Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Prescription costs wikipedia , lookup
Theralizumab wikipedia , lookup
Electronic prescribing wikipedia , lookup
Pharmacogenomics wikipedia , lookup
National Institute for Health and Care Excellence wikipedia , lookup
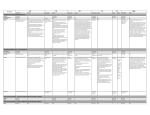
Gwent Shared Care Protocol METHYLPHENIDATE for the treatment of Attention Deficit/Hyperactivity Disorder (ADHD) Protocol No. 10 PLEASE CHECK http://www.wales.nhs.uk/sites3/page.cfm?orgid=284&pid=5988 FOR THE LATEST VERSION OF THIS PROTOCOL General guidance The Gwent Partnership Medicines and Therapeutics Committee endorsed this protocol in 2005. It outlines shared care arrangements for patients taking methylphenidate for the treatment of Attention Deficit / Hyperactivity Disorder (ADHD). This Protocol does NOT cover the use of: 1. methylphenidate in narcolepsy (‘off label’ use). 2. methylphenidate at doses above the maximum recommended in ADHD. 3. Medikinet XL® in ADHD (non Formulary preparation). This Protocol should be read in conjunction with: The Shared Care Agreement Form (see Page 7). “Guidelines for the Assessment & Management of Attention Control problems” NICE TA98 Methylphenidate, atomoxetine and dexamfetamine for attention deficit hyperactivity disorder (ADHD) in children and adolescents - guidance of March 2006 see: http://www.nice.org.uk/page.aspx?o=TA098guidance NICE CG72 (September 2008 last modified March 2013 http://guidance.nice.org.uk/CG72) – Attention deficit hyperactivity disorder: Diagnosis and management of ADHD in children, young people and adults. Note CG72 incorporates recommendations from NICE TA98 and TA102. The Summary of Product Characteristics for Ritalin®, Concerta XL® or Equasym XL® see: http://www.medicines.org.uk/ 1. Licensed indication Methylphenidate is indicated as a part of a comprehensive treatment programme for ADHD in children, adolescents and adults when remedial measures alone prove insufficient. Treatment must be initiated under the supervision of an appropriate specialist (paediatrician or psychiatrist) in behavioural and emotional disorders. Diagnosis should be made according to DSM-IV criteria or the guidelines in ICD-10 and should be based on a complete history and evaluation of the patient. Diagnosis cannot be made solely on the presence of one or more symptom. The specific aetiology of this syndrome is unknown, and there is no single diagnostic test. Adequate diagnosis requires the use of medical and specialised psychological, educational and social resources. A comprehensive treatment programme, typically includes psychological, educational and social measures as well as pharmacotherapy and is aimed at stabilising children with a behavioural syndrome characterised by symptoms which may include chronic history of short attention span, distractibility, emotional lability, impulsivity, moderate to severe hyperactivity, minor neurological signs and abnormal EEG. Learning may or may not be impaired. Methylphenidate treatment is not indicated in all children with this syndrome and the decision to use the drug must be based on a very thorough assessment of the severity and the chronicity of the child's symptoms in relation to the child's age. Appropriate educational placement is essential, and psychosocial intervention is generally necessary. Where remedial measures alone prove insufficient, the decision to prescribe a stimulant must be based on rigorous assessment of the severity of the child's symptoms. The use of methylphenidate should always be used in the way according to the licensed indication and according to the prescribing/diagnostics guidelines. 2. Background information The decision to control behaviour through the use of medication is and indeed should be a difficult one. It has, however, been shown that the symptoms of ADHD can, in a large proportion of cases (up to 70%) be improved by the use of stimulant medication. The medication works by stimulating inhibitory mechanisms in the brain, thereby, controlling This Shared Care Protocol should be read in conjunction with the Summary of Product Characteristics Status: APPROVED Issue Date: July 2005 (Updated Dec. 2011 & Jan. 2014) Approved by: GPMTC 27th July 2005 Page 1 of 7 Review Date: January 2015 impulsiveness and enabling the child to attend and concentrate. This enables parents, teachers and child to regain control of the behaviour through psychosocial, behavioural and educational strategies that run in parallel. Stimulant medication has been in use since the 1950s and experience indicates that the benefits usually outweigh the problems that may arise. It is essential that proper monitoring occurs. 