Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
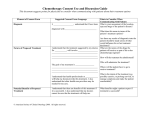
HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: USE THE APPROVED LETTERHEAD FOR YOUR INSTITUTION OFFICIAL TITLE OF PROJECT (Lay title in non-technical Language such as A study to see whether treatment A or treatment B is better for patients with cancer XXXX.) CONSENT FORM This form is part of the process of informed consent. It is designed to explain this research study and what will happen to you if you choose to be in this study. If you would like to know more about something mentioned in this consent form, or have any questions at anytime regarding this research study, please be sure to ask your doctor or nurse. Read this consent form carefully to make sure you understand all the information it provides. You will get a copy of this consent form to keep. You do not have to take part in this study and your care does not depend on whether or not you take part. (IF the sponsor is a drug company) This study is sponsored by (Pharmaceutical Company), the company that manufactures the drug (drug name) to be used in this study. This study will take place at various centres throughout Canada and the United States and the Cross Cancer Institute/Tom Baker Cancer Centre is one of the centres. (The Sponsor) will reimburse Alberta Health Services for costs related to conducting this study. (OR IF the sponsor is a cooperative group) This study is being conducted by the Radiation Therapy Oncology Group (RTOG) a cooperative oncology research group of which the Cross Cancer Institute/Tom Baker Cancer Centre is a member. This study will take place at various centres throughout Canada and the United States, and the Cross Cancer Institute/Tom Baker Cancer Centre is one of the centres. (Pharmaceutical Company) which manufactures the drug (drug name) will supply the drug for the study. Alberta Health Services will be reimbursed for research related costs. (IF the patient's physician is part of the study team:) Your doctor, who is one of the researchers, will discuss the study with you. (OR IF the patient's physician is not part of the study team:) Your doctor has given us permission to ask you to be in this study. Your participation in this study is entirely voluntary. Please take your time to make your decision. It is recommended that you discuss with your friends and/or family about whether to participate in this study. (Site Specific Footer) Page 1 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: “WHY IS THIS STUDY BEING DONE?” You are being asked to take part in this study because you have (type of) cancer. (All studies -- give specifics of what the standard treatment is, what its response rate is, and/or effects and/or outcome, and why this study is worth doing and, if a drug is involved, what is different about this drug compared to standard therapy? State what the experimental aspects of the study are.) This study is being done because___________. (Explain in one or two sentences. Examples are: “Currently, there is no effective treatment for this type of cancer,” or “We do not know which of these two commonly-used treatments is better.”) “WHAT DO WE HOPE TO LEARN?” We hope to learn (purpose). The purpose of this study is to (see below)________________. (Ensure that you include the primary and secondary objectives of the study.) Describe what the phase of this study means. (If Applicable) (Phase I study): Test the safety of (Drug/Intervention) and see what effects (good and bad) it has on you and your cancer. OR Find the highest dose of a (Drug/Intervention) that can safely be given without causing severe side effects. In order to determine this dose, some patients on this study may experience severe side effects. (Phase II study): To find out what effects (good and bad) (Drug/Intervention) has on you and your (type of) cancer. (Phase III studies): To compare the effects (good and bad) of the (New Drug/Intervention) with (commonly used Drug/Intervention) on you and your (type of) cancer to see which is better. “WHAT IS INVOLVED IN THIS STUDY?” In this study, you may receive one of ____ treatments. You will be “randomized” to receive one of the treatments described below. Randomization means the treatment that you are assigned will be determined by chance. It is like flipping a coin. Randomization is done by a computer. Neither you nor the researcher will choose which treatment you will be assigned. You will have an (Equal/One in Three/Etc.) chance of being assigned to treatment A - Z. You and your doctor will not be told which treatment you are receiving. (Only applies to double- (Site Specific Footer) Page 2 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: blind randomized studies) You will be followed to see what effect the treatment(s) has/have on your health. (It is easier for the patient to understand the treatment schema in either a table or flow chart.) For Example Day 1, Treatment A Treatment B 5-FU CPT-11 Leucovorin 5-FU CPT-11 Radiation Therapy Day 5 X Day 9 Day 11 Day 15 X X X X X X X X X Day 17 X X X X X X OR Treatment A – (Describe) Example: If you get treatment A, you will have to come to the outpatient department at the Cross Cancer Institute/Tom Baker Cancer Centre twice a week for a total of 8 weeks. During these visits, you will be given treatment A. Treatment B – (Describe) Example: If you get treatment B, you will