Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
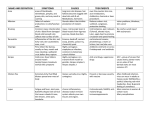
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES BANGALORE, KARANATAKA. PROFORMA FOR REGISTRATION OF SUBJECT FOR DISSERTATION 1. NAME OF THE CANDITATE AND ADDRESS : MR BASKARAN.N, First year M.Sc Nursing, Mysore road kambipura, Bangalore. 2. NAME OF THE INSTITUTION : Rajarajeswari College of Nursing 3. COURSE OF STUDY & SUBJECT : 1st year Ms.c Nursing 4. DATE OF ADMISSION : 31-10-09 5. TITLE OF THE TOPIC : A COMPARATIVE STUDY TO DETERMINE THE EFFECTIVENESS OF CONTINUOUS VERSUS INTERMITTENT PHOTOTHERAPY IN REDUCTION OF LEVEL OF BILURUBIN AMONG BABIES WITH HYPERBILURUMINIEA IN SELECTED HOSPITAL AT BANGALORE. 6. BRIEF RESUME OF INTEND WORK INTRODUCTION Phototherapy is safe and effective in neonatal hyperbilirubinemia. Despite its worldwide application, specific questions regarding methods of optimizing efficacy remain unanswered. Turning the infant is believed to increase the efficacy of phototherapy and this practice was routinely used in approximately half of neonatal departments in a recent survey. some degree of jaundice or hyperbilirubinemia occurs in most newborns. Severe neonatal hyperbilirubinemia is associated with kernicterus, a rare condition characterized by athetoid spasticity, gaze and visual abnormalities, and sensory-neural hearing loss in survivors. It may also be associated with mental retardation1. A 2003 review concluded that kernicterus has a mortality of at least 10% and a morbidity of at least 70%.The true incidence of kernicterus is unknown because it is not a mandatory reportable disease. However, a 2001 Joint Commission Sentinel Event Alert stated that cases of kernicterus have continued to be reported in recent years. Efforts have been made by clinicians and investigators to eliminate this rare disease by instituting system-level measures to screen for hyperbilirubinemia and prevent the occurrence of kernicterus.3–5 Most notable among these is a set of clinical practice guideline concerning the management of hyperbilirubinemia in infants of at least 35 weeks gestation published by the American Academy of Pediatrics2. The 2004 guideline emphasizes the attention to risk factors associated with hyperbilirubinemia, close follow-up of at-risk infants, and the use of phototherapy and exchange transfusion to decrease the level of hyperbilirubinemia as appropriate. Bilirubin and its photo isomers in the biological fluids of a hyperbilirubinaemic newborn infant before and during phototherapy were analyzed by a recently improved HPLC method. In the serum, the percentages of and bilirubin in the total bilirubin concentration before phototherapy were approximately 10% and on average increased over 1.5-fold at 2 hrs after initiation of phototherapy3. The percentage of the (Ecyclobilirubin in the serum bilirubin was under 1 %. In the bile, the mean concentration of bilirubin, derived mainly from bilirubin, nearly tripled during phototherapy. The Ecyclobilirubin concentration in the bile was very low before phototherapy, increased nearly tenfold at 3 h after initiation of phototherapy, and was 5- to 6-fold as high as that of bilirubin. In the urine, upon exposure to light, the urinary concentration of Ecyclobilirubin is apparently equivalent to half of the biliary concentration of bilirubin and one-fifth of that of Ecyclobilirubin. It was concluded that during phototherapy of neonatal hyperbilirubinaemia the structural photo isomer Ecyclobilirubin predominates considerably over the geometric photo isomer Phototherapy has emerged as the most widely form of therapy for the treatment and prophylaxis of neonatal unconjugated hyperbilirubinemia4. Original article maturity, presence or absence of hemolysis, or degree of skin pigmentation phototherapy appears to be safe given the decades of experience with its use in the United States and Europe and the lack of reported serious long-term side effects of short term phototherapy thus far The initial report from the Collaborative Study on the Effectiveness and Safety of Phototherapy, undertaken under the auspices of the National Institute of Child Health and Human Development, demonstrated that infants receiving phototherapy require significantly fewer exchange transfusions. Furthermore, subsequent follow-up studies revealed no adverse outcome in the neonates who received phototherapy in the neonatal period Phototherapy can be used either as therapy or as prophylaxis. Two different mechanisms have been proposed to explain the action of phototherapy in reducing serum bilirubin concentrations in newborn infants; photoisomerization and photo oxidation. Compared with the photoisomerization pathway, the oxidation mechanism appears to play a very minor role in photo catabolism of unconjugated bilirubin in vivo Clinical studies comparing intermittent to continuous phototherapy have yielded conflicting results.5 6.1 NEED FOR STUDY: Signs of Neonatal Jaundice are seen within the first three days of birth in 80% of preterm babies and 60% of full-term infants. The