Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
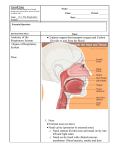
By the Name of Allah Sheet 1 embryology Development of the nose: The doc. talked in brief about the development of the face: During the 5th week: The face is formed mainly from the fusion of several processes from the 1st arches: 1. the frontonasal process: *from the frontal bon to the nose * In the lower edge of the frontonasal process we can find the olfactory pit (appears as depressions in the lower edge) * It (the olfactory pit) divides the frontonasal process into a medial nasal process and two lateral nasal processes 2. the maxillary processes: (Grow medially and fuse with the lateral and medial nasal processes) 3. the mandibular process Under these three processes we can find the 2nd pharyngeal arches During the 5.5th week: 1. the frontonasal process descends downward and gives the med. Nasal process witch forms the tip of the nose in the mid line (med. to the olfactory pits ) 2. the lat. Nasal processes (lat. to the olfactory pits ) form the lat. Wall of the nose 1 during the 6.5th week : We can see the olfactory pits bounded medially by the med. Nasal process, laterally by the lat. nasal processes and inferiorly by the maxillary processes They (med., lat. and maxillary processes) fuse together to form the nostrils. Note: as these processes fuse, the olfactory pits become deeper and form welldefined blind sacs. We can also see the philtrum in the roof of the oral cavity?! (The medial nasal process forms philtrum of the upper lip) Development of the nose: the roof of the nose is formed from: lat. nasal processes ( it also form the lat. wall) maxillary process formation of the nostrils and the vestibule: as we said the olfactory pits become deeper and form blind sacs that form the vestibule internally . the opening into each of which is the nostril the floor of the nose at first is very short and formed by: med. nasal process (it also forms the nasal septum) and the maxillary process on each side Notes: (The floor of the olfactory pits rupture so...) the nasal cavity communicate with the oral cavity The nasal septum is formed as a downgrowth from the med. nasal process … remember that it is the perpendicular palate of the ethmoidal bone Then the palatal processes of the maxilla grow medially and fuse with each other and with the nasal septum, thus completing the floor of the nose Lat. wall invaginations form the conchae (sup., med. and inf.) Development of the palate: The growth of the palatal process of the maxilla from lateral side to the midline fusion of the two palatal processes with the nasal septum thus completing the floor of the nose and separating the nasal cavity from the oral cavity the chonana is formed posteriorly which communicates the nasal cavity with the nasopharynx 2 the hard palate is formed by the fusion of: *the 1ry palate: formed by medial nasal process *the 2ry (lat.) palate: formed by the fusion of: the 2 palatal processes of maxilla So… The 2ry palate fuses with the 1ry palate forming the hard palate and the incisive foramen after that the 2 edges of the 2ry palate elongate -backward and to the midlineforming the soft palate (the 2 edges fuse together during the 8th week) and the uvula (during the 11th week ) so… the floor of the nose 1) it separates the oral cavity from the nasal cavity 2)and it forms the 2 lat. cavities of the nose (with the nasal septum in the middle) Anomalies: Cleft palate: A congenital fissure in the roof of the mouth, resulting from incomplete fusion of the palate (if the fusion was not on the midline) during embryonic development, It may be unilateral or bilateral, it may be partial or complete (it may extend through the entire palate) 3 Development of the paranasel sinuses: Develops as diverticula (pouch like growth) of the lateral wall and extend in the maxilla, ethmoid, frontal and sphenoid bones to form their sinuses So it causes invagination to the lateral wall to form the paranasel sinuses At birth these sinuses are rudimentary They reach their maximum size at puberty Enlargement of the air sinuses participates in the development of the face esp. the maxillary and frontal air sinuses (I'm not sure about the two sinuses!!) So… the paranasel air sinuses contribute to the definitive shape of the face and most of them reach their normal size at puberty General notes: The lower respiratory system begins to develop during the 4th week as an outgrowth of the ventral wall of the foregut named the respiratory diverticulum. So the 1st thing to appear is the respiratory diverticulum (aka lung buds) from the ant. Wall (ventral wall) *Foregut → floor of the pharynx (ventral wall) → respiratory diverticulum Note that: 1. the lining epithelium of the larynx, trachea, bronchi and lung tissues are endodermal in origin 2. while the cartilage, muscles, C.T, and blood vessels are mesodermal in origin ( from splanchnic mesoderm) 3. the 2 layers of mesoderm: 1) splanchnic 2) Somatic layer ()جدارية: that forms the parietal pleura… Separation of the trachea and esophagus: A. The foregut (particularly the esophagus) is Post. To the lung buds B. At first the respiratory diverticulum communicate with the foregut C. After that the esophageotracheal ridges are formed → then they (the ridges) fuse with each other → and form esophageotracheal septum that constricts and completely separates the trachea and lung buds (ant. ) from the esophagus (pst.) 4 *Note that the laryngeal orifice maintains the communication between the