have to be admitted to the University of Alberta/Calgary Hospital for three days at the beginning of the study. During your hospital stay, you will be given treatment B. (If the elements of the treatment are common for all treatments do one paragraph for all the treatments and wherever possible use table formats.) “HOW MANY PEOPLE WILL TAKE PART IN THIS STUDY?” About ( ) people will take part in this study (at the CCI, TBCC or worldwide?) “WHAT WILL MY PARTICIPATION INVOLVE?” If you take part in this study, you will have the following tests and procedures: (List procedures and their frequency under the categories below in a table format. For randomized studies, list the study groups and under each describe categories of procedures. Include whether a patient will be at home, in the hospital, or in an outpatient setting. If (Site Specific Footer) Page 3 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: objectives include a comparison of interventions, list all procedures even those that are considered standard) (Wherever possible use a table format for each of the following): Procedures that are part of regular cancer care and may be done even if you do not join the study. Standard procedures being done because you are in this study. Procedures that are being tested in this study. An example of a table Initial X X X X Day 14 X Blood Test Lung Function Test X-Rays & Scans X Quality of Life Questionnaire (time to complete) Physical Exam – blood X X pressure, etc (Use and modify the table which exists in the protocol to a lay version). Day 28 X X X X X (If Applicable) Pathology Review (Do not use if Pathology Review is NOT part of the study) All or some of your tumour was removed by biopsy or surgery. Some of this tumour tissue was examined by a pathologist to help make your diagnosis. The remaining tumour tissue is stored in the pathology department. If you participate in this study, this tissue will be sent to (a central office) for review and research investigation associated with this protocol (list tests that will be performed). You will not have to provide any other tissue. After the study testing is finished, any tissue left will be destroyed. (If Applicable) Sample Banking for Future Research You may also be asked whether your (tissue/blood) can be stored for future research. If so, you will be given another consent form asking for your permission. (If this condition applies to your application, then ensure to include the tissue/blood banking consent form.) (Site Specific Footer) Page 4 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: “HOW LONG WILL I BE INVOLVED IN THE STUDY?” You may be in this study for as long as (Months/Weeks, until a certain event). (Where appropriate, state that the study will involve long-term follow-up.) “WHAT ARE THE SIDE EFFECTS?” Every medical treatment including the standard treatment has side effects, which your doctor will explain to you. It is important that you know and understand the possible side effects of the treatments given in this study. (If Applicable) (IF the study involves radiation treatment) You will receive a separate sheet and/or booklet that will give you more information about treatment involving radiation. (OR IF the study involves chemotherapy) You will receive a separate sheet and/or booklet that will give you more information about treatment involving chemotherapy. (Combine the two sentences if both radiation and chemotherapy are given in this study.) The following are the side effects of each drug used in this study. These side effects may or may not be more severe when the drugs are taken together. These are the side effects we know about at present. However, since this is a study of new treatments there may be other side effects that we do not know about yet. (Site Specific Footer) Page 5 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Drug Route Zoledronic IV Acid Version Date: Common Fever Fatigue (tiredness) Anorexia or loss of appetite Less Common Headaches Low levels of calcium in the blood, which may cause muscle cramps Insomnia Anxiety Rare Kidney failure Severe allergic reactions Permanent damage to the jawbone and might require surgery to remove the damaged area. This might be more likely to happen in patients who have certain dental procedures. If you see a dentist, you should inform them that you may be receiving zoledronic acid. (Use the following sample table and if possible keep the table on one page) IV = Intravenous (into a vein) SC = Subcutaneous (under the skin) IM = Intramuscular (in a muscle) PO= Oral (by mouth) (If there are additional side effects that you feel should be mentioned in the context of this study, please list) You may feel some discomfort from the needle when study treatments are given or blood drawn. There is also a small risk of fainting, swelling, bruising, bleeding or (rarely) local infections at the site of the needle punctures which will be used for giving your study medications, as well as for taking blood samples. (Applicable for studies with CT component) As part of this study, you will have CT scans and/or x-rays. There is a potential risk of radiation exposure from these CT scans and x-rays, however, this risk is considered small. The amount of radiation exposure from one CT scan is (Site Specific Footer) Page 6 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: about the same as the amount of radiation a