Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Moral treatment wikipedia , lookup
Mental health in Russia wikipedia , lookup
Self-help groups for mental health wikipedia , lookup
Mental health wikipedia , lookup
Pyotr Gannushkin wikipedia , lookup
Mental disorder wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Clinical mental health counseling wikipedia , lookup
Involuntary commitment internationally wikipedia , lookup
Mental health professional wikipedia , lookup
Abnormal psychology wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Psychiatric survivors movement wikipedia , lookup
Lifetrack Therapy wikipedia , lookup
Deinstitutionalisation wikipedia , lookup
Community mental health service wikipedia , lookup
Taken from NHS Virtual Learning Environment module on Scotland’s Mental Health
First Aid for Young People
Mental health definitions
Mental health has a personal meaning for every individual. Here are some definitions of different
aspects:
Mental wellbeing: a term that includes life satisfaction and how we feel about ourselves. This
covers a range of things such as sense of control, having a purpose in life, a sense of
belonging and positive relationships. Mental wellbeing can be experienced despite having a
diagnosis of a mental health problem – in this respect mental health can be considered as two
intersecting continua, mental wellbeing and mental health problems.
Mental health: used as an umbrella term to refer to both mental health problems and mental
wellbeing.
Mental health problems: a term that refers to symptoms that meet the criteria for clinical
diagnosis of mental health problems. Examples include depression, anxiety and eating
disorders.
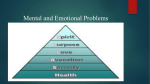
Mental health continuum
A helpful way to think about mental health is as part of a continuum ranging from minimum
mental wellbeing to maximum mental wellbeing, taking in maximum mental health problems to
minimum mental health problems.
The four quadrants in the mental health continuum shown opposite (adapted from K. Tudor,
1996, Mental health promotion: paradigms and practice) represent different possible times and
situations in a person's life.
We can move around the continuum for many reasons. Our mental wellbeing can be affected by
circumstances outside our control, as well as by the way we look after ourselves.
When things that we cannot control have a negative effect on our mental wellbeing, we can do
something positive by taking good care of ourselves.
Models of health
A widely accepted definition of health is: "a state of complete physical, mental and social
wellbeing and not merely the absence of disease or infirmity". (World Health Organization).
Health may also include people's ability to lead a socially and economically productive life.
Dahlgren G, Whitehead M (1992) give us a social model of health (see diagram on next screen),
describing factors that influence people's health and wellbeing and determine inequalities – from
socio-economic factors to lifestyle. Importantly, future health inequalities are, to a large extent,
determined from a child's earliest years. Early responses to the needs of children and young
people through mental health first aid will help to tackle some of the inequalities which will affect
future physical and psychological functioning.
Age, gender and hereditary factors can affect mental health:
constitution – long-term physical illness for example can make a person more likely to develop
mental health problems, particularly depression; depression may stifle the potential for good
relationships.
gender – girls are more likely to develop eating disorders, with distorted ideas of body image
and low self esteem; eating disorders might interrupt education.
age – adolescents, through peer pressure, can feel they have to conform with a high degree of
anxiety attached; excessive alcohol for example may increase the risk of physical or sexual
abuse, potentially resulting in life long mental health problems
suicide is the major cause of death for people under the age of 35.
Lifestyle factors can affect mental health and vice versa, for example:
regular physical exercise is known to have a positive effect on mental wellbeing
young people growing up in households with alcohol dependent adults are more at risk of
developing mental health problems
a family's belief system can lead to a young person being bullied and seen as 'different', leading
to potential mental health problems, such as self harm. Self harm can lead to further isolation
from social networks.
Social network factors can affect mental health and vice versa, for example:
good social relationships, friendships and belonging are important parts of sustaining mental
wellbeing
alienation through racism, bullying/cyberbullying, can lead to isolation, anxiety and depression
and other mental health problems
young LGBT people can become isolated from their peer groups through significant levels of
homophobic bullying, leading to self harm or suicide
depression can affect a young person's sense of belonging and isolate them further from a
source of social support.
Living and working conditions can affect mental health and vice versa, for example:
mental health problems are more common in areas of deprivation, poor housing and access to
services
unemployment, and limited opportunity is consistently associated with poor mental health
less education and low income or material standard of living, in addition to poor physical health
are also associated with mental health problems.
Socio-economic, environmental and cultural factors will affect a society's mental wellbeing
and vice versa, for example:
mental health problems are both a cause and a consequence of social, economic and
environmental inequalities
by making structural changes to economic, cultural and environmental conditions there could
be a beneficial effect on society's mental wellbeing.
