Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
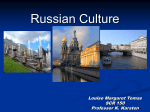
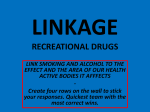
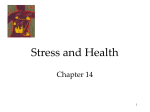
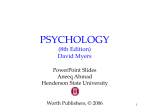
Bedfordshire Public Health Annual Report Report 2 March 2007 Progress in achieving targets linked to improving Life Expectancy D:\478185952.doc 1 1 Introduction As Bedfordshire’s Director of Public Health I have responsibility for the health of the people of Bedfordshire and for delivery of key public health goals, including the reduction of health inequalities. To inform Bedfordshire’s joint work to improve health, each year the Director of Public Health is charged with producing a Public Health Annual Report. In order to produce this report in a more timely and focused manner, I have decided to produce chapters of the report throughout the year. Improving Bedfordshire’s health and reducing health inequalities will require many agencies to working together to: Deliver national strategies which tackle the major issues that impact on health across the whole of England; and Identify issues where Bedfordshire is different from the rest of the England and where local strategies and approaches are required. This first chapter of the Annual Report reviews Bedfordshire’s performance against key national targets relating to improving life expectancy. These targets relate to: Cancer and heart disease / stroke the biggest causes of early deaths. Smoking and obesity the biggest risk factors for poor health. Bedfordshire is making progress against all targets linked to life expectancy, but progress could be better. Our life expectancy remains lower then the Eastern Region average. Achievement against current targets is unlikely to change this. If this is to be achieved more ambitious targets are required. This report recommends that a debate takes place regarding Bedfordshire’s future targets for improving life expectancy. Future reports will consider Bedfordshire’s progress in achieving Local Area Agreement targets and other national health improvement targets to reduce suicides, reduce health inequalities and improve outcomes for people with long-term conditions. The full programme of future public health “annual” reports is in development. I welcome your thoughts on the issues you believe I should consider. Dr Dorothy Gregson Director of Public Health Bedfordshire Acknowledgement – thank you to Helen Knowles, Edmund Tiddeman, Muriel Scott, Debs Richardson and Cass Golmbena D:\478185952.doc 2 2 Life Expectancy The national objective is to increase life expectancy at birth in England from 74.6 to 78.6 years for men and from 79.7 to 82.5 years for women by 2010. If the existing trend starting in 19961 continues, England should achieve a life expectancy of 78.6 years for men and 82.2 years for women. By 2004 (the most recent data available) the life expectancy in Bedfordshire was 77.6 years for men and 81.5 years for women; increases of 2.8% for men and 1.6% for women on the baseline. These trends are in line with those for England. Figure 1 Life expectancy trends in Bedfordshire 84 Bedfordshire females slope 0.179 East of England females slope 0.141 England females slope 0.164 82 Life expectancy at birth 80 78 76 East of England males slope 0.226 Bedfordshire males slope 0.244 England males slope 0.262 74 72 70 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 Bedfordshire males Bedfordshire females East of England males East of England females England males England females On average people in Bedfordshire live longer then men and women in England. However, our life expectancy is not better then Eastern Region. Life expectancy in men has not improved as fast as the rest of the region and so is now significantly below the Regional average. This is despite the fact that Bedfordshire experiences less deprivation then Eastern Region as a whole. It appears more can be achieved. 1 these are actually based on 3 year averages for 1995-1997 and 2009-2011. D:\478185952.doc 3 2.1 Causes of Early Deaths Life expectancy is closely related to all age, all-cause mortality, which is easier to measure, and more easily broken down into components to allow the contribution of different diseases to be identified. If we want to improve life expectancy then it is important to know what causes people to die early. This can be measured in terms of Years of Life Lost2 (YLL) which takes into account the age at death and assumes that a death before the age of 75 is premature. The biggest causes of early deaths (deaths of people aged under 75) in Bedfordshire are cancer and heart disease / stroke, accidents and suicide, see Figure 2. This pattern is in line with the national picture. Figure 2 Main causes of reduced life expectancy in Bedfordshire Years of life lost under 75 years, 2001-03 (pooled) Liver disease, 3.2% Chronic breathing diseases and pneumonia, 4.0% suicide and injury undetermined, 5.6% all cancers, 33.8% accidents, 9.4% all other causes, 19.4% all circulatory diseases, 24.6% The total number of years lost as result of people dieing under the age of 75 years in Bedfordshire was on average 15,995 per year between 2003 and 2005 . The major causes of these early deaths were cancer and circulatory disease see Table 1. 