Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
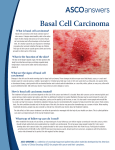
MOC Self-Assessment David Fieleke, MD A 27 year-old male was recently diagnosed with his seventh basal cell carcinoma. A photograph of his palm and panoramic radiograph of the upper and lower jaw are shown below. A germline mutation in which gene is the primary cause of his syndrome? A. TYR B. XPA-XPG C. BLM / RECQL3 D. CDKN2A E. PTCH1 A 27 year-old male was recently diagnosed with his seventh basal cell carcinoma. A photograph of his palm and panoramic radiograph of the upper and lower jaw are shown below. A germline mutation in which gene is the primary cause of his syndrome? A. TYR B. XPA-XPG C. BLM / RECQL3 D. CDKN2A E. PTCH1 A 27 year-old male was recently diagnosed with his seventh basal cell carcinoma. A photograph of his palm and panoramic radiograph of the upper and lower jaw are shown below. A germline mutation in which gene is the primary cause of his syndrome? A. TYR B. XPA-XPG C. BLM / RECQL3 D. CDKN2A E. PTCH1 E. PTCH1 This patient has basal cell nevus syndrome, an autosomal dominant disorder caused by a germline mutation in PTCH1 (or less commonly PTCH2 or SUFU) which is part of the sonic hedgehog signaling pathway. Patients with basal cell nevus syndrome develop numerous basal cell carcinomas, usually beginning at a young age (median age of onset is 20). Associated developmental defects can include palmar and plantar pits, macrocephaly, dysgenesis of the corpus callosum, falx cerebri calcification, coarse facies, cleft palate, bifid ribs, and spina bifida occulta). Basal cell nevus syndrome patients are also predisposed to multiple other neoplasms including, medulloblastomas, meningiomas, odontogenic keratocysts, rhabdomyosarcomas, fibrosarcomas, cardiac fibromas, and ovarian fibromas. Schematic of the sonic hedgehog (SHH) pathway in a representative keratinocyte. Normally, hedgehog ligand activates the pathway by binding to and inhibiting PTCH1, allowing depression of smoothened (SMO), activation of suppressor of fused gene (SUFU), and the downstream upregulation of GLI1 transcription factors that are involved in cell growth and proliferation. Distractors Each answer choice is a gene which when defective leads to a disorder or syndrome with an increased risk of skin cancer. Distractors TYR encodes for the enzyme tyrosinase which is mutated in Oculocutaneous albinism type 1. These patients have white hair, white or pink skin with the inability to tan, and translucent eyes. All types of skin malignancies occur with an increased frequency in OCA type 1, with squamous cell carcinoma being the most prevalent. Distractors XPA-XPG encode for proteins involved in DNA repair, mutations of which lead to the various phenotypes of xeroderma pigmentosum. These defects in DNA repair lead to hypersensitivity to the damaging effects of ultraviolet radiation. There is a 1000-fold increase in skin cancers in these patients. Distractors BLM / RECQL3 is defective in Bloom syndrome. The gene products are helicases involved in DNA synthesis, and when defective the result is telomere dysfunction and genomic instability. Patients with Bloom syndrome have a high-pitched voice, characteristic facial features, photosensitivity, and a significantly increased risk of cutaneous squamous cell carcinoma. Distractors CDKN2A encodes two proteins (p16INK4A and p14ARF) which are tumor suppressors important for cell cycle inhibition. The loss of these cell cycle suppressors leads to a heritable increased cutaneous melanoma risk. Patients are also at increased risk for pancreatic cancer as well as certain central nervous system tumors. Citations Ranshoff KJ, Jaju PD, Tang JY, et al. Familial skin cancer syndromes: Increased melanoma risk. J Am Acad Dermatol. 74,3: 423-434. Jaju PD, Ranshoff KJ, Tang JY et al. Familial skin cancer syndromes: Increased nonmelanotic skin cancers and extracutaneous tumors.J Am Acad Dermatol. 74,3: 437-451. The 59 year-old male depicted below was evaluated in clinic and a biopsy was performed, confirming the suspected diagnosis. Due to the size and location of the tumor, the Mohs surgeon considered attempting to shrink the tumor medically prior to surgical excision. Side effects that were reviewed with the patient included muscle spasms, hair loss, and taste disturbance. Which of the following medications was discussed? A. Vemurafenib B. Pembrolizumab C. Vismodegib D. Imatinib E. Alemtuzumab The 59 year-old male depicted below was evaluated in clinic and a biopsy was performed, confirming the suspected diagnosis. Due to the size and location of the tumor, the Mohs surgeon considered attempting to shrink the tumor medically prior to surgical excision. Side effects that were reviewed with the patient included muscle spasms, hair