Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
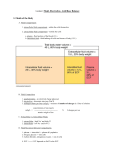
Physiology 31 Lecture Chapter 20 – Fluid & Electrolyte Balance I. Overview A. Cellular function requires a fluid medium with a homeostatic balance of the following 1. Water, in which daily water intake and loss are equal 2. Electrolytes, in which the amount of electrolytes absorbed by the small intestine balance the amount lost from the body, mainly through the urine 3. Acid-base, in which the body rids itself of acid (H+ ions) at a rate that balances its metabolic production, maintaining a stable pH B. These balances are maintained by the all of the bodily systems, except for the reproductive system II. Water Balance & the regulation of ECF Volume A. The average person’s body is about 50-60% water B. Compartments in which water is found include 1. 65% in intracellular fluid (ICF) within cells 2. 35% in extracellular fluid (ECF), which includes a. 25% interstitial fluid around cells b. 8% blood plasma and lymph c. 2% transcellular fluid, such as cerebrospinal, synovial, serous, vitreous & aqueous humors, bile, and fluids in the GI, urinary, and respiratory tracts C. Water moves by osmosis from one compartment to another, so the ECF and ICF osmolarities rarely differ D. A person is in a state of water balance when daily water intake and losses are equal 1. Water gains come mainly from ingested water, in addition to a small amount of water from cellular respiration 2. Water is lost mainly in urine, as well as from feces, expired breath, and sweat through the skin 3. Diarrhea can cause a significant water loss 4. Intravenous (IV) fluids may be needed to replace water loss 2 E. Fluid intake is regulated by the thirst center in the hypothalamus 1. The hypothalamus responds to signs of dehydration, such as a. Angiotensin II, produced in response to falling blood pressure b. Decreased atrial stretch, due to low blood volume c. Signals from osmoreceptor neurons in the hypothalamus that monitor blood osmolarity d. ADH (vassopressin), is synthesized and released in response to rising blood osmolarity e. ADH stimulates water reabsorption from kidney tubules 2. Thirst is stimulated and satiated by a. The thirst center sends sympathetic signals to the salivary glands to inhibit salivation b. Short term satiation of thirst is accomplished by cooling and moistening the mouth and inflating the stomach b. Long term satiation of thirst depends on absorbing water from the small intestine and lowering blood osmolarity F. Fluid output and retention is regulated by factors that control urine output 1. ADH is secreted by the posterior pituitary gland in response to dehydration, which causes the kidneys to reabsorb water. ADH release is inhibited if a. Blood volume or pressure are too high, or b. Blood osmolarity is too low 2. Aldosterone, released by the adrenal cortex, causes sodium (and water) to be reabsorbed from the kidneys. Adosterone secretion is influenced by a. Increased plasma K+ concentration causes aldosterone release; results in K+ secretion from the blood to the kidney tubules (prevents hyperkalemia) b. Angiotensin II, formed in response to renin release when BP is low, causes secretion of aldosterone c. Increased ECF osmolarity inhibits aldosterone secretion, thus more Na+ is excreted in the urine 3 3. Atrial Naturetic Peptide (ANP), released during high BP, promotes Na+ and water excretion, and inhibits the release of ADH, renin, and aldosterone G. Disorders of Water Balance occur if there is an abnormality of total fluid volume, concentration, or distribution among the compartments 1. Fluid deficiency arises when output exceeds intake over a period of time. Two kinds of fluid deficiency are a. Volume depletion (hypovolemia), in which proportionate amounts of water and sodium are lost; may be due to hemorrhage, burns, vomiting, diarrhea, or hyposecretion of aldosterone b. Dehydration (negative water balance), in which volume is reduced and osmolarity is elevated because the body has lost more water than sodium; caused by lack of drinking water, diabetes mellitus, ADH hyposecretion, profuse sweating c. Severe fluid deficiency can result in