2 D:\478185952.doc 4 Table 1: Years of life lost for people of Bedfordshire All causes, males All causes, females Total all causes, male and female Cause of early death All cancers All circulatory diseases All other causes Accidents Suicide and injury undetermined Chronic breathing diseases and pneumonia Liver disease Total Average number of years of life lost (YLL) per year (2003 to 2005) 9,998 5997 15,995 Percent of total Average number of YLL per year (2003 to 2005) 5,411 3,942 3,096 1,499 894 Percent of total 33.8% 24.6% 19.4% 9.4% 5.6% 647 4.0% 505 15,995 3.2% 100.0% 62.5% 37.5% 2.2 National targets linked to life expectancy Public Service Agreements (PSAs) set out the key improvements that the public can expect from Government expenditure. They are three year agreements, negotiated between each of the main Departments and HM Treasury during the Spending Review process. Each PSA sets out a Department's high-level aim, priority objectives and key outcome-based performance targets. The Department of Health PSAs have a high priority within the NHS. National Public Service Agreement targets have been set to reduce deaths from cancer and cardiovascular disease, the biggest contributors to years of life lost. The targets are: PSA 01a - Substantially reduce mortality rates by 2010 from heart disease and stroke and related diseases by at least 40% in people under 75, with at least a 40% reduction in the inequalities gap between the fifth of areas with the worst health and deprivation indicators and the population as a whole; PSA 03a - Substantially reduce mortality rates by 2010 from cancer by at least 20% in people under 75, with a reduction in the inequalities gap of at least 6% between the fifth of areas with the worst health and deprivation indicators and the population as a whole; These targets expire in 2010. New targets will soon be required. The following sections focus on the local performance against the PSA targets for reducing rates of cardiovascular disease and cancer. Aspects relating to inequalities will be considered in future reports. This report seeks to stimulate a debate regarding how ambitious we should be with respect to future targets to improve life expectancy. D:\478185952.doc 5 3 Cardiovascular disease mortality Cardiovascular disease is the second leading cause of death for people in Bedfordshire accounting for around 1220 deaths per year. With 330 of these occurring in people aged under 75 years it is the second largest cause of premature death. This equates to 3,900 years of life lost per year. The total of 1220 deaths are split fairly equally between men and women but in those under 75 deaths, 220 (2/3 rd) are men, and 110 (1/3 rd) are women. Figure 3 shows the decline in mortality over recent years. This has been measured in terms of the directly age-standardised rate (DSR). This technique allows death rates in populations with different age structures to be compared. Figure 3 160 Mortality rate from all circulatory diseases for persons age less than 75 years, trend 1996 to 2004, projection to 2008 DSR per 100,000 persons, 3 year average 140 120 100 80 60 40 20 0 1994 1996 1998 ENGLAND 2000 2002 EAST OF ENGLAND 2004 Bedfordshire PCT 2006 2008 Target Progress has been in line with national trends and is on track to meet the overall target. The fall in cardiovascular mortality has been attributed to improvements in treatments (<50%) and to risk factor changes (>50%). National trends in mortality have been declining since a peak in the 1970s. It has been suggested (Critchely, Capewell 2003) that the national target is not challenging and there is potential to reduce mortality further with modest progress on reducing risk factor in line with what has been achieved in other countries. D:\478185952.doc 6 2010 Local programme budgeting information indicates that at present £41,000,000 is spent on CVD. This is approximately 10% of Bedfordshire PCT’s overall budget. 3.1 Actions to reduce cardiovascular mortality. There are a number of factors that contribute to cardiovascular disease (CVD). Modifiable risk factors (i.e. ones that can be improved) include: smoking, physical inactivity, obesity and poor nutrition. High alcohol increases cardiovascular disease but not coronary heart disease. Figure 4 illustrates how these risk factors link. Cardiovascular disease is common and exists both with and without symptoms of disease. Both the risk factors and the disease are more common in deprived and disadvantaged groups. Future public health report will address inequalities and inequity. Figure 4: How modifiable risk factors in cardiovascular disease link together CVD mortality TIA/ PVD/ other CHD Stroke CVD risk Hypertension High cholesterol Diabetes Obesity Smoking Physical Inactivity Poor Nutrition High Alcohol TIA – transient ischaemic attack, PVD peripheral vacular disease Improving cardiovascular mortality depends on ensuring: Good access to effective and timely treatment for people with cardiovascular disease. Effective assessment and management of people at risk of cardiovascular disease. Progress in reducing risk factors in the population as a whole. Smoking and obesity are considered in section 5 and section 6. D:\478185952.doc 7 PSAs are in place for measuring risk factors associated with cardiovascular disease. Also access to treatment is closely monitored. 