Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
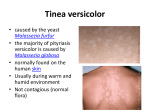
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE – 41 REGISTRATION OF SUBJECT FOR DISSERTATION 1. NAME OF THE CANDIDATE AND SHIVARAJ, ADDRESS POST GRADUATE (M. Sc. M.L.T.), DEPARTMENT OF MICROBIOLOGY, ST. JOHN’S MEDICAL COLLEGE AND HOSPITAL, SARJAPUR ROAD, BANGALORE-560034. 2. NAME OF THE INSTITUTION ST. JOHNS MEDICAL COLLEGE 3. COURSE OF STUDY & SUBJECT M. Sc. M.L.T. (MICROBIOLOGY) 4. DATE OF ADMISSION TO THE SEPT 1ST 2009 COURSE 5. TITLE DETECTION, ISOLATION AND SPECIATION OF MALASSEZIA FROM PATIENTS WITH SUPERFICIAL CUTANEOUS MYCOSES. 1 6. Brief Resume of the study 6.1 Need for study: Superficial cutaneous mycosis is a common clinical condition seen in our country. It may be caused by Dermatophytes, Malassezia, Candida or Trichosporon species. The genus Malassezia most commonly cause superficial cutaneous infection, but rarely in people with certain predisposing factors become invasive and cause opportunistic systemic infection1,2. Among the superficial cutaneous infections, Pityriasis versicolor is the most common and others include seborrheic dermatitis, atopic dermatitis and folliculitis2. The taxonomic status of this genus has been recently expanded to include eleven species3,4. Although diagnosis based on typical yellow fluorescence of the involved skin on Wood’s Lamp examination and “spaghetti and meat ball” or “banana and grape” appearance on direct microscopy with 10% Potassium hydroxide (KOH) examination of skin scrapings are technically simple and offer quick diagnosis, culture based diagnosis is of utmost importance to establish the clinico-mycological relationship2,5. All species of Malassezia except Malassezia pachydermatis are lipophilic and therefore their isolation and speciation, unlike other fungi, is technically demanding. Although, there is evidence to suggest variation in geographical distribution of the different species, not much data is available from our country4,5,6. This study, therefore, will help us to establish and standardize techniques of isolation and speciation of Malassezia and also understand the species distribution in our centre. 6.2 Review of literature: The genus Malassezia is commonly responsible for a variety of superficial cutaneous infections and rarely opportunistic systemic fungal infection in immunocompromised patients. Pityriasis versicolor is the most common presentation and the others include seborrheic dermatitis, atopic dermatitis and folliculitis2,5. The fungus that causes Pityriasis versicolor was detected and described for the first time by Eichstedt in 1846 and by Sluyter in 18477. In 1853, Robin named the fungus 2 as Microsporum furfur, as he thought it was similar to the dermatophyte, Microsporum audouinii. Hence, the disease was renamed as tinea versicolor1. In 1874, Malassez described yeast like cells from a lesion of the scalp and called them “Spores”. In 1884, Bizozero observed spherical as well as elliptical yeast like cells in epidermal scales of the humans and noted that these yeast cells were similar to the “Spores of Malessez” and named spherical cells Sacchromyces sphaericus and the oval cells S. ovalis. In 1889, Baillon recognized the etiological agent to be different from Microsporum species and included this group of yeasts under a new genus Malessezia7. In 1904, Sabouraud considered this organism as a causative agent of dandruff and gave it a new name, Pityrosporum malassez1. Acton and Panja considered Pityrosporum to be synonym of Malassezia, but they failed to prove it7. But in 1969, Sternberg and Keddie detected the same antigenic components in Pityrosporum orbiculare and Malassezia furfur by the fluorescent antibody technique which proved that both are synonymous1. Isolation of the fungus in culture media was not successful until the lipophilic nature of Malassezia was described in 1939 by Barham7. In 1951 Gordon isolated yeast like fungus and named it as Pityrosporum orbiculare. In 