person would get from natural surroundings in three years. Sometimes an intravenous (into a vein) contrast dye is given with a CT scan. Although the dye is relatively safe, occasionally side effects or reactions occur. These may be mild (such as skin rash or hives) to severe (such as breathing difficulties or shock). The doctors and staff of the Radiology Department are trained to treat these reactions if they occur. Even if you do not participate in a study, you may need CT scans as part of standard care. If you participate in this study, you might receive more scans than your doctor would normally do. These side effects may be temporary, long term and/or permanent. However, most of the side effects listed above are reversible. That means they will stop once the drug is discontinued or its dose lowered. (State long-term side effects if any, e.g. second malignancies, infertility, etc. in the table) If you have any side effects, either those on the list or others, or if you want more information on how the drug(s) could affect you, you should call the doctor or nurse in charge of the study. Their telephone numbers are on page (insert page #) of this form. If we get any new information about the drugs/treatments/side effects in this study, you will be told about them so that you can continue to get the best care possible. Unique Side Effects/Special Precaution List side effects that are unique or precautions that need to be taken that may prevent and/or intensify side effects. "WHAT ARE THE REPRODUCTIVE RISKS?" The effects of (drug) on the human reproductive system are unknown. There may be unforeseeable risks to a pregnant woman and/or fetus. Therefore, it is very important that if you are sexually active (male/female), you use an effective method of birth control during participation in the study and for three months following treatment. This may include, but is not limited to, abstinence, birth control pills, an IUD, condoms, implants or being surgically sterilized. While you agree to take the necessary precautions for birth control, it is very important that your partner uses an effective method of birth control as well. If you or your partner becomes pregnant during the course of the treatment, you must inform your doctor immediately. Your doctor will ensure that you receive information about the options available in relation to the pregnancy and that you and your partner are fully supported in whichever option is chosen. The effect of (drug) in breast milk is also unknown. If you are breast-feeding, you cannot participate in the study. (Site Specific Footer) Page 7 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: “WHAT ARE MY RESPONSIBILITIES?” You must be willing to attend all scheduled study visits and undergo all of the procedures described above. It is very important that you inform the study doctor or study nurse of any side effects or health problems that you may be experiencing as well as any medications (prescribed or holistic) that you are taking while on this study. (If applicable, include statement about Quality of Life questionnaires, medication diaries etc.) “WHAT ARE MY ALTERNATIVES?” You may choose not to participate in this study. Other treatments that could be considered for your cancer may include the following: (1) radiation therapy; (2) chemotherapy; (3) surgery; or (4) no treatment except medications to relieve symptoms. These treatments could be given either alone or in combination with each other. Please talk to your doctor about the known benefits and risks of these other treatment options. Your doctor can also discuss with you what will happen if you decide not to undertake any treatment at this time. With the last choice (4), your cancer is expected to grow and your disease could spread. “ARE THERE ANY BENEFITS TO PARTICIPATING IN THIS STUDY?” Participation in this study may or may not be of personal benefit to you. However, based on the results of this study, it is hoped that, in the long-term, patient care can be improved. "WHAT HAPPENS IF I BECOME SEVERELY ILL?” (For double-blinded studies only:) You and your doctor will not be told which study treatment you are receiving except in the case of an emergency. If you have an emergency, your doctor will be told which study treatment you are receiving so that you can get proper care. “CAN I WITHDRAW FROM THIS STUDY?” In discussion with you, your doctor at the Cross Cancer Institute/Tom Baker Cancer Centre, either at his/her own initiative or at the request of the sponsor of this study, may withdraw you from the study at any time if it is in your best interests. Taking part in this study is voluntary; you may withdraw from the study at any time if you wish to do so. If you decide to stop participating in the study, we encourage you to talk to your doctor first. (Site Specific Footer) Page 8 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: Your doctor can take you off the study treatment early for reasons such as: The treatment does not work for you and your cancer gets worse. You are unable to tolerate the study treatment. New information becomes available that indicates the study treatment is no longer in your best interest. Your doctor no longer feels this is the best treatment for you. If you stop treatment early, we would like to keep track of your medical condition indefinitely to look at the long-term effects of the study treatments. (If