loss, and taste disturbance. Which of the following medications was discussed? A. Vemurafenib B. Pembrolizumab C. Vismodegib D. Imatinib E. Alemtuzumab The 59 year-old male depicted below was evaluated in clinic and a biopsy was performed, confirming the suspected diagnosis. Due to the size and location of the tumor, the Mohs surgeon considered attempting to shrink the tumor medically prior to surgical excision. Side effects that were reviewed with the patient included muscle spasms, hair loss, and taste disturbance. Which of the following medications was discussed? A. Vemurafenib B. Pembrolizumab C. Vismodegib D. Imatinib E. Alemtuzumab C. Vismodegib The diagnosis is basal cell carcinoma, which is extensively involving the lower eyelid and medial canthus. The gold standard for treatment is surgical excision, preferably Mohs surgery due to its high cure rate and tissue sparing abilities. However, because of the possible functional impairment and cosmetic disfigurement that surgery may present in this case, treatment with Vismodegib could be considered. C. Vismodegib Aberrant Hedgehog pathway signaling due to genetic alterations play a vital role in the pathogenesis and progression of basal cell carcinoma. Vismodegib is a small-molecule inhibitor of the Hedgehog pathway. It has been approved by the FDA for treatment of adults with metastatic BCC or locally advanced BCC that recurred after surgical treatment or for patients who are not candidates for surgery or radiation. The most common side effects of vismodegib therapy are muscle spasms, dysgeusia, and alopecia. Some patients also experience weight loss, nausea, fatigue, decreased appetite, or diarrhea. Neoadjuvant vismodegib has been shown to reduce basal cell carcinoma surgical defect area by 31% if used for at least 3 months. Therefore, neoadjuvant vismodegib could be considered for large basal cell carcinomas in functionally and cosmetically sensitive locations. Distractors Each of the other answer choices is a targeted therapy that is utilized in cutaneous oncology: Distractors Vemurafenib – Used in metastatic melanoma harboring the BRAF V600E mutation, seen in approximately 50% of all melanomas. – Selectively inhibits the mutated BRAF V600E kinase. This reduces signaling through the aberrant mitogen-activated protein kinase (MAP kinase) pathway. Distractors Pembrolizumab – Highly selective monoclonal antibody against programmed cell death protein 1 (PD-1). – PD-1 and its ligands play a major role in regulating immune response through various mechanisms. When abnormally expressed by tumor cells and lymphocytes in the microenvironment, immune evasion by cancer cells can occur. – Blockade of the abnormal pathway results in tumor growth suppression and decreased metastasis. – Pembrolizumab has been effective in treating advanced melanoma. Distractors Imatinib mesylate – Protein-tyrosine kinase inhibitor that inhibits the BCR-ABL tyrosine kinase. – Also has affect against platelet-derived growth factor (PDGF) and stem cell factor (SCF), c-kit, and inhibits PDGF- and SCFmediated cellular events. – It can be used in cutaneous oncology for the treatment of dermatofibrosarcoma protuberans (DFSP) which is characterized by specific chromosomal abnormalities involving the platelet derived growth factor B locus (amplified t(17; 22) translocation or a linear unbalanced t(17; 22) containing the COL1A1 –PDGFB fusion gene is present). Distractors Alemtuzumab – Humanized monoclonal antibody against the CD52 surface antigen on multiple immune cells, including T and B lymphocytes. – Its use results in the cells harboring the antigen to be depleted from the blood via antibody dependent cellular cytotoxicity. – Initially approved for chronic lymphocytic leukemia (CLL) but is also often effective in erythrodermic mycosis fungoides / Sezary Syndrome due to depletion of central memory T cells that predominate in Sezary Syndrome. Citations Sekulic A, Migden MR, Lewis K, et al. Pivotal ERIVANCE basal cell carcinoma (BCC) study: 12-month update of efficacy and safety of vismodegib in advanced BCC. J Am Acad Dermatol. 72,6: 1021–1026. Ally MS, Aasi S, Wysong A, et al. An investigator open-label clinical trial of vismodegib as a neoadjuvant to surgery for high-risk basal cell carcinoma. 71,5: 904– 911. Sharma A, Shah SR, Illum H, et al. Vemurafenib: targeted inhibition of mutated BRAF for treatment of advanced melanoma and its potential in other malignancies. Drugs. 3;72(17):2207-22. McDermott J, Jimeno A. Pembrolizumab: PD-1 ihibition as a therapeutic strategy in cancer. Drugs Today. 51;1: 7-20. Labropoulos SF, Razis ED. Imatinib in the treatment of dermatofibrosarcoma protuberans. Biologics. 1;4: 347-353. Jawed SI, Myskowski PL, Horwitz S, et al. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sezary syndrome). Par II. Prognosis, management, and future directions. J Am Acad Dermatol. 70;2: 223.e1–223.e17. A 72-year-old male is seen with the following lesion on his left superior forehead. A saucerization biopsy is performed which confirms in situ disease. A staged excision is planned. After an initial excision with 5 mm margins, you receive word from the dermatopathologist that the specimen was positive for in situ disease at the medial margin. Which of the following histopathological features best describe what the dermatopathologist has identified? A. Clusters and single cells within the epidermis with nuclear enlargement with atypia, prominent nucleoli and well-defined ample cytoplasm. Pagetoid scatter is prominent. Immunohistochemistry: CK7+ and CAM 5.2+. B. Poorly circumscribed proliferation of atypical cells with pagetoid scatter. Predominance of individual melanocytes (over nests) which extend along adnexal epithelium, but do not invade into the underlying dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. C. Poorly circumscribed proliferation of atypical cells with pagetoid scatter. Asymmetric nests of cells with large nuclei and occasional mitoses lack maturation as they descend into the dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. D. Full-thickness atypia without maturation in the epidermis that extends along adnexal structures but does not invade into the dermis. Acanthosis, parakeratosis, mitotic figures, and occasional pagetoid scatter are present. Immunohistochemistry: pankeratin+, p53+, MART-1-. E. Epidermal pagetoid scatter overlying lobules of atypical basaloid cell with sebaceous differentiation. The lobules have infiltrative borders, central necrosis, and frequent mitotic figures. Immunohistochemistry: EMA+, adipophilin+. A 72-year-old male is seen with the following lesion on his left superior forehead. A saucerization biopsy is performed which confirms in situ disease. A staged excision is planned. After an initial excision with 5 mm margins, you receive word from the dermatopathologist that the specimen was positive for in situ disease at the medial margin. Which of the following histopathological features best describe what the dermatopathologist has identified? A. Clusters and single cells within the epidermis with nuclear enlargement with atypia, prominent nucleoli and well-defined ample cytoplasm. Pagetoid scatter is prominent. Immunohistochemistry: CK7+ and CAM 5.2+. B. Poorly circumscribed proliferation of atypical cells with pagetoid scatter. Predominance of individual melanocytes (over nests) which extend along adnexal epithelium, but do not invade into the underlying dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. C. Poorly circumscribed proliferation of atypical cells with pagetoid scatter. Asymmetric nests of cells with large nuclei and occasional mitoses lack maturation as they descend into the dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. D. Full-thickness atypia without maturation in the epidermis that extends along adnexal structures but does not invade into the dermis. Acanthosis, parakeratosis, mitotic figures, and occasional pagetoid scatter are present. Immunohistochemistry: pankeratin+, p53+, MART-1-. E. Epidermal pagetoid scatter overlying lobules of atypical basaloid cell with sebaceous differentiation. The lobules have infiltrative borders, central necrosis, and frequent mitotic figures. Immunohistochemistry: EMA+, adipophilin+. A 72-year-old male is seen with the following lesion on his left superior forehead. A saucerization biopsy is performed which confirms in situ disease. A staged excision is planned. After an initial excision with 5 mm margins, you receive word from the dermatopathologist that the specimen was positive for in situ disease at the medial margin. Which of the following histopathological features best describe what the dermatopathologist has identified? A. Clusters and single cells within the epidermis with nuclear enlargement with atypia, prominent nucleoli and well-defined ample cytoplasm. Pagetoid scatter is prominent. Immunohistochemistry: CK7+ and CAM 5.2+. B. Poorly circumscribed proliferation of atypical cells with pagetoid scatter. Predominance of individual melanocytes (over nests) which extend along adnexal epithelium, but do not invade into the underlying dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. C. Poorly circumscribed proliferation of atypical cells with pagetoid scatter. Asymmetric nests of cells with large nuclei and occasional mitoses lack maturation as they descend into the dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. D. Full-thickness atypia without maturation in the epidermis that extends along adnexal structures but does not invade into the dermis. Acanthosis, parakeratosis, mitotic