3.2 Access to effective and timely treatment- -Thrombolysis When someone has a Myocardial Infarction (MI or heart attack) early treatment with clot busting drugs, thrombolysis treatment, can improve their outcome. Targets have been set to for: the time from the person calling for help and receiving the treatment (call to needle times). the time from a person reaching the hospital and receiving treatment (door to needle times). Table 2: Access to thrombolysis Bedford Hospital 2004/05 2005/06 Eligible patients to receive thrombolysis within 30 minutes of arrival in the hospital (door to needle time) Target 75% 88% Eligible patients to receive thrombolysis within 60 minutes of calling for help (call to needle) Target 68% 56% Luton and Dunstable Hospital Eligible patients to receive thrombolysis within 30 minutes of arrival in the hospital (door to needle time) Target 75% Eligible patients to receive thrombolysis within 60 minutes of calling for help (call to needle) Target 68% 88% Q1 06/07 94.10% Q2 06/07 80% 42% 16/17 62.50% 12/15 71.40% 10/16 10/14 75% 68% 54% 47% The call to needle times are challenging for rural areas where the time taken for emergency ambulances to reach hospitals are significant. The cardiac network is exploring alternative approaches. 3.3 Assessment and management of people at risk of cardiovascular disease 3.3.1 Practice Based Registers There are two main approaches to prevention of cardiovascular disease (CVD). The high risk approach, where the aim is to identify people without symptoms of cardiovascular disease with an absolute risk of CVD events greater than 20% over the next 10 years, i.e. they have at least a one in five chance of having a CVD event such as stroke or Myocardial infarction in the next 10 years. D:\478185952.doc 8 Population approach, where the aim is to reduce the level of risk for the whole population, e.g. reducing the average level of serum cholesterol or blood pressure for a population. This will occur if everyone chooses to lead a healthier life. The PSA targets for cardiovascular disease reflect the high risk approach whereby those at highest risk are identified: PSA01b - Number of GP practices with PCT validated registers of patients without symptoms of cardiovascular disease but who have an absolute risk of CVD events greater than 20% over the next 10 years Practice based disease registers enable the systematic proactive management of people with chronic conditions such as diabetes, hypertension, coronary heart disease and stroke. Table 3 sets out the number of people identified and placed on GP registers with a range of risk factors. It also presents the numbers predicted using national prevalence models based on population age and ethnicity structure. Table 3: Expected number of people and recorded number of people on GP registers for Hypertension, coronary heart disease, cardiovascular disease, diabetes, smoking and obesity Number of people predicted in Bedfordshire PCT’s population CHD 15,00 Diabetes 17,000 Obesity 83,000 Overweight and 211,000 Obesity Hypertension 99,000 Smoking 84,000 CVD risk >20% 9,000 women, 28,000 men Source QMAS January 2007 Actual number of people recorded on GP practice registers within Bedfordshire PCT 13,000 15,000 30,000 Not available 46,000 12,000 Not available The main rationale in identifying people at high risk of disease is to help them reduce their risk through lifestyle changes and pharmacological management. This approach has the advantages that advice and support can be offered on an individual tailored basis. Disease registers direct resources to those most in need and most likely to benefit. The Strategic Health Authority has set the PCT a target of 75% of our practices having PCT validated registers of patients without symptoms of cardiovascular disease but who have an absolute risk of CVD events greater than 20% over the next 10 years. This will be challenging. This high risk approach to preventing CVD is not without its problems. These include the fact that the level of an individual’s risk is a continuum, not dichotomous. Any cut off point to distinguish high risk people from the low risk people is an artificial one. On a practical level this will mean that someone assessed as having a cardiovascular disease D:\478185952.doc 9 risk of 19% is likely to be in a low risk category whereas someone with a risk of 21% will be determined as high risk and have