Attitudes, inequalities and stigma
The way in which we think and feel about our own and others' mental health depends very much
on our attitudes and beliefs.
Our attitudes and beliefs are influenced by a whole range of factors. The Frame of Reference
diagram opposite can help us to think of some of the things that have developed our attitudes
and beliefs about mental health.
Your personal experiences and influences have developed your own window on the world and
we all have a different frame of reference.
Frame of Reference, developed by Jacqui and Aaron Schiff.
Common mental health problems and young people
The aim here is to introduce, briefly, a range of mental health problems that you may well
encounter in your work with young people.
More common mental health problems, include:
depression
anxiety
self harm
alcohol and drug use
Depression
Everyone can feel sad or low when things are not going well. However, a normal low mood is not
depression, is short term and people recover without treatment. Characteristics of depression
include:
low mood that lasts for at least two weeks
lack of energy
lack of interest in things previously of interest
affects ability to carry out normal tasks
affects ability to have satisfying relationships
Around 1 in 4 young people will have had depression by the time they become adults.
(Reference: Mind Factsheet: Children, Young People and Mental Health. How common are
mental health problems in young people?)
What is anxiety?
Anxiety is a normal response to challenging events. It can vary from mild unease to a terrifying
panic attack. Problematic anxiety differs from normal anxiety by:
being more severe
longer-lasting
interfering with a person's life and relationships.
What is self harm?
Self harm is any form of deliberate self injury. It is:
a behaviour not an illness
helps to relieve feelings of distress
on the increase
not a failed suicide attempt
a survival strategy.
One in ten people aged 15 and 16 in the UK has self harmed at some point in their life. UK rates
are among the highest in Europe at 400 per 100,000 per year.
Mental Health Foundation (2006) Truth hurts: report of the National Inquiry into self-harm among
young people.
Alcohol and substance use are used by some young people as a way of escaping from
emotional issues and mental health problems. Even irregular and relatively small amounts of
alcohol and drugs can lead to problems for young people from psychosis to suicide. Alcohol and
substance use also increases possibility of later addiction, as well as risk taking activities
resulting in:
physical injuries
aggression and antisocial behaviour
sexual risk taking and unwanted sexual contact
becoming a victim of crime
suicide or self injury.
44% of 13 year olds and 77% of 15 year olds have had an alcoholic drink.
21% of 15 year olds and 5% of 13 year olds reported that they had used drugs. (SALSUS 2011)
Although less common the following mental health problems still need to be permanently on the
radar of the mental health first aider for young people. These are:
suicide
eating disorders
There are a number of myths surrounding mental health – try the quiz at the end of this section to
see what you believe may be true or false.
What is an eating disorder? Eating disorders involve a combination of issues including:
distorted body image
low self esteem
anxiety for some control
an expression of issues such as depression or trauma.
An eating disorder is a serious and life threatening illness.
Common eating disorders include:
anorexia nervosa
bulimia nervosa
eating disorder not otherwise – such as binge eating.
Suicide
Anyone can have suicidal thoughts at some time. Triggers include:
negative setbacks – from bereavement to relationships, from bullying to debt
depression – overwhelmed that the future appears hopeless
impulse – a young person may become suicidal very rapidly perhaps in response to a trigger
such as a relationship breaking up or a failure at school.
There is increased risk from alcohol.
According to a study cited in the Samaritans report on young people and suicide, there are an
estimated 24,000 suicide attempts made by 10 to 19 year olds in England and Wales each year,
which amounts to one attempt every 20 minutes.
Eden-Evans, V. (2004) Young People and Suicide, Samaritans.
Severe mental health problems
There is a difference between less common mental health problems such as suicide and eating
disorders as described earlier, and mental health disorders such as psychosis and bipolar
disorder which you are far less likely to encounter as a mental health first aider working with
young people. This section briefly introduces two such disorders.
Psychosis
Though psychosis related to schizophrenia is rare in young people there are cases in which
children exhibit signs early on. Symptoms include a fear of other people, difficulty distinguishing
reality from fantasy, hearing voices and delusions and generally sufferers will perceive the world
quite differently from others and are withdrawn and often show little of emotion.
Psychosis can occur however as a result of substance use, trauma, eating disorders.
Bipolar
Bipolar disorder sometimes known as manic depression is an illness with abnormal mood swings
of periods of extreme highs and euphoria often followed by deep lows and unhappiness.
DIAGNOSIS AND TREATMENT
Professionals who can help
It is not your role to diagnose a mental health problem, or to understand specialist treatment, but
to help a young person find appropriate professional support. Often the first call will be to the GP.
They will help directly, or refer on if a mental health specialist is necessary.
Young people will generally get better more quickly if they receive appropriate professional help.
