosis + hemorrhage small lung lesion (rare) Large undifferentiated cell carcinoma (<5%) Strongly associated with smoking large bulky usually peripheral mass >6 cm (50%) large area of necrosis pleural involvement large bronchus involved in central lesion (50%) Large-cell bronchogenic carcinoma small-cell bronchogenic carcinoma GROUND-GLASS OPACITY the pattern was shown to be caused by predominantly interstitial diseases in 54% of cases, equal involvement of the interstitium and airspaces in 32%, and predominantly airspace disease in 14% GGO is an important finding. In certain clinical circumstances, it can suggest a specific diagnosis, indicate a potentially treatable disease, and guide a bronchoscopist or surgeon to an appropriate area for biopsy Pure GGO( Ground-glass Opacity) Early stage 98,6,17 Lung cancer:solid nodules 12*8mm ,Lobular resection,8 yrs alive SELF TEST? MR INDICATIONS NEVER STOP LOOKING, CARRY ON WITH YOUR SYSTEMATIC APPROACH!!