ongoing medical management and intervention to address the risk. On one hand the high risk individual is labeled as a patient requiring medical intervention; and on the other the low risk person may be falsely reassured that they are ‘normal’ and not be motivated to make positive changes to their lifestyle. Although we can estimate accurately risks for population groups, it is not always easy to predict individual events. Chance is very much involved at the individual level. The impact of this is many individuals categorized as high risk will not experience a cardiovascular event; whereas a substantial proportion of those experiencing heart attacks or strokes will come from the ‘low risk’ groups. Another approach to managing risk for CVD is the population approach which aims to reduce the overall level of risk for everyone, e.g. by reducing salt and saturated fats in food and integrating physical activity into every day activities. Estimates3 to compare the effectiveness of these approaches suggest that the high risk approach , identifying those with CVD risk of ≥20% and treating them (with statins, B blockers< ACE inhibitors and aspirin) would reduce major CVD (MI and stroke) by 34%. A population approach involving a 5% reduction in total cholesterol levels (0.3mmol/ L) and Systolic BP (7mmHG reduction) would lead to a 26% reduction in major CVD. A 10% reduction in cholesterol and systolic BP levels could reduce CVD by 45%. The population approach has the additional merits of addressing other causes of mortality and morbidity e.g. cancer and mental health. 3.3.2 Hypertension PSA01c4 - Percentage of patients on practices' hypertension registers whose last blood pressure reading (measured within the last 9 months) is 150/90 or less Hypertension is common which makes its management an important contribution to prevention of cardiovascular events such as MI and stroke. National prevalence models predicts that there is likely to be about 98,000 people with hypertension above 140/90mmHg within Bedfordshire PCT. There are currently 50,000 people on local GP hypertension registers. Of these 34,000 have a BP measurement of 150/90 or less in the last 9 months, i.e. their hypertension was being controlled through treatment. This represents 70% of all those on the register. Both drug treatment and lifestyle changes, particularly weight loss, an increase in physical activity and a reduction in salt and alcohol intake, can lower blood pressure. 3.3.3 Cholesterol levels in those with CHD PSA01d1 - Percentage of patients on practices' CHD registers whose last measured cholesterol (measured within the last 15 months) is 5mmol/l or less. 3 Emberson, Whincup et al 2004 D:\478185952.doc 10 For those with coronary heart disease, reduction of cholesterol levels in the blood reduces the risk of further cardiovascular events. There are 13,000 people with CHD identified on the GP registers, of whom 9,000 (80%) have a cholesterol level of 5mmol or less; or 62% of the predicted 15,000 people with CHD in Bedfordshire. Blood cholesterol levels can be reduced by drugs, physical activity and by dietary changes, in particular a reduction in the consumption of saturated fat. 3.4 Conclusion Understanding the balance of investment of resources between the high risk approach and the population approach is important for many conditions. In considering the future target for life expectancy this balance will need to be explored. D:\478185952.doc 11 4 Cancer mortality rates Each year approximately 900 people die from cancer in Bedfordshire. Of these deaths, 450 occur in people aged less then 75. Cancer causes the largest number of premature deaths in Bedfordshire. Local programme budget information indicates that the NHS in Bedfordshire spends £22,000,000 on cancer. Figure 5 Mortality rate from all cancers for persons age less than 75 years, trend 1996 to 2004, projection to 2008 160 140 DSR per 100,000 120 England slope -2.78 East of England slope -2.29 Bedfordshire PCT slope -2.29 100 80 60 40 20 0 1996 1997 1998 1999 England 2000 2001 East of England 2002 2003 2004 Bedfordshire PCT 2005 2006 2007 Target Cancer mortality in Bedfordshire appears to be falling in line with regional and national trends. An initial much more ambitious local target was set for reduction of cancer. This was not met and the target was adjusted in 2006. Deaths from cancer can be reduced by the following approaches: Reduction of risk factors. The risk factors smoking and obesity are discussed in section 5 and section 6. Screening for cancer Timely and effective treatments - ensuring that those with suspicious symptoms can be assessed and diagnosed quickly and that those with cancer receive the most effective management from well qualified and experienced teams of specialists. PSA targets are in place with respect to creation of specialist multidisciplinary teams. Other key national priorities for cancer relate to speed of access to cancer and the introduction of bowel cancer screening. D:\478185952.doc 12 