Journal of pediatrics reports a retrospective study, which observed that the incidence of Jaundice is higher in breast- fed babies than in the formula- fed ones. Asian male babies and Native American ones are reported to be most affected by Neonatal Jaundice. They are followed by Caucasian infants who in turn are followed by African Neonates. Babies who are either small or large for gestational age are at an increased risk of developing Neonatal Jaundice. Large for gestational age babies are seen in mothers with diabetes6 Physiological jaundice is the most common type and effects over 50% of babies. Due to an immature liver, bilirubin is processed slower. This type of jaundice appears at 2 to 3 days of age and commonly disappears by 1 to 2 weeks of age. Bilirubin levels are not harmful with this type of jaundice. Jaundice becomes detectable to the naked eye when the total serum bilirubin level exceeds about 85μmo (5 mg/100ml) and most babies become visibly jaundiced in the first week of life. Unfortunately the terminology used in many texts Talks of jaundice being ‘moderate’ when it exceeds 200μmo and ‘severe’ when it exceeds 250μmo on any such definition ‘severe’ jaundice develops in a third of all breast fed babies in the first week of life! Such lax use of language undoubtedly triggers a lot of unnecessary investigation7. Jaundice is only really ‘actionable’ in the otherwise healthy term baby when the level exceeds 340μmo (20 mg/100ml) and potentially dangerous when it exceeds 43μmo (25 mg/100ml). Phototherapy would not need to be given so often if it were administered more effectively when given. The graph shown here documents how the bilirubin level varied over time in a large group of mature exclusively breast fed babies – most other ‘normative’ charts document the levels seen in a population where at least a third of the babies were bottle fed. the investigator investigate the prevalence the rate of hyperbilirubinemia is high. The phototherapy play significant role in reduction of bilurubin in babies with hyperbilirubinemia. So the researcher has the interest to determine the effectiveness between continuous and intermittent phototherapy to find the rapid recovery from hyperbilirubinemia8. 6.2 REVIEW OF LITERATURE: “A study was conducted on effectiveness of intermittent versus continuous phototherapy in reduction of level of bilirubin among babies with hyperbilirubinemia” at Iran the objective of this study was to assess effect of phototherapy with babies complication the study was performed on 114 babies with hyperbilirubinemia. The result concluded that phototherapy cycle of one hour on and one hour off is as effective as continuous phototherapy in treatment of hyperbilirubinemia9 The study was conducted on “Serum bilirubin kinetics in intermittent phototherapy of physiological jaundice” at Japan with the objectives of to treat the babies in the easiest way to minimize hospital duration Thirty four term babies with physiological jaundice were subjected to continuous phototherapy and to two regimens of intermittent phototherapy. The difference in serum bilirubin kinetics between the three groups of treated babies was insignificant; a schedule of one in four hours of irradiation achieved the same treatment effect as continuous phototherapy10. The study was conducted on Regardless of different protocols of phototherapy, the Number-Needed-to-Treat (NNT) for prevention of serum bilirubin level exceeding 20 mg/dL ranged from six to 10 in infants of at least 34 weeks gestation at America This implies that one needs to treat six to 10 jaundiced neonates with TSB ≥ 15 mg/dL by phototherapy in order to prevent the TSB in one infant from rising above 20 mg/dL. Phototherapy combined with cessation of breastfeeding and substitution with formula was the most efficient treatment protocol for infants of at least 34 weeks gestation with jaundice. Eight studies examined the effect of bilirubin reduction on brainstem auditory evoked response (BAER). All consistently showed treatments for neonatal hyperbilirubinemia significantly improved abnormal BAER’s in both healthy jaundiced infants and jaundiced infants with hemolytic disease Three studies evaluated the effect of phototherapy on visual outcomes. All showed no short- or long-term (up to 36 months) effect on vision as a result of phototherapy when infants’ eyes were properly protected during treatment11. A research was conducted on “bilurubin included cell death during continuous and intermittent phototherapy and in the dark “at Norway the study objectives is to assess the duration of intermittent vs. continuous phototherapy, and to assess the bilurubin level during the treatment I.e. cell death the researchers compared continuous and intermittent light exposure in the presence of bilurubin with respect the cellular damage. The result showed that continuous and intermittent light exposure caused the same degree of apoptotic cell death while the cells underwent more necrotic death after intermittent exposure12. A research was conducted on “To look