Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
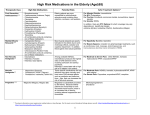
Prescribing in Elderly Populations C H R I S T I N A B U C H M A N , P H A R M . D. C l i n i c a l A s s i s t a n t P r o fe s s o r a t Wa s h i n g t o n S t a t e U n i v e r s i t y C o l l e g e o f P h a r m a c y Ya k i m a E x t e n s i o n P r o g r a m Learning Objectives By the end of this seminar, the learner should be able to: ◦ Identify risk factors present when prescribing to elderly patients ◦ Discuss interventions to decrease ADEs in senior populations What Defines “Elderly”? Age alone is not a good description Look at overall function with categories ◦ youngest old (65-74) ◦ middle old (74-85) ◦ oldest old (85 and above) Geriatric patients ◦ Gait abnormalities and/or falls ◦ Depression ◦ Fatigue ◦ Cognitive impairment ◦ Dementia with or without behaviors ◦ Urinary incontinence ◦ Reduced strength ◦ Sedentary lifestyle ◦ Weight loss Reference: http://my.clevelandclinic.org/services/medicine-institute/geriatric-medicine/patient-caregiver-education Medication Use in the Elderly Elderly make up 12%-13% of U.S. population ◦ Take 30% of all prescription drugs Among people 65 years and older: ◦ 90% use at least 1 drug per week ◦ >40% use at least 5 drugs per week ◦ 12% use 10 or more drugs per week 40% of people who suffer adverse drug reactions (ADRs) are over 60 years of age ◦ 1/6th of hospital admissions are related to ADRs Pharmacodynamic/Pharmacokinetic Differences in Geriatric Patients Why do we focus on geriatric patients with regard to medications? ◦ Decreased CLEARANCE ◦ Increased SENSITIVITY ◦ Multiple MEDICATIONS ◦ Geriatric Differences (cont.) Greater likelihood of CONFUSION Potential multiple MEDICAL CONDITIONS ◦ Increased risk of DRUG INTERACTIONS / SIDE EFFECTS ◦ Treatment more confusing for the patient Physical LIMITATIONS COST issues may be more likely Adverse Drug Reactions 70% of ADRs Result From: ◦ Unnecessary Drugs ◦ Drug-Drug Interactions ◦ Contraindicated (drugs that should not be used in that person, e.g., people with certain heart conditions should not receive certain drugs for the treatment of Alzheimer’s disease) Likelihood ◦ 2 drugs used : 6% ◦ 5 drugs used : 50% ◦ 8 drugs used : 100% ◦ (must note that not all of these may result in harm or are always critical) Drug Classes of Concern in the Elderly The Beers Criteria Developed by the American Geriatrics Society and last updated in 2015 3 categories of drugs ◦ Inappropriate – Always to be avoided ◦ Potentially inappropriate – To be avoided in certain diseases or syndromes ◦ To be used with caution – Benefit may offset risk in some patients Beers Criteria Medications Class Drugs Recommendation Quality of Evidence/ Strength of Rec. Anticholinergics First gen antihistamines (diphenhydramine), Antiparkinsonian agents (benztropine), Antispasmodics (dicyclomine) Avoid Moderate/Strong Antithrombotics Dipyridamole, ticlopidine Avoid Moderate/Strong Anti-infectives Nitrofurantoin Avoid long term use and if CrCl<30 Low/Strong Cardiovascular Peripheral alpha-1 blockers (doxazosin), central alpha blockers (clonidine) Amiodarone/dronaderone, Digoxin Avoid to control HTN Moderate/Strong Avoid as 1st-line High/Strong Antidepressants (TCAs, paroxetine), barbiturates, benzodiazepines, sedative/hypnotics (z-drugs) Antipsychotics (1st and 2nd gen) Avoid High/Strong Avoid-unless dx need Moderate/Strong Endocrine Androgens, Estrogen Desiccated thyroid Sliding scale insulin (↑risk, no benefit) Sulfonylureas (long-acting) Avoid Moderate/Weak High/Strong Moderate/Strong High/Strong Gastrointestinal Metoclopramide (EPS effects) PPIs Avoid Avoid long term Moderate/Strong High/Strong Pain Medications NSAIDs (non-COX-selective) Muscle relaxers Avoid chronic use Avoid Moderate/Strong CNS STOPP-START Tool for Safe Prescribing in the Elderly Outlines criteria for stopping or starting medications in patients 65 years and older Many categories ◦ Cardiovascular ◦ Antiplatelet/Anticoagulant ◦ CNS and Psychotropic ◦ Others Similar recommendations to Beers Criteria List ◦ Recommendations more specific and explicit Validated by Delphi method Most recent update in 2015 STOPP – Section B: Cardiovascular System Potentially inappropriate prescribing includes: 1. Digoxin for heart failure with normal systolic ventricular function (no clear evidence of benefit). 