2008 4.1 Targets for effective treatment PSA03b Cancer Implementation of National Institute of Clinical Excellence (NICE) Improving Outcomes Guidance (IOGs) Cancer is not one disease – there are different types of cancer occurring in different parts of the body. When the incidence of the disease is relatively low and care is complex, there is a need to concentrate services in specialist centers. This means that people with cancer will be treated by health care teams who treat a lot of people with the condition. There is evidence that this leads to better outcomes. NICE have produced a range of guidance for different cancers called ‘Improving Outcomes guidance’ (IOG). One key strand of the guidance is the setting up of Multi disciplinary teams (MDTs). These MDTs consist of a wide range of specialists, e.g. surgeons, oncologist, nurses, pathologists. These specialists are responsible for managing the care of a sufficient volume of patients with a specific site-specific cancer to ensure quality. Bedfordshire PCT links to two networks, the Anglia Cancer Network and the Mount Vernon Cancer Network. How these networks function is under review. The networks have an important role to ensure the MDTs are in place and patients are able to access quality care pathways. In line with the PSA target designated specialist multidisciplinary teams are in place or under development for: gynaecological cancers upper GI cancers urological cancers haematological cancers specialist palliative care specialist head & neck cancers 4.2 Timely treatments When a diagnosis of cancer is suspected to reduce anxiety and ensure effective care, prompt access to investigation and treatment is required. National targets are in place for all patients with cancers to wait less then one month between diagnosis to treatment and a maximum of two months between urgent GP referral and treatment. Table 4: Percentage of cancer patients at Bedford Hospital waiting less then 31 days between diagnosis and treatment and percentage of cancer patients waiting less then 62 days between urgent GP and treatment. 31 day 62 day Apr May June July Aug Sept Oct Nov Dec Jan 98% 98% 100% 100% 100% 100% 97.8% 100% 100% 100% 100% 94% 100% 98% 100% 93.3% 97.1% 100% 100% 100% 4.3 Screening for cancer – bowel cancer Screening progammes aim to identify those in the early stage of cancer to allow prompt treatment and improved outcomes. National screening programmes are in place for breast and cervical cancer. A new national target is to introduce bowel cancer screening. Work is in progress to establish a bowel cancer screening site in Luton. 4.4 Conclusion As the role of cancer networks is under review, the link to commissioning will need to be reviewed to ensure that the PCT are fully engaged in cancer networks as they develop cancer care pathways spanning prevention, early identification and effective treatment. D:\478185952.doc 13 5 Smoking Outcome measure PSA08 - reducing adult smoking rates to 21% or less by 2010, with a reduction in prevalence among routine and manual groups to 26% or less Most people know that smoking is bad for health. Smoking, more than any other factor, cuts people's life expectancy. As well as being the prime cause of cancer and heart disease, it also causes many other fatal conditions and chronic illnesses among adults. The dangers of smoking are clear. Smoking kills people4: Smokers lose on average 16 years from their life expectancy compared to nonsmokers. Smoking is dangerous at any age, but the younger people start, the more likely they are to smoke for longer and to die early from smoking. Someone who starts smoking aged 15 is 3 times more likely to die of cancer due to smoking than someone who starts in their mid-20s. For every 1000 20-year-old smokers: 1 will be murdered. 6 will die in motor accidents. 250 will die in middle age from smoking. 250 will die in older age from smoking. Smoking causes 84% of deaths from lung cancer, 83% of deaths from chronic obstructive lung disease, including bronchitis. Smoking causes ill health: Regular exposure to second-hand smoke increases risk of CHD by around 25%. Smoking is linked to many other serious conditions including asthma and brittle bone disease (osteoporosis). Some ethnic groups in the UK favour chewed or other oral tobacco, notably betel quid. All forms of tobacco cause cancer. Smoking prevalence is unequally distributed within society being more common among manual social groups than among non-manual groups. In 2004, 31% of men and 28% of women in manual households smoked compared to 22% of men and 19% of women in non-manual households. This class difference has persisted since the 1990s, and recent data suggest no narrowing of the gap. This is a major cause of health in equalities. Smoking 10 cigarettes a day increase risk of post-operative breathing problems by 6. Smoking costs: treating illness and disease caused by smoking is estimated to cost the NHS up to £1.7 billion every year in terms of GP visits, prescriptions, treatment