1961, Burke was able to produce clinical Pityriasis versicolor by inoculating Pityrosporum orbiculare on the skin of persons with high plasma cortisol levels. In 1981, Redline and Dahm reported for the first time invasion of deep tissue by M. furfur and later Hassall and colleagues reported the same in young children receiving intravenous lipid therapy7. The distribution of Malassezia infection is world wide, but the disease is more prevalent in tropical and subtropical climates5,7. Studies from India show infection to be twice more common in males. It occurs mostly in the age group of 11-20 years. The disease is rare above 50 years of age8. Species distribution varies in different parts of India. M. sympodialis is the predominant species of human skin, in health and disease, followed by M. globosa, which is commonly found in scales of Pityriasis versicolor. M. restricta seems to be associated with Pityriasis capitis6,9. M. furfur is seldom found as normal flora or in disease states9. Recently the taxonomic status of the genus Malassezia has been expanded to include eleven species by their physio-biochemical properties as well as molecular 3 studies3,4. It includes M. globosa, M. restricta, M. sympodialis, M. furfur, M. obtusa, M. slooffiae, M. pachydermatis, M. japonica, M. nana, M. dermatis and M. yamatoensis. Important techniques used in the diagnosis and identification of Malassezia include, Wood’s Lamp examination of the lesions which show golden yellow fluorescence of the scaly lesions. Direct microscopic examination of 10% KOH preparation of skin scraping shows characteristic “spaghetti and meat balls” or “banana and grape” appearance2,5. Addition of an equal amount of Parker blue/black Quink permanent fountain ink to KOH (Parkers stain) enhances the visibility, as the bright blue stain is taken up by the organism. Calcofluor white fluorescent staining may also be used to avoid confusion from artifacts1,2,5. Isolation of Malassezia from clinical samples is done by inoculation on Sabouraud Dextrose Agar (SDA) with 0.5% chloramphenicol, 0.5% cycloheximide and source of lipid, in the form of olive oil2,5. Colonies are characteristically small 3-6mm, cream to yellow in colour, with slightly raised irregular edges, developing within 5-6 days at 32-35oC2,10. Lactophenol cotton blue (LPCB) mounting can be done for characteristic microscopic features. Apart from S.D.A., other media such as mDixon (modified Dixon) agar and Leeming and Notman agar can be used5. Speciation of Malassezia is done by routine biochemical and physiological tests like lipid dependency for their growth, temperature tolerance, catalase reaction, esculin splitting by β-glucosidase activity and tween assimilation2,3,5. Recently molecular typing methods such as Polymerase Chain Reaction (PCR) and Restriction fragment length polymorphism (RFLP) have also been used in speciation3,5. Malassezia species are susceptible to a variety of topical antifungal agents like 2.5% selenium sulphide, 1% zinc pyrithione and azoles such as clotrimazole and 2% ketoconozole5,11. The treatment duration is about 2-3 weeks11. In case of failure with topical agents or in severe cases with extensive lesions use of systemic antifungals with oral ketoconozole, fluconozole or itracozole is found to be effective5,12. Patients with fungemia can be treated with intravenous administration of amphotericin B or fluconozole4. 4 6.3 Objectives of the study: 1. To study the occurrence of Malassezia in clinically suspected cases of superficial cutaneous mycoses. 2. To isolate and speciate Malassezia from the above cases. 3. To study the clinical correlation in patients with underlying disease conditions from whom Malassezia is isolated 7. Materials and Methods: 7.1 Source of Data: Patients visiting the Dermatology OPD of St. John’s Medical College and Hospital during the period 1st January 2010 to 31st December 2010 whose skin scrapings on direct KOH preparation reveal the typical “spaghetti and meat balls” or “banana and grape” appearance will be included in this study. A minimum of 100 such clinical samples will be studied. 