2. Verapamil or diltiazem with NYHA Class III or IV heart failure (may worsen heart failure). 3. Beta-blocker in combination with verapamil or diltiazem (risk of heart block). 4. Beta blocker with bradycardia (< 50/min), type II heart block or complete heart block (risk of complete heart block, asystole). 5. Amiodarone as first-line antiarrhythmic therapy in supraventricular tachyarrhythmias (higher risk of side-effects than beta-blockers, digoxin, verapamil or diltiazem). 6. Loop diuretic as first-line treatment for hypertension (safer, more effective alternatives available). 7. Loop diuretic for dependent ankle edema without clinical, biochemical evidence or radiological evidence of heart failure, liver failure, nephrotic syndrome or renal failure (leg elevation and /or compression hosiery usually more appropriate). 8. Thiazide diuretic with current significant hypokalemia (i.e. serum K+ < 3.0 mmol/l), hyponatremia (i.e. serum Na+ < 130 mmol/l) hypercalcemia (i.e. corrected serum calcium > 2.65 mmol/l) or with a history of gout (hypokalemia, hyponatremia, hypercalcemia and gout can be precipitated by thiazide diuretic). 9. Loop diuretic for treatment of hypertension with concurrent urinary incontinence (may exacerbate incontinence). 10. Centrally-acting antihypertensives (e.g. methyldopa, clonidine, guanfacine), unless clear intolerance of, or lack of efficacy with, other classes of 2 antihypertensives (centrally-active antihypertensives are generally less well tolerated by older people than younger people). 11. ACE inhibitors or Angiotensin Receptor Blockers in patients with hyperkalemia. 12. Aldosterone antagonists (e.g. spironolactone, eplerenone) with concurrent potassium-conserving drugs (e.g. ACEI’s, ARB’s, amiloride, triamterene) without monitoring of serum potassium (risk of dangerous hyperkalemia i.e. > 6.0 mmol/l – serum K should be monitored regularly, i.e. at least every 6 months). 13. Phosphodiesterase type-5 inhibitors (e.g. sildenafil, tadalafil, vardenafil) in severe heart failure characterized by hypotension i.e. systolic BP < 90 mmHg, or concurrent nitrate therapy for angina (risk of cardiovascular collapse). Case 1 KH is a 78 year old female with a history of diabetes (type 2), insomnia, hypertension, hypothyroid, and osteoarthritis. Her current renal function (GFR) is estimated at 36 mL/min. She is taking glyburide 5mg daily, levothyroxine 80mcg daily, acetaminophen 1000mg TID, atenolol 50mg daily, diltiazem XR 120mg daily, amitriptyline 50mg at bedtime and Tylenol PM as needed to sleep. She has no reported allergies. Which of her current medications are concerning in the elderly? A. B. C. D. E. Acetaminophen Tylenol PM Atenolol Amitriptyline Glyburide Drug-Related Problems in the Elderly Prescribing Cascade Drug 1 ADE interpreted as new medical condition Drug 2 ADE interpreted as new medical condition Drug 3 Prescribing Cascade Example Drug-induced Parkinsonism can result from commonly used antiemetics (metoclopramide, promethazine) and antipsychotics (all except quetiapine and clozapine) Can lead to misdiagnosis as new onset Parkinson’s disease and treatment with a new drug ◦ start acetylcholinesterase inhibitor (donepezil) ◦ new onset of urinary incontinence ◦ adding an anticholinergic medication (oxybutynin) ◦ and so on Drug-Disease interactions Disease Drugs Heart Failure (exacerbate HF or promote