required) Should you decide to withdraw from the study at any time, information collected on you up until that point would still be provided to (the Sponsor). “ARE THERE COSTS TO ME FOR TAKING PART IN THIS STUDY?” (IF all elements of the treatment are free:) You will not have to pay for the treatment you receive in this study. (IF some payment is required:) You will not have to pay for drug A/Treatment B used in this study. However, you will need to pay for drug C [note especially: G-CSF]. You will have to pay for the drugs you need for side effects. If you are covered by a private insurance company, you may get some or all of your money back, but if you do not have private insurance, you will not get any money back. (OR All studies where at least some of the treatment cost is covered by the sponsoring agency:) It is also possible that the Sponsor (Sponsor's name) that is providing the drug(s) (name the drug(s)) may decide to put the drug (name the drug(s)) on the market. After the study is over, you may have to pay for the drug if you continue on it. (If there are expected to be extra costs, please estimate how much.) (IF extra visits are required:) You will be coming to the Cross Cancer Institute/Tom Baker Cancer Centre more often than if you were not part of this study. There may be additional costs to you for taking part in this study such as: parking transportation meals babysitting, etc. You may be eligible for reimbursement of reasonable, out-of-pocket expenses related to your participation in this study. Please speak with your study doctor or study nurse regarding this. “WHAT ARE MY RIGHTS AS A PARTICIPANT?” If you suffer an injury or become ill as a result of participating in this research, you will receive all medical treatments (or services) recommended by your doctors. No compensation will be (Site Specific Footer) Page 9 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: provided beyond this point. However, it is important to note that nothing said in this consent form alters your legal rights to recover damages (e.g. legal action). If new information becomes available or there are changes to the study that may affect your health or willingness to continue in the study, you will be told in a timely manner. “WILL MY PERSONAL INFORMATION BE KEPT CONFIDENTIAL?” Identifiable health information will be collected from you and from your Provincial Electronic Health Record (NetCare) during this study. This information may be used by the researchers who are carrying out this study, and may be disclosed to others as described below. Any research proposal to use information that identifies you for a purpose other than this study must be approved in advance by the Health Research Ethics Board of Alberta – Cancer Committee. Direct access to your identifiable health information collected for this study will be restricted to the researchers who are directly involved in this study except in the following circumstances: Your identifiable health information may need to be inspected or copied from time to time for quality assurance (to make sure the information being used in the study is accurate) and for data analysis (to do statistical analysis that will not identify you). The following organizations may do this inspection: Health Canada, the Canadian regulatory body United States Food and Drug Administration, the United States regulatory body Health Research Ethics Board of Alberta – Cancer Committee Members of the Regulatory/Audit team at the Cross Cancer Institute/Tom Baker Cancer Centre, for quality assurance purposes National Cancer Institute of Canada, the organization that is coordinating this study Sponsor's name. Authorized representatives of the makers of the drugs you are taking in this study and/or a clinical research organization coordinating the study Other regulatory agencies that may need to see these records in order to monitor the research and verify the accuracy of the study data such as (insert examples of relevant foreign regulatory agencies equivalent to Health Canada or FDA; e.g., the European Medicines Agency) Any disclosure of your identifiable health information will be in accordance with the Alberta Health Information Act. As well, any person from the organizations listed above looking at your records on-site at the Cross Cancer Institute/Tom Baker Cancer Centre will follow the relevant Alberta Health Services and relevant Health Research Ethics Board of Alberta – Cancer Committee policies and procedures that control these actions. Any disclosure of your identifiable health information to another individual or organization not listed here will need the approval of the Health Research Ethics Board of Alberta – Cancer Committee. (Site Specific Footer) Page 10 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: Your identifiable health information collected as part of this study (if applicable) which includes records of your progress, your responses to the questionnaires and your diaries will be kept confidential in a secure AHS facility. Information that does not identify you will also be provided to (the Sponsor) or other companies acting on behalf of (the Sponsor), where it will be kept confidential in a secure location. The researchers who are directly involved in your study may share information about you with other researchers, but you will not be identified in that shared information except by a