and operations Reducing smoking involves: Health education in relation to preventing initiation of smoking. This work is taken forward for children through the Healthy Schools initiative. Brief advice and specialist support to help people give up smoking. Tobacco control - promoting a smoke free environment and making smoke free the norm. 4 Smoking Kills A White Paper on Tobacco D:\478185952.doc 14 PSA targets are in place for smoking cessation and recording of smoking status in primary care. 5.1 Smoking Cessation PSA08a - Number of 4-week smoking quitters who attended NHS Smoking Cessation services and ratio of smoking quitters per 100,000 population aged 16 and over. One of the most cost-effective health care interventions is smoking cessation. National targets are set for the NHS to support people to quit. Each year Bedfordshire spends £350,000 on smoking cessation services. These services support people to give up smoking and train other health care professionals to support people to give up smoking. Table 5: Actual number of people supported by NHS Smoking cessation services to give up smoking in Bedfordshire and targets. PSA08a Actual Number of 4week smoking quitters Target for 4 week quitters Actual ratio of smoking quitters per 100,000 population. Target ratio 2003/04 1144 2004/05 1521 2005/06 2,459 2006/07 1,209 2007/08 1557 1759 2,288 2,504 2,526 372 564 506 564 705 732 725 A Local Area Agreement target is in place to increase in the number of four week quitters from areas of high deprivation. The aim is to increase the number of quitters from these areas from 177 to 356 each year. So far the performance at quarter three is *139, this equates to 39% of the annual target. Traditionally more quitters have been achieved in the final quarter. *THIS IS FOR BEDFORDSHIRE These figures reveal that Bedfordshire, along with many other areas, has struggled to achieve it smoking cessation targets. 5.2 Recording of smoking status in primary care PSA08b Smoking status among the population aged 16 and over as recorded in GP Currently in Bedfordshire GPs have recorded that 12,222 people smoke. It is estimated that 84,000 people smoke in Bedfordshire. Recording of smoking status underpins: Practices ability to identify and target people at high risk of developing cardio vascular disease and other diseases. Public health’s ability to monitor the impact of work to reduce smoking prevalence. 5.3 Conclusions More work is required locally to ensure current targets are consistently met. D:\478185952.doc 15 6 Obesity PSA10 Obesity - halting the year-on-year rise in obesity among children under 11 by 2010 in the context of a broader strategy to tackle obesity in the population as a whole. 6.1 Why obesity is important Obesity is a contributory risk factor for many chronic diseases including heart disease, stroke, some cancers, type 2 diabetes and other conditions including sleep apnoe and back pain. Obesity and physical inactivity is a risk factor for several major cancers— colon, breast (postmenopausal), endometrial, kidney, and cancer of the oesophagus. In addition, obese people are more likely to suffer from a number of psychological problems such as low self-image and confidence, social stigma, reduced mobility and a poorer quality of life. Overall, there is a nine-year reduction in life expectancy amongst obese patients5. Despite these well documented health risks, the prevalence of obesity in England has more than trebled between 1980 and 2002, from 6% to 22% in men and 8% to 23% in women.6 This increasing prevalence can also be seen in children aged 2 to 10: Between 1995 and 2003, levels of obesity in children rose from 9.9% to 13.7%, and combined levels of overweight and obesity rose from 22.7% in 1995 to 27.7% in 2003. Increases in prevalence were most significant among older children aged 8 to 10 rising from 11.2% in 1995 to 16.5% in 20037. As between 40-70% of obese children will become obese adults, current high levels of overweight and obesity among children will exacerbate the trend towards overweight and obesity in the adult population. Across Bedfordshire, it is estimated that approximately one quarter of the adult population are currently obese, equating to 83,000 people. An additional 40% of men are overweight and 30% of women, equating to an additional 128,000 people who are at an increased health risk. By 2010, if trends continue, 94,000 adults in Bedfordshire will be obese. In 2002, 5.3% of 5-year old children across Bedfordshire were obese compared to an average of 6% across England. Although approximately 1 in 6 children across Bedfordshire (14.8%) were overweight, with 16.3% of 5 year old girls overweight across Bedfordshire compared to a national average of 14.2%. This figure for Bedfordshire is skewed by the significantly higher number of 5 year old girls in South Bedfordshire who are overweight. The Health Select Committee has estimated that the national costs of obesity are £3.3 £3.7 billion per year and of obesity plus overweight at £6.6 - £7.4 Billion. Between 1998 5 Select Committee on Health, 2004 HSE, 2002. 