3. Contraindications & Cautions Methylphenidate is contraindicated in: Known sensitivity to methylphenidate or to any of the excipients. Glaucoma. Phaeochromocytoma. During treatment with non-selective, irreversible monoamine oxidase (MAO) inhibitors, or within a minimum of 14 days of discontinuing those drugs, due to risk of hypertensive crisis. Hyperthyroidism or thyrotoxicosis. Diagnosis or history of severe depression, anorexia nervosa/anorexic disorders, suicidal tendencies, psychotic symptoms, severe mood disorders, mania, schizophrenia, psychopathic/borderline personality disorder. Diagnosis or history of severe and episodic (Type 1) Bipolar (affective) disorder (that is not well controlled). Pre-existing cardiovascular disorders including severe hypertension, heart failure, arterial occlusive disease, angina, haemodynamically significant congenital heart disease, cardiomyopathies, myocardial infarction, potentially life-threatening arrhythmias and channelopathies (disorders caused by the dysfunction of ion channels). Pre-existing cerebrovascular disorders cerebral aneurysm, vascular abnormalities including vasculitis or stroke or known risk factors for cerebrovascular disorders Cautions: Children < 6 years and adults – In adolescents whose symptoms persist into adulthood and who have shown clear benefit from treatment, continued treatment into adulthood is now a licensed indication for Concerta XL® (but not Equasym XL® or Ritalin®). NICE CG72 states: Following a decision to start drug treatment in adults with ADHD, methylphenidate should normally be tried first (UNLICENSED use). Abuse – methylphenidate should be used with caution in patients with known drug or alcohol dependency because of a potential for abuse, misuse or diversion (Note careful supervision is required during withdrawal from abusive use since severe depression may occur). Family history of tics or Tourette’s Syndrome – needs careful evaluation before prescribing but is not necessarily an absolute contra-indication. Epilepsy (particularly poorly controlled epilepsy) - Children with well-controlled epilepsy can be considered for careful introduction of methylphenidate however, in all such cases atomoxetine should be considered – see separate Gwent Shared Care Protocol (No 11). Pregnancy – females of child-bearing potential (i.e. post-menarche) should not use methylphenidate unless clearly necessary 4. Dosage regimen a) Methylphenidate immediate release (IR) An initial dose of 5mg twice daily, increasing by 5mg is recommended. If no effect has been seen after one week, an increase from 5mg twice daily by 5mg increments to a maximum dose of 60mg a day is suggested (unless side effects prevent). If there is no significant response by one month then discontinue. Methylphenidate modified release (MR) preparations THESE SHOULD NOT BE ROUTINELY GIVEN AS FIRST LINE TREATMENT AND PRESCRIBERS SHOULD BE FAMILIAR WITH THE DIFFERENCES IN THEIR PHARMACOKINETIC PROFILES. NICE CG72 states: When prescribing methylphenidate for the treatment of children or young people, MR preparations should be considered for the following reasons: convenience improving adherence This Shared Care Protocol should be read in conjunction with the Summary of Product Characteristics Status: APPROVED Issue Date: July 2005 (Updated Dec. 2011 & Jan. 2014) Approved by: GPMTC 27th July 2005 Page 2 of 7 Review Date: January 2015 reducing stigma (because the child or young person does not need to take medication at school) reducing problems schools have in storing and administering controlled drugs their pharmacokinetic profiles. ABHB MTC advice is that MR methylphenidate should be used only in exceptional circumstances where the supervising clinician has clear evidence that administration of a midday dose is problematic or inappropriate. b) Concerta XL® tablets (oral administration) Treatment should be initiated at a dose of 18mg once daily (in the morning), and increased if necessary up to a maximum of 54mg once daily In Concerta XL the methylphenidate is contained within a non-absorbable shell designed to release the drug at a controlled rate. Following oral administration of Concerta XL® to adults the drug overcoat dissolves, providing an initial maximum drug concentration at about 1 to 2 hours. The methylphenidate contained in the two internal drug layers is gradually released over the next several hours. Peak plasma concentrations are achieved at about 6 to 8 hours, after which plasma levels of methylphenidate gradually decrease The tablet shell is eliminated from the body; patients should not be concerned if they occasionally notice in their stool something that looks like a tablet. There have been rare reports of obstructive symptoms in patients with known strictures in association with the ingestion of drugs in non-deformable MR formulations. b) Equasym XL® capsules (oral administration) The recommended dose is 10mg once daily initially, increased if necessary to a maximum of 60mg once daily. Equasym XL delivers therapeutic plasma levels for a period of approximately 8 hours (i.e. consistent with the school day rather than the whole day). Equasym XL has a plasma profile showing two phases of active substance release, with a sharp, initial, upward slope similar to a