circulatory shock and death 2. Fluid excess can occur in two forms a. Volume excess - the retention of excess fluid with normal osmolarity; can result from aldosterone hypersecretion or renal failure b. Hypotonic hydration (water intoxication) – the retention of more water than sodium, reducing osmolarity, as when one loses water and sodium in sweat and drinks plain water; can cause pulmonary and cerebral edema 3. Fluid sequestration – total body water may be normal, but fluid may accumulate in a particular location; occurs in edema, hemorrhage, and pleural effusion where fluids accumulate in the pleural cavity 4 III. Electrolyte Balance A. Electrolyte (ion) functions include 1. Provide enzyme cofactors (e.g., Zn2+, Mg2+) 2. Allow action potentials in neurons and muscles (Na+, K+, Cl-) 3. Stimulate the secretion and action of hormones and neurotransmitters (e.g., Ca2+) 4. Allow muscle contraction (Ca2+) 5. Maintain acid-base balance (H+, HCO3-, and phosphates) 6. Allow secondary active transport across membranes (Na+, K+) 7. Stimulate osmosis across cell membranes B. Major cations include Na+, K+, Ca2+, and H+ C. Major anions are Cl-, HCO3- , phosphates (HPO42- and H2PO4-), and proteins D. Sodium (Na+) is the main cation in the ECF 1. Na+ functions include a. Osmotic and fluid balance b. Nerve and muscle activity c. Cotransport of molecules (e.g., glucose, amino acids) across cell membranes d. Acid-base buffering (NaHCO3) e. Heat generation via the Na+/K+ pump 2. Sodium homeostasis is maintained by a. Aldosterone promotes Na+ reabsorption b. ADH reduces Na+ concentration by promoting water reabsorption independently of Na+ c. Atrial naturietic peptide inhibits Na+ and water reabsorption, lowering blood pressure 3. Imbalances of sodium include a. Hypernatremia is an excess of Na+, which causes water retention, hypertension, and edema b. Hyponatremia is a deficiency of Na+, often a result of hypotonic hydration; salt appetite is stimulated in the hypothalamus 5 E. Potassium (K+) is the major cation in the ICF. It has similar functions as Na+, and is a cofactor for some enzymes 1.Potassium homeostasis is maintained mainly by aldosterone, which promotes excess K+ excretion by the kidneys 2. Imbalances of potassium include a. Hyperkalemia causes serious nerve and muscle dysfunction, and can cause cardiac arrest! 1) If plasma and ECF K+ increases, the concentration gradient decreases, and more K+ remains inside cells, depolarizing them initially 2) Cells are unable to repolarize fully, causing cells to become less excitable b. Hypokalemia inhibits nerve and muscle function 1) Increase in K+ gradient causes more K+ to leave cells, hyperpolarizing them 2) Hyperpolarized cells are more difficult to depolarize to threshold for action potentials F. Chloride (Cl-) is the major anion of the ECF 1. Chloride functions include a. Regulation of osmotic balance (with Na+) b. Formation of stomach acid (HCl) c. The chloride shift mechanism in respiratory and renal function 2. Chloride homeostasis follows Na+ and other cations, and is regulated as a side effect of Na+ homeostasis 3. The primary effect of chloride imbalances is a pH imbalance G. Calcium (Ca2+) has low intracellular concentrations, but is often sequestered in smooth E. R., then released when needed 1. Calcium is necessary for a. Muscle contraction b. Nerve transmission and exocytosis of neurotransmitters c. Blood clotting d. A second messenger for some hormone actions 6 e. Bone and tooth formation 2. Calcium homeostasis is regulated by a. Parathyroid hormone (PTH) – increases serum Ca2+ levels by bone reabsorption and intestinal uptake b. Calcitriol (vit. D) is required for intestinal uptake of Ca2+ c. Calcitonin – decreases serum Ca2+ levels and increases bone deposition 3. Hypercalcemia can result from alkalosis, hyperparathyroidism, or hypothyroidism; causes muscle weakness, depressed reflexes, and cardiac arrhythmia 4. Hypocalcemia can result from acidosis, vit. D deficiency, diarrhea, pregnancy, lactation, hypoparathyroidism, or hyperthyroidism; causes potentially fatal muscle tetany H. Phosphates (PO43-, HPO42-, H2PO4-) are relatively concentrated in the ICF, where they are generated