resp. premordium and the floor of the larynx *at this stage many abnormalities might occur, such as atresia and fistula: Esophageal atresia: complete blockage of the esophagus Tracheoesophgeal fistula: track between the two cavities Prevalence: 1/3000 A) 90% of the cases Proximal: Complete blockage of the esophagus Distal: Tracheoesophgeal fistula It causes continues vomiting Particles and secretions of the GIT may reach the lungs causing inflammation and pneumonia B) 4 % of the cases Complete blockage i.e. no fistula C) two communications proximal and distal with one opining D) the most dangerous case Proximal: fistula Distal: atresia All the food enters to the lungs!! E) two fistula with two openings 33% of these abnormalities are associated with other abnormalities Mainly cardiac anomalies: such as ASD, VSD and tetralogy of fallot Other abnormalities: anal atresia, renal or lymph defects Complications: *polyhydraminios: the presence of excessive amount of amniotic fluid (Extra info. :oligohydramnios: a deficiency in the amount of amniotic fluid) *pneumonia after birth *when the baby cries his/her stomach distends 5 Development of the larynx: We have 6 pharyngeal arches, the 5th disappears The lining epithelial of the larynx develops from the endoderm And the cartilages (Thyroid, Cricoid and arytenoid) are formed from the 4th and 6th mesenchyma of the arches The laryngeal orifice at the beginning is a slit line shaped opening (6th week) after that it changes its shape into T like opining then at the age of 12th week it takes its final shape These changes are due to rapid proliferation of the mesenchyma The rapid proliferation of the lining epithelium result in temporary occlusion of the laryngeal lumen So… the laryngeal lumen initially is obstructed by membranous material however, canalization and vacuolization occur after that Vacuolization and re canalization of these membranes cause them to go laterally and produce pair of laryngeal ventricles(recesses) that are bounded by folds of tissue that differentiate into false and true vocal cords *above: false vocal cord *bellow: true vocal cord *vocal fold: membrane and ligaments So… the true and false vocal folds are formed from the membranes that were causing larynx obstruction The innervations of laryngeal muscles and mucosa follow their embryological origin (whether they come from the 4th or the 6th pharyngeal arches 1. superior laryngeal nerve is associated with the 4th pharyngeal arches and it innervates the cricothyroid muscle and the mucosa above the vocal cords 2. recurrent laryngeal nerve is associated with the 6th pharyngeal arches and it innervates all the muscles of the larynx and the mucosa below the vocal cords 6 Development of the trachea and bronchi: 1. The laryngotracheal tube descends downward to form the trachea Distally it divides into Rt. and Lt. lung buds at the level of T4 2. two out-pocketing of lung buds form the bronchial buds which form the Rt. and Lt. main bronchi 3. the Rt. main bronchus forms 3 2ry bronchi and the Lt. forms 2 2ry bronchi (The # of the 2ry bronchi on each side is according to the # of lung lobes) Note: The two lung buds are not symmetrical the different is related to the genes responsible for the structure of each bronchus 4. The 2ry bronchus divides repeatedly in dichotomous fashion forming 3ry bronchi that create broncho - pulmonary segments *Dichotomous fashion: it divides into two parts repeatedly I.e. 2 → 4 → 8 … *10 3ry bronchi in the R. lung and 8 in the left lung 5. by the end of the 6th month … 17 generations of subdivisions are formed 6. additional 6 divisions are formed postnataly So… the total # of divisions is 23 divisions which form bronchioles and alveoli Development of the lungs, viscera and pleura: 7 A) pericardio-peritoneal canal→ plural cavity B) trachea C) splanchnich mesoderm → visceral pleura D) lung bud E) somatic mesoderm → parietal pleura 1. At the beginning we have coelomic cavities that union into on cavity 2. This coelomic cavity forms all the body cavities (pericardial, peritoneal and pleura) 3. This cavity will develop into pericardio-peritoneal cavity 4. When the diaphragm develops it separates the pericardio-peritoneal cavity into pericardio-peritoneal and peritoneal cavities 5. Finally, the pericardio-peritoneal canal will form the pleura and the pericardium Due to the expansion and invagination of the lung buds into the pleural cavity (A) … the lung buds will be covered by the visceral pleura (C) … and the outer layer will form the parietal pleura (E) that lines the thoracic wall The plural cavity is formed by: Continues enlargement of the lung buds (y3nee: the plural fluid is the only thing that separate the visceral pleura (C) from the parietal pleura (E) Note that: The visceral pleura is derived from the splanchnich mesoderm The parietal pleura is derived from the somatic mesoderm The plural cavity is between these two layers The plural is divided in to : cervical, costal, mediastinal and diaphragmatic pleura 8 Innervations of the pleura: The phrenic nerve descends through the middle mediastinum –between the two lungs- it descends downward then laterally So.. the phrenic nerve: 1. from C3, C4 and C5 2. it innervates the mediastinal and diaphragmatic pleura 3. it has two parts : a. motor: to the diaphragm b. and sensory: to the parital plura costal and cervical pleura are innervated segmentally by the inter costal nerves the visceral is innervated by autonomic nervous system The end Happy Islamic Year Mira N. Al-Jabi 9