figures, and occasional pagetoid scatter are present. Immunohistochemistry: pankeratin+, p53+, MART-1-. E. Epidermal pagetoid scatter overlying lobules of atypical basaloid cell with sebaceous differentiation. The lobules have infiltrative borders, central necrosis, and frequent mitotic figures. Immunohistochemistry: EMA+, adipophilin+. Correct Answer: B The image and associated description depict melanoma in situ. The histopathology of melanoma in situ reveals a poorly circumscribed proliferation of atypical cells with pagetoid scatter. There is a predominance of individual melanocytes (over nests) which extend along adnexal epithelium, but do not invade into the underlying dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. Distractors All other answer choices describe the histopathology of other tumors that can have pagetoid spread in the epidermis. Distractors Answer choice A describes Paget’s Disease / Extramammary Paget’s Disease – Clusters and single cells within the epidermis with nuclear enlargement with atypia, prominent nucleoli and well-defined ample cytoplasm. Pagetoid scatter is prominent. Immunohistochemistry: CK7+ and CAM 5.2+. Distractors Answer choice C describes invasive melanoma – Poorly circumscribed proliferation of atypical cells with pagetoid scatter. Asymmetric nests of cells with large nuclei and occasional mitoses lack maturation as they descend into the dermis. Immunohistochemistry: S100+, HMB45+, MART-1+. Distractors Answer choice D describes squamous cell carcinoma in situ (Bowen’s Disease) – Full-thickness atypia without maturation in the epidermis that extends along adnexal structures but does not invade into the dermis. Acanthosis, parakeratosis, mitotic figures, and occasional pagetoid scatter are present. Immunohistochemistry: pankeratin+, p53+, MART-1-. Distractors Answer choice E describes sebaceous carcinoma – Epidermal pagetoid scatter overlying lobules of atypical basaloid cell with sebaceous differentiation. The lobules have infiltrative borders, central necrosis, and frequent mitotic figures. Immunohistochemistry: EMA+, adipophilin+. Citations Higgins HW, Lee KC, Galan A, et al. Melanoma in situ: Part I. Epidemiology, screening, and clinical features. J Am Acad Dermatol. 73,2:181-190. Higgins HW, Lee KC, Galan A, et al. Melanoma in situ: Part 2. Histopathology, treatment, and clinical management . J Am Acad Dermatol. 73,2:193-203. Cassarino DS, DeRienzo DP, Barr RJ. Cutaneous squamous cell carcinoma: a comprehensive clinicopathologic classification – part one. J Cutaneous Pathology. 33,3:191-206. Lopes LL, Lopes IM, Lopes LR, et al. Mammary and extramammary Paget’s disease. An Bras Dermatol. 90,2:225-231. Ansai S, Hashimoto H, Aoki T, et al. A histochemical and immunohistochemical study of extra-ocular sebaceous carcinoma. Histopathology. 22,2: 127-134. http://idsblinck.blogspot.co.uk/2009_11_01_archive.html A 62 year-old male presented with the tumor shown below on the right lower lip. A biopsy confirmed squamous cell carcinoma. Which of the following characteristics is not considered a high risk tumor feature that affects staging of cutaneous SCC according to the most recent American Joint Committee on Cancer Staging Manual (Seventh Edition)? A. History of kidney transplant B. Perineural invasion C. Location on lip D. Depth of invasion > 2mm E. Poorly differentiated histology A 62 year-old male presented with the tumor shown below on the right lower lip. A biopsy confirmed squamous cell carcinoma. Which of the following characteristics is not considered a high risk tumor feature that affects staging of cutaneous SCC according to the most recent American Joint Committee on Cancer Staging Manual (Seventh Edition)? A. History of kidney transplant B. Perineural invasion C. Location on lip D. Depth of invasion > 2mm E. Poorly differentiated histology A 62 year-old male presented with the tumor shown below on the right lower lip. A biopsy confirmed squamous cell carcinoma. Which of the following characteristics is not considered a high risk tumor feature that affects staging of cutaneous SCC according to the most recent American Joint Committee on Cancer Staging Manual (Seventh Edition)? A. History of kidney transplant B. Perineural invasion C. Location on lip D. Depth of invasion > 2mm E. Poorly differentiated histology A. History of kidney transplant Cutaneous squamous cell carcinoma can be locally invasive, but also has the potential to metastasize to regional lymph nodes or distant organs. It is the leading cause of death among skin cancer, which is often a result of uncontrolled regional disease. A. History of kidney transplant Various staging schemes for cutaneous SCC have been developed. The most recent proposed by the American Joint Committee on Cancer (Cancer