by ATP hydrolysis 1. Phosphate functions include a. Phosphates are a component of nucleic acids, phospholipids, ATP, GTP, cAMP, and related compounds b. Phosphates activate many metabolic pathways by phosphorylating substances such as glucose and enzymes c. Phosphates are important acid-base buffers 2. Phosphate levels are regulated by parathyroid hormone, which increases phosphate excretion and minimizes the formation of CaPO4 3.Phosphate imbalances are not as critical as other electrolyte imbalances 7 IV. Acid-Base Balance A. The pH of the ECF is normally maintained between 7.38-7.42, despite constant production of acidic products (e.g., lactic acid, phosphoric acids, fatty acids, carbonic acid) B. Acids, Bases, & Buffers 1. An acid is any chemical that releases H+ ions in solution a. Strong acids (HCl) give up most of their H+ ions and can lower pH significantly b. Weak acids (H2CO3) do not give up many H+ ions, thus affect pH only slightly 2. A base is any chemical that takes up H+ ions in solution a. Strong bases (-OH) have a strong tendency to bind H+ ions and raise pH b. Weak bases (HCO3-) bind less H+, thus have less of an effect on pH 3. A buffer is any mechanism that resists changes in pH by converting strong acids or bases to weak ones. The body has both physiological and chemical buffers a. Physiological buffers, such as the respiratory and urinary systems, stabilize pH by controlling the body’s output of acids, bases, or CO2 b. Chemical buffers bind H+ and removes it from solution as its concentration begins to rise, or releases H+ into solution as its concentration falls. 4. Three chemical buffer systems in the body are the a. Bicarbonate buffer system, represented by the eqn.: CO2 + H2O H2CO3 HCO3- + H+ (has an optimal pH of 7.4) 1) The lungs and kidneys remove CO2, which keeps the rxn. moving to the left, reducing H+ ions 2) If there is a need to lower pH, the kidneys excrete HCO3-, which moves the rxn. to the right, increasing the H+ concentration 8 b. Phosphate buffer system has an optimal pH of 6.8, and is important for buffering the renal tubules & ICF. The rxn. is H2PO4- HPO42- + H+ c. Protein buffer system accounts for ¾ of all chemical buffering in body fluids, due to side groups of amino acids 1) Carboxylic acid groups (-COOH) release H+ when ph begins to rise 2) Amino groups (-NH2) bind H+ when pH falls too low C. Respiratory control of pH - the respiratory system buffers pH by adjusting pulmonary ventilation 1. Reduced ventilation allows CO2 to accumulate in the blood and lower its pH by the rxn. CO2 + H2O H2CO3 HCO3- + H+ 2. Increased ventilation expels CO2, reversing the above rxn, lowering H+, and raising the pH D. Renal control of pH – the kidneys neutralize more acid or base than any other buffer system in the body 1. They secrete H+ into the tubular fluid, where it binds to chemical buffers and is excreted in the urine 2. The above H+ normally neutralizes all the HCO3- in the tubular fluid, making urine bicarbonate free 3. Excess H+ in the tubular fluid can be buffered by phosphate and ammonia (NH3+) E. Disorders of acid-base balance 1. Acidosis is a pH of 7.35 a. Respiratory acidosis occurs when pulmonary gas exchange is insufficient to expel CO2 as fast as the body produces it b. Metabolic acidosis is the result of lactic acid or ketone accumulation, ingestion of acidic drugs, such as aspirin, or loss of base, as in diarrhea 9 2. Alkalosis is a pH of 7.45 a. Respiratory alkalosis results from hyperventilation b. Metabolic alkalosis is rare, but can be caused by overuse of antacids or loss of stomach acid through vomiting 3. Uncompensated acidosis or alkalosis is a pH imbalance that the body cannot correct on its own; it requires clinical intervention (i.e., fluid replacement therapy) 4. Compensated acidosis or alkalosis is an imbalance that the body’s homeostatic mechanisms can correct a. Respiratory compensation is correction of the pH through changes in pulmonary ventilation b. Renal compensation is correction of pH by changes in H+ secretion by the kidneys 5. Water, electrolyte, and acid-base imbalances are intimately entwined; an imbalance area can cause or result from an imbalance in another