fluid retention) Cilostazol, NSAIDs (including COX-2 Inhibitors), donaderone, non-dihydropyridine Ca channel blockers, thiazolidinediones Syncope (risk of orthostatic hypotension and bradycardia) AChE Inhibitors, chlorpromazine, peripheral α-blockers, TCAs, olanzapine, thioridazine Seizures/epilepsy (lowered seizure threshold) Bupropion, chlorpromazine, clozapine, maprotiline, olanzapine, thioridazine, thiothixene, tramadol Delirium (worsening) TCAs, benzodiazepines, anticholinergic drugs, chlorpromazine, corticosteroids, H2 blockers, meperidine, sedative hypnotics, thioridazine Dementia/Cognitive Impairment Antipsychotics (chronic and as-needed use), benzodiazepines, anticholinergic drugs, H2 blockers, zolpidem Hx of falls or fractures Anticonvulsants, antipsychotics, benzodiazepines, nonbenzodiazepine hypnotics, TCAs, SSRIs Chronic Constipation Antispasmodic and anticholinergic drugs, TCAs, first-generation antihistamines, nondihydropyridine Ca channel blockers, oral antimuscarinics for urinary incontinence Urinary incontinence Estrogen (in women), α-blockers BPH/ urinary retention Drugs that have strong anticholinergic effects (except antimuscarinics for urinary incontinence), inhaled agents that have anticholinergic effects Other Drug-Related Problems: Drug-drug interactions ◦ The elderly take a large number of drugs and often take herbal and dietary supplements ◦ Drug-drug interactions are different in the elderly due to pharmacokinetic and pharmacodynamics differences Inadequate monitoring ◦ Documenting indications for new medications, keeping a current list, monitoring for efficacy and ADEs, periodic review for necessity Inappropriate drug selection ◦ START criteria can help guide agent choice Lack of patient adherence ◦ Financial/physical constraints, cognitive decline, multiple drugs, multiple times a day dosing Overdosage ◦ Renally cleared drugs, start low and go slow Under prescribing ◦ Commonly under prescribed: opioids, β-blockers, antihypertensives, Alzheimer drugs, anticoagulants, immunizations Case 2 LT is a 69 year old male with a history of diabetes (type 2), hypertension, hyperlipidemia, and gastroparesis secondary to diabetes. His current medications include Lantus 80 units QHS, metformin XR 1000mg daily, simvastatin 40mg daily, benazepril 20mg daily, and metoclopramide 10mg prior to meals. He came into the clinic last month with a new onset tremor at rest and was diagnosed with new onset Parkinson’s Disease. He started levodopa 250mg BID at that time and it has since improved his symptoms. What are the issues with this case? What would you like to change in this case? Bringing it all together Case 3: “Spiraling out of control” MM is an 86 y/o Asian woman who presents to the clinic with increased confusion and agitation Patient speaks fluent Cantonese and minimal English Patient’s daughter is the primary source of patient’s medical history Chief complaint: patient is “Spiraling out of control” Daughter reports the following about MM: ◦ ◦ ◦ ◦ ◦ ◦ worsening memory, difficult to manage got lost on way home non-adherent to medications trouble sleeping worsening bladder control worsening OA pain (hands) Case 3 Family/Social History: Lives at home with her 61 y/o daughter who recently retired as a seamstress Rx payment: Medicare Part D coverage with step therapy Pharmacy(ies) used: Uses multiple pharmacies where patient’s daughter can get the lowest drug prices Case 3: Medications and OTC Case 3: Physical Exam and Lab Vital signs ◦ BP= 134/82 mm Hg; Pulse= 73 bpm, regular; Temp = 98.4 °F; RR = 18/min ◦ Height = 4’ 10” Weight = 90 lbs. BMI =18.8 kg/m2 Pain score 6/10 MMSE = 16/30 (21/30 4 months ago) Lab test ◦ ◦ ◦ ◦ Ca2+= 9.1 mg/dL | Mg = 2.2 mEq/L | PO4 = 4.2 mg/dL Albumin = 3.8 d/dL | Bili = 0.8 mg/dL | Alk Phos = 88 U/L AST= 32 U/L | ALT= 37 U/L TSH = 0.22 μU/mL Bone density screening from a community