Staging Manual, 7th edition) identifies the following characteristics of the tumor as high risk features: – depth/invasion > 2mm thickness – Clark level ≥ IV – perineural invasion – anatomic location (primary site ear, primary site lip) – differentiation (poorly differentiated or undifferentiated). A. History of kidney transplant Immunosuppression (such as solid organ transplantation and history of CLL) was acknowledged as being associated with worse outcome, but it does not alter the staging scheme as presented by the AJCC. This was done because strict TNM criteria preclude inclusion of extra-tumoral clinical risk factors in the staging system. Tumor recurrence is another factor associated with an increased risk of nodal metastasis but was not included in the AJCC-7. The National Comprehensive Cancer Network (NCCN Clinical Practice Guidelines in Oncology) has recently identified a more extensive list of high risk features that should be considered when evaluating and treating potentially high-risk cutaneous squamous cell carcinoma. Citations Farasat S, Yu SS, Neel VA, et al. A new American Joint Committee on Cancer staging system for cutaneous squamous cell carcinoma: Creation and rationale for inclusion of tumor (T) characteristics. J Am Acad Dermatol. 64;6: 1051-1059. Navarrete-Dechent C, Vaness MJ, Droppelmann N, et al. High-risk cutaneous squamous cell carcinoma and the emerging role of sentinel lymph node biopsy: A literature review. J Am Acad Dermatol. 73;1: 127–137. Nuno-Gonzalez A, Vicente-Martin FJ, Pinedo-Moraleda F, et al. Review: High Risk Squamous Cell Carcinoma. Actas Dermosifiliogr. 103;7: 567-578. You are treating a 64 year-old female for the two large basal cell carcinomas shown below. She weighs 68 kg. It has been challenging to maintain adequate anesthesia and you have frequently had to inject more 1% lidocaine with epinephrine (1:100,000) throughout the procedures. You have injected a total of 48 mL of the local anesthetic when the patient begins to complain of numbness around her mouth and facial tingling. You suspect early signs of lidocaine toxicity. What is the recommended safe maximum adult dose of lidocaine with epinephrine in dermatologic surgery? A. 2.0 mg/kg B. 3.0 mg/kg C. 4.5 mg/kg D. 7 mg/kg E. 55 mg/kg You are treating a 64 year-old female for the two large basal cell carcinomas shown below. She weighs 68 kg. It has been challenging to maintain adequate anesthesia and you have frequently had to inject more 1% lidocaine with epinephrine (1:100,000) throughout the procedures. You have injected a total of 48 mL of the local anesthetic when the patient begins to complain of numbness around her mouth and facial tingling. You suspect early signs of lidocaine toxicity. What is the recommended safe maximum adult dose of lidocaine with epinephrine in dermatologic surgery? A. 2.0 mg/kg B. 3.0 mg/kg C. 4.5 mg/kg D. 7 mg/kg E. 55 mg/kg You are treating a 64 year-old female for the two large basal cell carcinomas shown below. She weighs 68 kg. It has been challenging to maintain adequate anesthesia and you have frequently had to inject more 1% lidocaine with epinephrine (1:100,000) throughout the procedures. You have injected a total of 48 mL of the local anesthetic when the patient begins to complain of numbness around her mouth and facial tingling. You suspect early signs of lidocaine toxicity. What is the recommended safe maximum adult dose of lidocaine with epinephrine in dermatologic surgery? A. 2.0 mg/kg B. 3.0 mg/kg C. 4.5 mg/kg D. 7 mg/kg E. 55 mg/kg D. 7 mg/kg The manufacturer maximum recommended dose in adults is 7 mg/kg of lidocaine with epinephrine or 4.5 mg/kg of lidocaine without epinephrine. For children, the recommended maximum dose is 3.0-4.5 mg/kg of lidocaine with epinephrine or 1.5-2.0 mg/kg of lidocaine without epinephrine. For tumescent local anesthesia as used for office-based liposuction, a total lidocaine dose of 55 mg/kg has been shown to be safe. D. 7 mg/kg Local anesthetic systemic toxicity (LAST) is manifested by a progression of central nervous system excitement. – The first symtpoms a patient experiences are often circumoral numbness and facial tingling. – This can be followed by slurred speech, metallic taste, auditory changes, and hallucinations. – Hypertension and tachycardia may also be present. – Severe toxicity can lead to seizures or central nervous system depression, and the end-stage of a severe case is cardiac failure or arrest. Citations Kouba DJ, LoPiccolo MC, Alam M, et al. Guidelines for the use of local anesthesia in office-based dermatologic surgery. J Am Acad Dermatol. 74;6: 1201–1219. Alam M, Ricci D, Havey J, et al. Safety of peak serum lidocaine concentration after Mohs micrographic surgery: A prospecrtive cohort study. J Am Acad Dermatol. 63;1: 87–92.