7 DoH 2006 6 D:\478185952.doc 16 and 2004 there has been a 17-fold increase in the drugs used to treat obesity. Annual expenditure on drugs used to treat obesity was more than £30 million in 20048. National Audit Office figures indicate one million fewer obese people in this country could lead to around 15,000 fewer people with coronary heart disease, 34,000 fewer people developing type 2 diabetes, and 99,000 fewer people with high blood pressure. Obesity is an important risk factor for diabetes. 2010 predictions for Bedfordshire PCT are that with current levels of obesity the number of people with diabetes will increase from 14,000 in 2001 to 16,000 in 2010. However if the current rise in obesity continues then the predicted number of people with diabetes is 17,000 in 2010. A reduction in obesity levels to 1995 levels gives predicted levels of 15,000 people with diabetes. PSA targets are in place for measuring obesity in children and in adults. This must occur in the context of an obesity strategy. A local area agreement target exists to support people who are obese to loose weight. 6.2 Measuring obesity in children PSA10a Prevalence of obesity among primary school age children (YR and Y6). In Bedfordshire a system has been agreed to monitor height and weight of all 5-6 (YR) and 10-11 year olds (Y6), as required by Department of Health. Table 6: PSA10a Obesity among primary school age children Total number of primary school age children in Year R and Year 6 recorded as obese for their age in the past school year Total number of primary school age children in Year R and Year 6 height and weight recorded in the past school year Total number of primary school age children in Year R and Year 6 Percentage of children with height and weight recorded who are obese Percentage of children with height and weight recorded 8 2005/06 2006/07 2007/08 actual target target data 138 140 1300 1269 1300 7250 9062 9060 9060 10.87 10.77 17.93 14 14.35 80.02 British Heart foundation http://www.heartstats.org/datapage.asp?id=6158 D:\478185952.doc 17 6.3 Measuring obesity in people over 16 through primary care PSA10b Recording and proportion of people with of BMI of 30 or greater in the last 15 months in people aged 16 and over on GP list. Table 7: Expected number of people and recorded number of people on GP registers for Hypertension, coronary heart disease, cardiovascular disease, diabetes, smoking and obesity Number of people predicted in Bedfordshire PCT’s population Obesity 83,000 Actual number of people recorded on GP practice registers within Bedfordshire PCT 30,000 6.4 Helping people to lose weight There is a local area agreement target to increase in the number of recorded obese individuals aged 15-75 completing a personalised weight management programme in accordance with Department of Health protocol and achieving a minimum 5% loss of initial bodyweight. For this target an obese individual is a person with a BMI9 of 30+, or 28+ with other illnesses such as: diabetes, CHD, Angina, heart failure or hypertension. A target of 399 people has been set for the period 2006/07 to 2008/09. By December 2006, 76 people had been recruited with 8 achieving a 5% loss in body weight. 6.5 Conclusions At present we are on course to meet national and local targets with respect to obesity. However delivery of these targets is insufficient to halt the year on year increase in obesity. 9 Body Mass Index (BMI) is your weight in kilograms divided by the square of your height in metres. In the UK, people with a body mass index between 25 and 30 are categorised as overweight, and those with an index above 30 are categorised as obese D:\478185952.doc 18 . 7 Conclusions On average people in Bedfordshire live longer then men and women in England. However, our life expectancy is not better then Eastern Region. This is despite the fact that Bedfordshire experiences less deprivation then Eastern Region as a whole. It appears more can be achieved. The biggest causes of early deaths are cancer and heart disease / stroke. Improving our death rates will involve ensuring: the people of Bedfordshire have good access to timely and effective treatment. there are systems in place to identify people early who have disease and ensure effective treatment to reduce future risk. we tackle the key determinant of disease including smoking and obesity. This report has reviewed progress against national PSA targets to improve life expectancy. It has highlighted Bedfordshire is making progress against all targets, but progress could be better. There is also concern that work on obesity is insufficient to impact on the future health status of the population. More ambitious targets on smoking could also improve health. Our current targets expire in 2010. New targets will soon be required. This report seeks to stimulate a debate regarding how ambitious our future target to improve life expectancy should be. D:\478185952.doc 19