Unfortunately young people suffering from mental health problems do not often call on
professional support. They are, however, much more likely to do so if an adult suggests it.
Professionals who can help include:
GPs
School counsellor/guidance/pastoral care and counsellors
Educational psychologists
Clinical psychologists, including family therapy and Cognitive Behavioural Therapists (CBT)
Child and adolescent psychotherapists
Psychiatrists
Allied health professionals
Community psychiatric nurses (CPNs)
Breathing Space
Offering a confidential helpline. Tel: 0800 83 85 87
ChildLine
Offering help and advice about a wide range of issues, talk to a counsellor online, send an email
or post on the message boards. Tel: 0800 1111
Samaritans
Providing confidential emotional support 24/7.
Tel: 0845 790 9090
Types of treatment
There are a range of treatment options depending on the specific problem. For the most part,
treatment will be through a talking therapy, or a combination of talking and other therapeutic
approaches such as art therapy, play therapy, and behavioural focused work such as cognitive
behavioural therapy. It is not usual for medication to be prescribed for more common mental
health problems, such as depression or anxiety, for this age group.
Cognitive behavioural therapy is one of the evidence-based treatment options, which is often
recommended by GPs, and provided by the NHS.
For more information on a variey of treatment options see this resource below from the Royal
College of Psychiatrists.
http://www.rcpsych.ac.uk/mentalhealthinfoforall/moreinformation/definitions/typesoftherapyandt
reatment.aspx
What is CBT?
CBT is a way of talking about:
how you think about yourself, the world and other people
how what you do affects your thoughts and feelings.
CBT can help you to change how you think ('Cognitive') and what you do ('Behaviour'). Unlike
some of the other talking treatments, it focuses on the 'here and now' problems and difficulties.
Instead of focusing on the causes of your distress or symptoms in the past, it looks for ways to
improve your state of mind now.
CBT has been shown to help with: anxiety, depression, panic, phobias (including agoraphobia
and social phobia), stress, bulimia, obsessive compulsive disorder, post-traumatic stress
disorder, bipolar disorder and psychosis. CBT may also help if you have difficulties with anger or
low self esteem.
LEGAL ASPECTS
Framework for child protection
There are fundamental principles which underpin approaches to child protection in Scotland. The
core principles are included in:
United Nations Convention on the Rights of the Child (www.unicef.org/crc/)
GIRFEC (as we have seen in the introduction)
Protecting children and young people: Framework for Standards and the Children's Charter
When confidentiality needs to be broken
"Where there is a disclosure of abuse or suicide plan or plans to harm self or others, Counsellors
have a duty of care to the client and others and need to take appropriate action."
Geldard, K. et al, Counselling Adolescents, Sage 2004
This statement includes the duty of care of the mental health first aider. There may be protocols
in your place of work that make it clear who you should inform if you are concerned about a
young person who has been or might be at risk.
It is important that you are always honest with the young person and involve them in any course
of action you take.
It would be particularly useful to familiarise yourself with the Framework for Standards
and Children's Charter, which sets out a list of demands that children have a right to make. The
Framework for Standards is the detailed means for translating the commitments made in the
Children's Charter into practice.
The Children's Charter sets out a list of demands that children should feel entitled to make:
get to know us
take us seriously
speak with us
listen to us
involve us
respect our privacy
use your power to make things happen when they
be responsible to us
help
should
put us in touch with the think about our
think carefully about how you
right people
lives as a whole
use information about us
help us be safe
The Charter reflects children and young people's own views regarding what they need and the
standard of care they expect when they have problems or are in difficulty and need to be
protected. It shows that children and young people place more value on relationships and
attitudes than processes and events. This should be reflected in the planning and implementation
of all child-focused interventions.
Three pieces of key legislation include:
The Children's (Scotland) Act 1995
The Data Protection Act 1998
The Age of Legal Capacity (Scotland) Act 1991
The Children's (Scotland) Act 1995
This is the main piece of legislation relevant to the protection of children in Scotland it stresses
that: the welfare of the child is the paramount consideration and that the child's views, taking
appropriate account of age and understanding, should be taken into account where major
decisions are to be made about his or her future.
The Data Protection Act 1998
All those involved with children are likely to hold personal information about them, including
sensitive personal information. The Act requires that data is gathered and processed fairly, is
held securely and is used solely for the purpose for which it was collated.
The Age of Legal Capacity (Scotland) Act 1991
Children under 16 do not normally have legal capacity but this Act identifies the circumstances in
which children can act in a way that is legally competent. The Act specifies when children and
young people can consent to medical treatment or instruct a solicitor.