methylphenidate IR tablet, and a second rising portion approximately three hours later, followed by a gradual decline. The second phase of release resulted in a second maximum observed concentration in most subjects at 4.5 hours after dosing Administration of an MR formulation at breakfast instead of two IR formulation tablets (breakfast and lunch) may reduce the pre-lunch trough and post lunch peak of methylphenidate, and plasma levels may be lower after the end of the school day. Concerta XL® and Equasym XL® compared: Name Concerta XL® Equasym XL® Product details Modifie d release 10-12 hours duration Strengths Formulation 18mg 27mg 36mg 54mg Modifie d release Up to 8 hours duration 10mg 20mg 30mg Capsule shaped tablet containing two layers of drug separated by semipermeable membrane Outer layer (overcoat) released first followed by gradual release of drug from inner core. Empty tablet shell excreted. Capsule containing two types of pellets/beads which allow immediate release of drug, followed by gradual release over the day. Dose equivalent: 18mg = 5mg IR tds 36mg = 10mg IR tds 54mg = 15mg IR tds Release profiles 22% IR: 78% MR Initial peak plasma concentratio n in 1-2 hours. Second peak at 6-8 hours Administration details Tablet must be swallowed whole, not chewed crushed or broken 30% IR: 70% MR Initial peak plasma concentratio n in 1-2 hours. Second peak at 4.5 hours Capsules may be opened and contents mixed with soft foods. (stability unknown) Contents must be swallowed not chewed crushed or broken This Shared Care Protocol should be read in conjunction with the Summary of Product Characteristics Status: APPROVED Issue Date: July 2005 (Updated Dec. 2011 & Jan. 2014) Approved by: GPMTC 27th July 2005 Page 3 of 7 Review Date: January 2015 Note: In adolescents whose symptoms persist into adulthood and who have shown clear benefit from treatment, continued treatment into adulthood is now a licensed indication for Concerta XL® (but not Equasym XL®). Although recommended by NICE CG72, initiation of ADHD treatment with any formulation of methylphenidate (including Concerta XL®) in adults remains an UNLICENSED use. 5. Drug Interactions Check BNF Appendix 1 (sympathomimetics) before co-prescribing any other drug. 6. Adverse drug reactions All serious adverse events should be reported to MHRA/CHM using the Yellow Card . Anticoagulants – Methylphenidate may enhance anticoagulant effect of warfarin and other coumarins. Antidepressants – Methylphenidate may inhibit metabolism of SSRI’s and tricyclics, coadministration with MAOI’s may cause hypertensive crisis. Antiepileptics – Methylphenidate increases plasma level of phenytoin and possibly phenobarbitone and primidone. Antihypertensives – serious adverse events reported with concomitant methylphenidate. Adverse event by reported frequency Loss of appetite (common ≥1/100 to <1/10) Indigestion, reflux or nausea (common ≥1/100 to <1/10) Headaches (very common ≥ 1/10) Dizziness (common ≥1/100 to <1/10) Mood or personality changes (common ≥1/100 to <1/10) Insomnia (very common) Emergent suicidal ideation or behaviour during treatment (uncommon ≥1/1000 to <1/100) Onset or exacerbation of motor and verbal tics (uncommon ≥1/1000 to <1/100) Palpitations (common ≥1/100 to <1/10), exertional chest pain (uncommon ≥1/1000 to <1/100), unexplained syncope, dyspnoea, or other symptoms suggestive of heart disease Management Can be limited by taking with meals and by giving drug holidays wherever possible. If growth should halt for more than 6 months then medication must be discontinued and, if after two months, growth does not proceed then Paediatric investigation is required. Can be limited by taking with meals. May occur initially and then stop. If not transient, alternative brands may be more effective and if symptoms persist off medication then full Paediatric examination to exclude other pathology should be carried out. Usually occur after long-term, high dose usage. Can be resolved by ensuring the last daily dose is taken at least 4 hours prior to bed time. Occasionally ADHD can impair sleep and an evening dose can improve sleep. Immediate specialist evaluation required. Stop methylphenidate and discuss with specialist. Prompt specialist cardiac evaluation required. Careful supervision is required during withdrawal, since this may unmask depression as well as chronic over-activity. Some patients may require long-term follow-up. 7. Baseline investigations To be undertaken by specialist: A complete history should be taken, documenting: concomitant medicines; past and present medical and psychiatric disorders or symptoms; family history of sudden cardiac death, unexplained death, or malignant arrhythmia; and accurate pre-treatment height and weight on a growth chart (adult patients should have their BMI recorded). i) Physical examination for the presence of heart disease (including BP and pulse). The use of methylphenidate is contraindicated in certain pre-existing cardiovascular