number. The key that indicates what number you have been assigned will be kept secure by the researchers directly involved with your study and will not be released. Although absolute confidentiality can never be guaranteed, Alberta Health Services will make every effort to keep your identifiable health information confidential, and to follow the ethical and legal rules about collecting, using and disclosing this information in accordance with the Alberta Health Information Act and other regulatory requirements. The information collected during this study will be used in analyses and will be published and/or presented to the scientific community at meetings and in journals, but your identity will remain confidential. This information may also be used as part of a submission to regulatory authorities around the world to support the approval of the drug used in this research. It is expected that the study results will be published as soon as possible after completion. Your study doctor will be informed of the results of the study once they are known. (The following statement must be reproduced word-for-word in informed consent documents for applicable clinical trials: ) A description of this clinical trial will be available on http://www.ClinicalTrials.gov, as required by U.S. Law. This Web site will not include information that can identify you. At most, the Web site will include a summary of the results. You can search this Web site at any time. This study’s registration ID number to use on this web page is: XXXXXXXXXXX (Please include the study registration ID for this trial). “WHERE CAN I GET MORE INFORMATION” (Optional) For your reading, the Organization (Name of Organization) has a booklet titled “(Name of booklet)”, which is available from your doctor. Or include a website if available for that type of cancer. (Site Specific Footer) Page 11 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: “WHO DO I CALL IF I HAVE QUESTIONS OR PROBLEMS?” For information about your disease and/or research related injury/illness, you may contact the Principal Investigator (name and telephone number), Co-Investigator (name and telephone number), Research Nurse (name and telephone number) or page them through the Cross Cancer Institute/Tom Baker Cancer Centre Switchboard at (XXX) XXX-XXXX to answer any questions you have about this study. If you have questions about your rights as a participant or about ethical issues related to this study and you would like to speak to someone not involved in the conduct of the study, please contact the Office of the Health Research Ethics Board of Alberta – Cancer Committee at: 780-423-5727 or toll-free 1-877-423-5727. Only include for Alberta Health Services studies - If your doctor or study nurse has not been able to answer or resolve your questions and/or concerns about this study, or if you feel at any time that you have not been informed to your satisfaction about the risks, benefits, or alternatives to this study, or that you have been encouraged to continue in this study after you wanted to withdraw, you can call the Alberta Health Services Patient Relations Department toll free at 1-855-550-2555. (Please check www.albertahealthservices.ca for the appropriate telephone numbers.) (Site Specific Footer) Page 12 of 13 HREBA-CC Main ICF Template Final v2015_November Protocol/Study #: Version Date: UNDERSTANDING OF PARTICIPANTS I can refuse to take part or withdraw from this study at any time without jeopardizing my health care. If I continue to take part in the study, I will be kept informed of any important new developments and information learned after the time I gave my original consent. I also give consent for the Principal Investigator and Alberta Health Services (the Custodian) to disclose identifiable health information, as per the Alberta Health Information Act, to the organizations mentioned on the previous pages. I have read and understood all of the information in this consent form. I have asked questions, and received answers concerning areas I did not understand. I have had the opportunity to take this consent form home for review and discussion. My consent has not been forced or influenced in any way. I consent to participate in this research study. Upon signing this form I will receive a signed copy of the consent. (PRINT NAMES CLEARLY) ____________________________ Name of Patient ____________________________ Name of Person Obtaining Consent ___________________________ Signature of Patient ___________________________ Signature of Person Obtaining Consent ___________________________ Date ___________________________ Date Patient Study Number or Hospital Number: _____________________ Was the patient assisted during the consent process in one of the ways listed below? □ Yes □ No If yes, please check the relevant box and complete the signature space below: □ The consent form was read to the patient, and the person signing below attests that the study was accurately explained to, and apparently understood by the patient. □ The person signing below acted as a translator for the patient during the consent process. ________________________________ Signature of person assisting In the consent discussion ____________________________ Date Please note: More information regarding the assistance provided during the consent process should be noted in the medical record for the patient if applicable. Page 13 of 13