pharmacy event ◦ T-score: < -1 (Reference: > -1 Low risk; 0 to -1 Moderate risk; < -1 high risk) Case 3: Review of Systems General: confused and agitated HEENT: diminishing vision Musculoskeletal: pain in both hands, unable to grip well and dropping things, some difficulty buttoning blouse GU: incontinence, with 3-5 accidents/week, including evenings Case 3: Caregiver Assessment Daughter is the sole caregiver to MM Daughter feels guilty about putting MM in a nursing facility and wants to continue to care for her mother in their own home Cost for caring for MM is becoming a burden Resorted to using herbal remedy and OTC medication to minimize drug cost Case 3: Dementia What labs do we have that could contribute to her worsening cognition? What other labs should be drawn for MM to better evaluate her declining cognition? What is the most likely cause of her sudden cognitive decline? ◦ MMSE = 16/30 (21/30 4 months ago) – moderate dementia Drug-induced Dementia Diphenhydramine has strong anticholinergic properties, but due to the low dose and frequency used, it is unlikely to cause significant cognitive adverse effects Valerian root is an herbal product used to aid in sleeping. Valerian root has been shown to inhibit of CYP 3A4 in vitro studies Darifenacin for MM’s OAB is a CYP 3A4 substrate that also strong anticholinergic properties Valerian root could have exacerbated anticholinergic adverse effect from Darifenacin PLAN: discontinue valerian root tea Dementia Treatment MM is diagnosed with moderate Alzheimer’s disease dementia. Which of the following would be the best treatment for her? A. B. C. D. Memantine 5 mg daily Donepezil 5 mg at bedtime Rivastigmine 4.6/24 hrmg patch daily Donepezil 5 mg at bedtime plus memantine5 mg daily Case 3: OAB MM’s daughter also reports that her mother has worsening bladder control. Which of the following are possible predisposing factors? A. Cognitive impairment, thyroid disease, and constipation B. Glaucoma, thyroid disease, and osteoarthritis C. Poor medication adherence, glaucoma, and constipation D. Thyroid disease, glaucoma, and constipation Treatment for OAB Which of the following medications is best suited for MM’s worsening OAB because of minimal cognitive adverse effects and potential for drug interaction? A. B. C. D. Mirabegron Fesoterodine Tolterodine Trospium Case 3: Osteoarthritis MM’s osteoarthritis pain is poorly controlled. Her physician wants to discontinue the acetaminophen/codeine due to concerns about cognitive impairment and the risk for falling. Which of the following would be the best recommendation to treat MM’s OA pain? A. Start diclofenac 1% gel 2 g 4 times a day to the affected area B. Start naproxen 500 mg po twice daily C. Start tramadol 50 mg po every 6 hours D. Increase the dose of plain acetaminophen from 650 mg po three times daily to 650 mg po every 6 hours Wrapping it up MM has other conditions that need managed today: ◦ Osteoporosis ◦ T-score of <-1 High risk at screening event. ◦ Glaucoma ◦ Daughter reports not being able to refill her mother’s prescription for tafluprost due to its high cost ($165/month). ◦ Hypothyroid ◦ TSH was 0.22 μU/mL Questions? You can email questions to me at [email protected] Thanks!! References 1. 2. 3. 4. Ruscin JM, Linnebur SA. Drug Therapy in the elderly (June 2014). Merck Manual Professional Version Web site. Available at: http://www.merckmanuals.com/professional/geriatrics/drug-therapyin-the-elderly/introduction-to-drug-therapy-in-the-elderly. Accessed February 16, 2017. Rochon PA, Gurwitz JH. Optimizing drug treatment in elderly people: the prescribing cascade. BMJ 1997;315:1097. O'Mahony D, O'Sullivan D, Byrne S, O'Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015 Mar;44(2):213-218. Clinical Pharmacology [database online]. Tampa, FL: Gold Standard, Inc.; 2017. URL: http://www.clinicalpharmacology.com.