disorders (see section 3 above) unless specialist paediatric cardiac advice has been obtained. ii) Assessment for co-existence of psychiatric and depressive disorders, as well as anxiety, agitation or tension, should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression. iii) Assessment for co-existence of tics or Tourette's syndrome, including a family history. This Shared Care Protocol should be read in conjunction with the Summary of Product Characteristics Status: APPROVED Issue Date: July 2005 (Updated Dec. 2011 & Jan. 2014) Approved by: GPMTC 27th July 2005 Page 4 of 7 Review Date: January 2015 8. Ongoing monitoring To be undertaken by specialist: i) Height and weight and appetite (with maintenance of a growth chart) – at least six monthly. For adult patients a record of the patient’s BMI should be kept. ii) BP and pulse (recorded on a centile chart) – at least six-monthly. iii) Emergence or worsening of psychiatric and depressive disorders as well as anxiety, agitation, tension or aggressive behaviour – at least six-monthly. iv) Onset or exacerbation of motor and verbal tics – at least six-monthly. 9. Specialist contact details Advice can be obtained from the local Child Psychiatry, Adult Psychiatry and Community Paediatric Services from 9 to 5pm Monday to Friday Child psychiatry: 01633 436830 Learning Disabilities: Community Paediatrics: 01633 436831 01633 623553 via responsible Consultant 01633 436832 Secretary 01633 436944 Adult psychiatry: contact local General Adult Community Mental Health Team see: http://howis.wales.nhs.uk/sitesplus/866/page/52574 10. Criteria for shared care All Wales criteria for Shared Care can be found at: http://www.awmsg.org/docs/awmsg/medman/Criteria%20for%20Shared%20Care.pdf GMC guidance on Shared Care (2013) states: Decisions about who should take responsibility for continuing care or treatment after initial diagnosis or assessment should be based on the patient’s best interests, rather than on convenience or the cost of the medicine and associated monitoring or follow-up. Shared care requires the agreement of all parties, including the patient. Effective communication and continuing liaison between all parties to a shared care agreement are essential. 11. Responsibilities of Specialists (Secondary Care) i. The assessment & diagnosis of ADHD in accordance with national recommendations in NICE CG72. ii. To undertake the baseline clinical valuations (as detailed in Section 7 above). iii. To provide a patient information leaflet indicating the risks and benefits associated with methylphenidate. iv. To advise the patient/carer on potential side effects and the action to be taken should they occur (particularly development or worsening of anxiety, psychiatric and bipolar symptoms and tics as well as palpitations, exertional chest pain, unexplained syncope, dyspnoea, or other symptoms suggestive of heart disease). v. To confirm patient/carer understanding and consent to treatment. vi. To initiate methylphenidate and change the dose (if required). vii. To prescribe the first 28 days supply of methylphenidate. viii. Following initiation, to send the GP a Shared Care Agreement Form (Page 7) inviting them to participate in shared care management of the patient. ix. To monitor the patient in accordance with the schedule above (Section 7). x. To inform the GP of dosage schedule, monitoring measurements and progress of treatment after each appointment. xi. To inform the GP if the patient fails to attend and clearly indicating that the patient is taking methylphenidate. xii. To re-evaluate the long term usefulness of the drug for the individual patient with trial periods off medication to assess the patient's functioning without pharmacotherapy this should be performed at least once yearly (preferably during times of school holidays). xiii. To ensure that monitoring responsibility is transferred from child to adult services once the patient reaches 18 years of age. xiv. To ensure that the service accepting the care of the patient on reaching adulthood seeks further agreement with GP to continue prescribing preparations of methylyphenidate where an UNLICENSED preparation is required (Equasym XL® and Ritalin®) for continued This Shared Care Protocol should be read in conjunction with the Summary of Product Characteristics Status: APPROVED Issue Date: July 2005 (Updated Dec. 2011 & Jan. 2014) Approved by: GPMTC 27th July 2005 Page 5 of 7 Review Date: January 2015 treatment into adulthood. 12. Responsibilities of patients/carers To attend hospital and GP clinic appointments Failure to attend will result in the medication being stopped. To report any adverse events immediately to their specialist or GP (particularly development or worsening of anxiety, psychiatric and bipolar symptoms and tics as well as palpitations, exertional chest pain, unexplained syncope, dyspnoea, or other symptoms suggestive of heart disease). 