for the effect of position changing on bilurubin level during the continuous and intermittent phototherapy” at Israel the study objective was to assess the phototherapy with changing position and effect of continuous and intermittent phototherapy They conducted the pilot study in term infants requiring phototherapy in order to determine the time required to clear the skin of bilurubin. Balancing time was 150 minutes. They conducted a randomized study complaining turning the baby in supine position only. They conducted that infants should be nursed supine during phototherapy infants in the supine group showed a significally larger drop in serum total bilurubin concentration and required shorter duration of phototherapy13 A study was conducted to determine the incidence of post-phototherapy neonatal plasma total bilurubin rebound at England a prospective clinical survey was performed on 226 and neonates treated with phototherapy, neonates were tested for PTB 24 hours after discontinuation of phototherapy a total of 30 neonates developed significant rebound they conducted that post phototherapy neonates bilurubin rebound to clinically significant levels may occur especially in cases of prematurity14. “A study was conducted on effectiveness of phototherapy treatment” they describe in a very simple way that staff can assess the effectiveness of the treatment they concluded that the effectiveness is greatly influenced by how for they are position from the child and can be almost doubled by the cot which could be easily accesse by the staffs15 STATEMENT OF THE PROBLEM “A comparative study to determine the effectiveness of Continuous vs. Intermittent Phototherapy in reduction of level of bilurubin among babies with hyperbiluruminiea selected hospital at Bangalore”. 6.3 OBJECTIVES OF THE STUDY 1. To determine the effectiveness of continuous phototherapy of babies with hyperbilirubinemia in group-I 2. To determine the effectiveness of intermittent phototherapy of babies with hyperbilirubinemia in group-I 3. To compare the effectiveness of intermittent and continuous phototherapy in reduction of Bilurubin level 4. To find association between effectiveness of continuous phototherapy and demographic variables of babies 5. To find association between effectiveness of intermittent phototherapy and demographic variables of babies HYPOTHESES H1-There is a significant difference between mean post assessment score of continuous phototherapy and mean post assessment of intermittent phototherapy in reduction of level of Bilurubin. H2- There is a significant association between the post test score of continuous vs. intermittent phototherapy in reduction of Bilurubin level among babies with hyperbilirubinemia with their selected demographic variables 6.3.1. ASSUMPTIONS 1. Intermittent phototherapy as effective as continuous phototherapy 2. Babies with hyperbilirubinemia may prone to develop complications 6.3.2 VARIABLES (a)Dependent Reduction in level of Bilurubin (b)Independent Continuous and intermittent phototherapy 6.3.3 OPERATIONAL DEFINITIONS Comparative study It refers to the basis of analytic epidemiology the statistical comparison between groups. Bilurubin It refers to the orange pigmentation of bile formed primarily by the breakdown of hemoglobin in red blood cells after termination of their lifespan Hyperbilirubinemia It refers to the increased Bilurubin level in the blood Intermittent phototherapy It refers to the phototherapy is given to babies with hyperbiluruminiea that as to be given alternatively by each one hour on and 4hours off. Continuous phototherapy It refers to the phototherapy is given to babies with hyperbiluruminiea that as to be given continuously by each 15minutes on and 30 minutes off. 7. MATERIALS AND METHODS 7.1 Source of data New born babies who are admitted in NICU with phototherapy, who will meet the inclusive criteria 7.2 Method of collection of data 7.2.1 Definition of the study subject New born babies who are admitted in NICU with phototherapy who will meet the inclusive criteria 7.2.2 Inclusion and Exclusion Criteria a) Inclusion Criteria 1. Babies who have hyperbiluruminiea 2. Babies weight above 2000gm 3. Babies gestational age above 32 weeks b) Exclusion criteria 1. Babies who are having congenital abnormalities 2. Mothers those who are not willing 7.2.3 Research Approach: Quantitative approach 7.2.4 Research Design True experimental study 7.2.5 Setting The study will be conducted in selected hospital, Bangalore 7.2.6 Sampling technique Random sampling technique 7.2.7 A) Sample size 30- New born babies who are admitted in NICU with phototherapy who will meet the inclusive criteria b) Duration of the study 4 weeks 7.2.8 Tools of Research PART I: Socio demographic data Part II Bilurubin assessment scale 1. Normal level - Below 5mg/dl 2. Mild jaundice - 5 to 10 mg/dl 3. Moderate jaundice - 10 to 15 mg/dl 4. Severe jaundice - Above 15mg/dl CRAMER’S DERMAL ZONES INDEX OF NEONATAL JAUNDICE: Zone I face : 5mg/dl Zone II chest and upper abdomen : 10mg/dl Zone III thighs and upper arms : 12mg/dl Zone IV legs and forearm : 15mg/dl Zone V palms and soles : 15mg/dl 7.2.9 Collection of data The investigator collects the data by using bilurubin assessment scale. The sample will be collected by randomly, even no’s of the sample denotes the group-I and odd no’s of sample ,s denotes the group-II Before placing the sample in to the phototherapy bilurubin level will be checked and classified based on the bilurubin assessment scale .the researcher check the bilurubin level every 12 hours for 2 days during phototherapy. After 48 hours of phototherapy the bilurubin level will be checked, classified and compare with each group to know the effectiveness based on bilurubin assessment scale. 