7.2 Methods: Sample Collection2: Skin scrapings will be obtained from the multiple sites of lesion after cleaning the site with 70% alcohol using sterile blunt scalpel. Sample processing2,5: 1. Direct microscopic examination of skin scrapings: using 10% KOH. 2. Culture: S.D.A with 0.5% chloramphenicol, 0.5% cycloheximide and olive oil as lipid source will be used. Speciation of isolates: by their physio-biochemical properties using the following tests2,3,5. 1. Lipid dependency for their growth. 2. Temperature tolerance. 3. Catalase reaction. 4. Esculin splitting by β-glucosidase activity. 5. Tween assimilation. 5 Data to be collected from medical records will include: I. Demographic details of patient Name Age Sex Address Occupation II. Distribution of lesions and type (as described by the treating dermatologist). III. Wood’s Lamp Examination findings (as described by the treating dermatologist). IV. Underlying medical conditions such as Diabetes Mellitus, Steroid therapy, HIV status (if report already available or test done as part of treatment) and any other illness. 7.3 Inclusion Criteria: Only those patients whose skin scrapings on direct 10% KOH examination reveal the typical “spaghetti and meat balls” or “banana and grape” appearance will be included in this study. 7.4 Exclusion criteria: Those patients whose skin scrapings on direct microscopic examination do not show the typical appearance are excluded from the study. 7.5 Does the study require any investigation or interventions to be conducted on patients or other than human beings or animals? If so, describe briefly. No 7.6 Has ethical clearance been obtained from your institution in case of 7.3. Not applicable 6 8. References: 1. Inamadar Arun C, Palit Aparna. The genus Malassezia and human disease. Ind J Dermatol Venereol Leprol 2003;69(4):265-70 2. Chander Jagadish. Medical Mycology. 2nd ed. New Delhi (India): Mehtha; 2002. p. 70-78 3. Shokohi T, Afshar P, Barzgar A. Distribution of Malassezia species in patients with Pityriasis versicolor in Northern Iran. Ind J Med Microbio 2009;27(4):32124. 4. Anaissie Elias J, Ginnis Michael Mc. R, Haller Michell AP. Clinical Mycology. 2nd ed. China: Churchill Livingstone Elesvier; 2009. p. 251-54 5. Merz Willium G, Hay Roderick J, editors. Topley & Wilsons Microbiology and Microbial Infections – Medical Mycology. 10th ed. London (Eng): Hodder Arnold; 2005. p. 185,202-19 6. Kindo AJ, Sophia SKC, Kalyani J, Anandan S. Identification of Malassezia species. Ind J Med Microbio 2004;22(3):179-81. 7. K.J. Kwon – Chung, Bennett John E. Medical Mycology. USA: Lea & Febiger; 1992. p. 170-82. 8. Ghosh Sudip Kumar, Dey Sunil Kumar, Saha Indranil, Barbhuiya Jayashree Nath, Ghosh Arghyaprasun, Roy Aloke Kumar. Pityriasis versicolor: A clinicomycological and epidemiological study from a tertiary care hospital. Ind J Dermato 2008;53(4):182-5. 9. Dutta Sidhartha, Bajaj AK, Basu S, Anupam Dikshit. Pityriasis versicolor: Socioeconomic and clinic-mycologic study in India. Int J of Dermato 2002;41:823-4 10. Larone Davise H. Medically Important Fungi – A guide to identification. 4th ed. Washington(USA): ASM; 2002. p. 136-7,309 11. Cook Gordon. Mansons Tropical diseases. 20th ed. London (Eng): Saunders; 1996. p. 1055-56 12. Fauci Anthony S. Braunwald Eugene, Kasper Dennis L, Hauser Stephen L, Longo L. Dan, Jameson Larry J et. al. editiors. Harrisons principles of internal medicine: Vol 1. 17th ed. USA: The Mc-Graw Hill Medical; 2008. p. 1263 7 SIGNATURE OF THE CANDIDATE NAME AND DESIGNATION OF THE DR. JAYANTHI SAVIO, ASSISTANT PROFESSOR, GUIDE DEPARTMENT OF MICROBIOLOGY, ST. JOHN’S MEDICAL COLLEGE AND HOSPITAL, BANGALORE - 560034 REMARKS OF THE GUIDE SIGNATURE OF THE GUIDE DR. S. MURALIDHARAN HEAD OF THE DEPARTMENT PROFESSOR, DEPT. OF MICROBILOGY, ST. JOHN’S MEDICAL COLLEGE AND HOSPITAL, BANGALORE - 560034 SIGNATURE OF THE HOD REMARKS OF THE DEAN OF DEAN OF INSTITUTION SIGNATURE OF THE INSTITUTION 8