13. Responsibilities of Primary Care To return the Shared Care Agreement Form (Page 7) to the requesting specialist within one week of receipt. To issue ongoing prescriptions for methylphenidate as per dose recommended by specialist. To monitor for the risk of diversion, misuse and abuse of methylphenidate and to alert the specialist (Note careful supervision is required during withdrawal from abusive use since severe depression may occur). To contact the patient/carer if they fail to attend appointments with specialist and if necessary refuse to issue further prescriptions until specialist supervision has occurred. Whenever practical, to ask the patient/carer about any adverse reactions, particularly in relation to the development or worsening of anxiety, psychiatric and bipolar symptoms and tics as well as palpitations, exertional chest pain, unexplained syncope, dyspnoea, or other symptoms suggestive of heart disease (see Section 6 above). 14. Responsibilities of To monitor for the risk of diversion, misuse and abuse of methylphenidate Any suspected serious adverse reaction to an established drug should be reported to MHRA via the “yellow card scheme.” http://yellowcard.mhra.gov.uk/ all prescribers 15. Supporting documentation / information BNF Section 4.4 CNS stimulants Patient information leaflet for Ritalin: http://emc.medicines.org.uk/medicine/4093/PIL/Ritalin/ Patient information leaflet for Equasym: http://emc.medicines.org.uk/medicine/2695/XPIL/Equasym+5mg%2c+10mg+or+20mg+Tablets/ Patient information leaflet for Equasym XL: http://www.medicines.org.uk/EMC/medicine/15805/PIL/Equasym+XL+10+mg%2c+20+mg+or+30+mg+Capsules/ Patient information leaflet for Concerta XL: http://emc.medicines.org.uk/medicine/19551/XPIL/Concerta+XL+27+mg+Prolonged-Release+Tablets/ MHRA’s Drug Safety Update (March 2009): http://www.mhra.gov.uk/home/groups/pl-p/documents/publication/con041213.pdf EMEA’s Questions and Answers on the review of medicines containing methylphenidate (Jan 2009): http://www.emea.europa.eu/pdfs/human/referral/methylphenidate/MethylphenidateQ&A_65828508en.pdf FDA Drug Safety Communication: Safety Review Update of Medications used to treat Attention-Deficit/Hyperactivity Disorder (ADHD) in children and young adults (November 2011): http://www.fda.gov/Drugs/DrugSafety/ucm277770.htm “A large retrospective cohort study in children and young adults (aged 2-24 years) did not show an association between use of ADHD drugs and cardiovascular events, which include MI, stroke or sudden cardiac death. These study results were not consistent with the increase in sudden death estimated in a previous study, however a small to modest increase in risk cannot be excluded.” Safety Review Update of Medications used to treat Attention-Deficit/Hyperactivity Disorder (ADHD) in adults (December 2011): http://www.fda.gov/Drugs/DrugSafety/ucm279858.htm This Shared Care Protocol should be read in conjunction with the Summary of Product Characteristics Status: APPROVED Issue Date: July 2005 (Updated Dec. 2011 & Jan. 2014) Approved by: GPMTC 27th July 2005 Page 6 of 7 Review Date: January 2015 Shared Care Agreement Form CONSULTANT REQUEST To: Dr. Your patient: NHS No. (10digit): was seen on: with a diagnosis of: I recommend that methylphenidate is initiated (specify formulation): This drug has been accepted as suitable for shared care by the ABHB MTC. I agree to the responsibilities set out in the protocol SCP No. 10 (copy attached and at: http://www.wales.nhs.uk/sites3/page.cfm?orgid=814&pid=38180) I am requesting your agreement to sharing the care of this patient. The preliminary tests set out in the protocol have been carried out. I am currently prescribing the stabilising treatment. I would like you to undertake treatment from: The initial treatment will be: The baseline tests are: If you undertake treatment I will reassess the patient in ____ weeks. You will be sent a written summary within 14 days. I will accept referral for reassessment at your request. The medical staff of the department are available at all times to give you advice. Consultant Name: Signature: Department: Hospital: Date: Contact Telephone Nos: GP RESPONSE (Please circle the appropriate number below detailing your response) 1. I am willing to undertake shared care as set out in SCP No. _____ for this patient. 2. I would like further information. Please contact me on: _______________________ 3. I am unable to undertake shared care for this patient because: (Please state) _________________________________________________________________________________ G.P. Signature _________________________________________ Date _________ Practice Address/Stamp ________________________________________________ PLEASE RETURN WHOLE COMPLETED FORM OR A COPY TO THE REQUESTING CONSULTANT WITHIN 1 WEEK This Shared Care Protocol should be read in conjunction with the Summary of Product Characteristics Status: APPROVED Issue Date: July 2005 (Updated Dec. 2011 & Jan. 2014) Approved by: GPMTC 27th July 2005 Page 7 of 7 Review Date: January 2015