7.2.10 Method of Data Analysis And presentation 1. The investigator will use descriptive statistics such as mean, median, and standard deviation and inferential statistics like “t” test and chi-square test will be used. 2. The analyzed data will presented in the form of tables, diagram and graph 7.3 Does the study require any investigation to be conducted patients or other human or animals? If so describe briefly? Yes with prior consent from samples the study will be conducted on children with hyperbiluruminiea regarding phototherapy to reduce the Bilurubin level in selected hospital at Bangalore 7.4 Has ethical clearance has been obtained from your institution in case of? Yes permission will be obtained from the concerned person and authority of the institution before the study privacy, confidentiality and anonymity will be guarded scientific objective of the study will be maintained with honesty and impartiality. 8. LIST OF REFERENCES 1) Maisels MJ. Jaundice Neonatology: Pathology and Management of the Newborn, 6th edition JB Lippincott, 2008 Philadelphia. 2) Ronald RJ, De Sandre GH, Sibley Neonatal jaundice and liver disease Neonatal-Perinatal Medicine Diseases of the fetus and infant 8th edition Philadelphia, Mosby. 3) Scheidt PC, Bryla DA, Phototherapy for neonatal hyperbilirubinemia six year follow-up of NICHD clinical trial 2007. 4) S Chung M, Kulig J, An evidence based review of important issues concerning neonatal 2nd edition 2004 hyperbilirubinemia. 5) Forfar & anneil’s text book of peadiatrics 6th edition Lippincott 6) Brown AK, Kim MH, Efficacy of phototherapy in prevention and management of neonatal hyperbilirubinemia UK 2002. 7) Rubaltelli FF, Zanardo V, Granati B.Effect of various phototherapy regimens on bilirubin decrement Pediatrics 1978 8) Maisels MJ. Phototherapy Maisels MJ, Watchko JF edition Neonatal Jaundice New York Hardwar academic Publishers. 9) Shane Watchko JF Neonatal Jaundice Phototherapy New York. Hardwar Academic Publishers. 10) Pedram niknaf abdol Jaundice Neonatology: Pathology and Management of the Newborn. 6th edition JB Lippincott. Philadelphia 11) Sp Lau KP fung Neonatal jaundice and liver disease. In Neonatal-Perinatal Medicine: Diseases of the fetus and Infant.8th edition Philadelphia 12) American Academy of Pediatrics Clinical Practice Guideline. Management of hyperbilirubinemia in the newborn Infant 35 or more weeks of gestation. Subcommittee on Hyperbilirubinemia. 13) Ellen harmazol Phototherapy for neonatal hyperbilirubinemia: Six year follow-up of clinical trial 2nd edition UK 14) E shine well M.D Phototherapy for neonatal jaundice.3rd edition England 15) Verman statement of phototherapy using in position 2nd edition 2008 Websites: www.pubmed.com www.childspo.com www.baby.com www.scird.com www.medspace.com NICHD Signature of the candidate NAME AND DESIGNATION OF GUIDE : Ms MAHALAKHSMI M.Sc (N), HOD, PEADIATRIC NURSING, RAJARAJESWARI COLLEGE OF NURSING, BANGALORE. SIGNATURE : (Remarks of the guide) : The present study provide guidelines for nurses to practice effective method of phototherapy CO-GUIDE (IF ANY) : : Ms. PARVATHI M.Sc (N) LECTURER RAJARAJESWARI COLLEGE OF NURSING BANGALORE. SIGNATURE : HEAD OF THE DEPARTMENT : Ms MAHALAKHSMI M.Sc (N), HOD, PEADIATRIC NURSING, RAJARAJESWARI COLLEGE OF NURSING, BANGALORE Signature : Remarks of the principal : The topic selected for study is relevant and forwarded for needful action Signature : ETHICAL COMMITTEE CLEARANCE 1. Title of the Dissertation : A comparative study to determine the effectiveness of continuous vs. intermittent Phototherapy in reduction of level of Bilurubin among babies with hyperbilirubinaemia in selected hospital at Bangalore. 2. Name of the Candidate : Mr.Baskaran.N 3. Subject : M.Sc Nursing Child Health Nursing 4. Name of the Guide 5. Approved/Not Approved : MIS. MAHALAKSHMI.MSC NURSING : (If not approved suggestions) Head of the department of Head of the department of Pediatric Nursing Medical Surgical Nursing Rajarajeswari College of Nursing Rajarajeswari College of Nursing Bangalore. Bangalore. Head of the department of Head of the department of OBG Nursing Psychiatric nursing Rajarajeswari College of Nursing Rajarajeswari College of Nursing Bangalore. Bangalore. Head of the department of community Rajarajeswari College of Nursing Bangalore. Principal Rajarajeswari College of Nursing Bangalore