Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
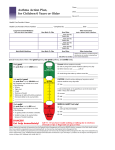
American Lung Association th 27 Annual Respiratory Care Conference Asthma Response Team Clifton Dennis, RRT, AE-C Pediatric Lifetime and Current Prevalence 18 16 14 12 10 Lifetime current 8 6 4 2 0 Georgia 38 States Pediatric Asthma Prevalence 16 14 12 10 Georgia 38 States 8 6 4 2 0 0-4 years 5-9 years 10-14 years 15-17 years Pediatric Asthma By Sex 16 14 12 10 Georgia 38 States 8 6 4 2 0 Boys Girls Pediatric Asthma By Race/Ethnicity 20 18 16 14 12 Georgia 38 States 10 8 6 4 2 0 White Blacks Hispanic Other Multirace Pediatric Asthma Hospitalization Rates Georgia 250 200 150 100 50 0 0-4 yrs 5-9 yrs 10-14 yrs 14-17 yrs Asthma Deaths 30 25 20 Georgia United States 15 10 5 0 White Black Other Pediatric Asthma Deaths CSRA 1999-2006 4.5 4 3.5 3 2.5 2 1.5 1 0.5 0 1999 2000 2001 2002 2003 2004 2005 2006 Asthma Response Team responsibilities Introduction and explanation of why we are here Complete ART encounter form Initial PEF, FVC. FEV1 Will determine severity based on EPR-3 guidelines for this admission Review two week history of symptoms to determine severity Review one year history to determine risk Review asthma disease and the asthma process provide asthma booklet/packet Explain the use of Quick Relievers and Controllers 1. Review albuterol use 2. Review ICS usage 3. Review MDI/DPI usage with demonstration Review triggers- Mention smoking cessation 1. Trigger avoidance 2. Ozone trigger 3. Encasements- available through CMS if qualified Review spacer with/without mask 1. Provide adults with spacer 2. Provide children with spacer /mask in Asthma Kit Review peak flow meter usage 1. Teach proper peak flow 2. Label peak flow meter with predicted values Insure follow up appointment is made prior to discharge 1. Specialist appointment is recommended for high risk, moderate to severe patients 2. Intermittent to mild may follow up with PCP May use MCG continuity Clinic@ 721 -2143 from 8-4:30 as walk in if needed Complete Asthma Action Plan- Utilize GREAT for asthma action plan. Will require parental signature 1. 1- copy to parent/patient 2. 1- copy for medical records (signed copy) 3. 1- copy for ART team 4. This will be faxed to school nurse and PCP if applicable Provide Asthma kit, spacers & peak flow meters Document whom provided ART services, equipment used and serviced provided by the ART team member. Asthma Response Team Encounter Form Patient Information Race Gender Patient name Date of birth Age Height Clinical asthma severity score (CAS) Score Triage score 30 minute score 1 hour score Discharge Score Inpatient admit score PICU admit score Predicted Peak flow Actual PEF FEV1 FVC Impairment Coughing Wheezing Trouble breathing Limited activities Awaking at night Patient label Visit Information Visit date Primary care MD School County Zip code Emergency room physician Reason for visit Severity of Asthma Well controlled Not well controlled Very poorly controlled # of days in past two weeks Past Asthma History ( Risk) # of visits to ER for asthma in past 12 mos. # of office visits for asthma last 12 mos. # of hospital admissions for asthma (2/yr persistent) # of ICU admissions for asthma (1=persistent) # of times oral steroids have been used in 12 mos. ( more than 2 /yr = persistent asthma) Use of quick relievers Current Medications Albuterol ( Proair, Ventolin,Proventil) Levalbuterol ( Xopenex) Cromolyn, Intal, Tilade Inhaled Steroid ( Flovent, Pulmicort, Qvar,Areobid,Asmenex) Oral steroid ( Prednisone, Deltasone, Prednisolone, Decadron, Prelone, Pedipred) Leukotriene modifiers ( Singulair,Accolate,Zyflo ) PO Services Provide by ART Team member Supplies provided to patient Nebulizer Treatment Peak flow meter MDI treatment Spacer with mask DPI treatment Spacer without mask Education Asthma Kit Home Phone #_________________________________________________________________________________ Cell Phone# ___________________________________________________________________________________ Alternate # ____________________________________________________________________________________ Jet MDI DPI Classification Intermittent Mild persistent Moderate Severe Persistent Residence Counties 200 180 160 140 120 100 80 60 40 20 0 Richmond county Aiken County Columbia County Edgefield County Children's Medical Service Enrollment 120 103 100 86 80 60 55 40 20 0 CMS Asthma PACK Asthma Classification 120 100 80 60 40 20 0 intermittent mild persistent moderate persistent severe persistent Health Care Utilization 3 2.5 2.5 2 2 1.5 1 1 0.5 0 0 Avg. ED visits Avg. PCP visits Avg. Hospitalizations Avg. PICU admissions Average CAS by location 7 6 6 5 4 3 5 4 3 3 2 1 1 0 initial score 30 min score 1 hour score Discharge score Inpatient score PICU score Patient Disposition 250 217 200 PICU Inpatient ED Discharge 7 day return 150 100 50 24 3 0 5 Metrics Teamwork Award for ART team References • Introduction: Enhancing the role of the emergency Department in the identification and management of childhood asthma: Rechelefsky, Kennedy, and Stone Pediatrics 2006 • Expert Panel Review number 3, NHLBI, 2007 • Behavioral Risk Factor Surveillance System, (BRFSS) CDC ,2008